
Abstract
Background:
To date, there remains a paucity of present-day literature on the topic of demographics and the biopsy-proven pathological positivity rate of endometriosis.
Objective:
The goal of this study was to explore the association between patients’ demographics and other concomitant gynecological conditions or procedures and the pathological positivity rate of excision of endometriosis.
Design:
Retrospective cohort study.
Methods:
All women >18 years old who underwent laparoscopic surgery for endometriosis at a tertiary care hospital from October 2011 to October 2020. Women were classified into two groups: (1) Study group: women with >80% pathological positivity rate of endometriosis and (2) Control group: women with <80% pathological positivity rate.
Results:
A total of 401 women were included in the analysis. No difference was noted in the 80% pathological positivity rate based on body mass index [BMI; 68.7% in normal BMI versus 80% in underweight, versus 74.5% in overweight, and 74.1% in obese patients (p = 0.72)]. The percentage of patients reaching 80% pathological positivity of endometriosis was lower in women who had undergone previous laparoscopy for endometriosis compared to surgery naïve women (66.5% versus 76.5%, p = 0.03). In addition, a higher percentage of women who underwent concomitant hysterectomy (83.5% versus 68.8% for non-hysterectomy, p = 0.005) or bilateral oophorectomy (92.7% versus 70.0% for non-oophorectomy, p = 0.002) reached 80% pathological positivity. Women with an associated diagnosis of fibroids (79.7% versus 70.5%) or adenomyosis (76.4% versus 71.7%) were more likely to reach 80% pathological positivity compared to women without any other coexisting pathology; however, the observed differences were not statistically significant. After applying a log-binomial regression model, compared to White non-Hispanics, Hispanic patients were 30% less likely to reach 80% positivity (RR: 0.70, 95% CI: 0.49–1.02), although not statistically significant.
Conclusion:
No significant racial difference was found when comparing the rates of 80% pathological positivity of suspected endometriosis lesions among groups. Endometriosis pathological positivity rate was unaffected by patients’ BMI and the presence of concomitant pathologies. In addition, prior laparoscopic surgery for endometriosis might cause tissue changes that result in a decrease in the observed pathological positivity rate of endometriosis lesions during subsequent surgeries.
Precis
Endometriosis pathological positivity rate was unaffected by the patient’s race, BMI, and the presence of concomitant gynecological pathologies. Women who underwent previous surgery for endometriosis were less likely to reach an 80% pathological positivity rate.
Introduction
Endometriosis is an estrogen-dependent chronic inflammatory disease, defined as the presence of ectopic endometrial tissue. 1 The disease hinders the quality of life among pre-menopausal women, affecting 2–10% of women of reproductive age, 20–50% of infertile women, and 30–80% of women with chronic pelvic pain.2,3 To date, immunologic, serum, and genetic markers for endometriosis are not sufficiently sensitive or specific, 4 yet women benefit from a definitive diagnosis as it provides the language in which they can discuss their condition and seek earlier treatment to improve their quality of life. 5 Laparoscopy with histopathological confirmation remains the gold standard for the diagnosis of endometriosis,6–8 allowing for the visual identification of lesions within and outside the pelvis. 7 Laparoscopic diagnosis is a practice that remains challenged by the diversity of lesion appearance, 7 inaccessible lesion location as seen with deep infiltrating endometriosis, and surgeon observation variability. 9
Historically, endometriosis has been described as having increased prevalence within non-minority patients with high socioeconomic status.10,11 To date, prevalence studies have investigated this relationship with the most common finding of a lower prevalence among Black non-Hispanic versus White non-Hispanic women. 10 There remains a paucity within present-day literature on the topic of race and the biopsy-proven pathological positivity rate of endometriosis. The objective of this study is to investigate the association of pathological positivity rate of endometriosis excision in women with race/ethnicity, body mass index (BMI), concomitant gynecologic conditions, and prior surgical history.
Materials and methods
This is a retrospective cohort study conducted at a tertiary care hospital after obtaining institutional review board approval. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Records were obtained from the pathology department of all patients above 18 years of age with endometriosis on the final pathological report following laparoscopic surgery performed between 1 October 2011 and 1 October 2020. All the charts were screened for possible inclusion in the study. All patients who underwent laparoscopy whose primary diagnosis/indication was to evaluate for endometriosis were included in the study. Patients who underwent open surgery or whose primary indication for surgery was not endometriosis and those with coexisting premalignant or malignant conditions were excluded. Procedures performed by surgeons who had completed general Ob/Gyn training and those who had subspecialized within the field were included. Procedures performed by non-gynecologic surgeons were also excluded. A total of 972 cases with a pathological report stating endometriosis were reviewed. Among these, 571 were excluded (Figure 1). A total of 401 patients were included in the study.

A flowchart of the inclusion and exclusion criteria.
The pathological positivity rate was calculated as the number of lesions positive for endometriosis via pathology divided by the total number of lesions biopsied. The number of biopsies taken was dependent on each case and was specifically directed via surgeon identification of abnormalities. The data extracted and collected from the medical records included patient’s age, ethnicity, race, BMI, parity, history of prior gynecological procedures, type of laparoscopic procedure performed in the operative note of interest, surgeon, surgeon specialty, number of endometriotic lesions biopsied, the presence of adenomyosis and fibroids in the pathology report, the presence of adenomyosis previously diagnosed via imaging, and prior medical or surgical management. The information collected from the pathology reports included the endometriotic biopsies, location of endometriotic biopsies, the presence of adenomyosis, and/or fibroids. This study focuses on peritoneal endometriosis lesions. BMI was defined by World Health Organization standards, and race categorization was obtained from previously available demographic data. Patients were also classified according to whether prior surgery for endometriosis or prior hysterectomy was done, concurrent hysterectomy and/or bilateral oophorectomy were performed, and whether fibroids and adenomyosis were diagnosed per pathological confirmation. We defined the threshold for pathological positivity rate for endometriosis as more than or equal to 80% of lesions positive on pathological evaluation within each case. Previous studies have shown negative pathology rates as high as 14% in patients undergoing diagnostic laparoscopy with chronic pelvic pain. 12 The specificity for visual appearance for endometriosis is reported to be around 83.1%; therefore, we chose a 20% cutoff to accommodate these findings. 13 To examine differences in positivity rates of endometriosis lesions, patients were classified as having reached (study group) or not having reached (control group) 80% positivity in pathological confirmation of endometriosis lesions. The study population was divided into two groups. The first group is the study group which includes the patients where the pathology results reached 80% positivity for endometriosis lesions excised. The study group is compared to the control group comprised of patients where the pathology results did not reach 80% positivity for the endometriosis lesions excised.
Statistical analyses
Demographic and clinical characteristics were compared between patients reaching and not reaching 80% positivity rate on their pathological evaluation. Continuous variables were expressed as mean and standard deviation or median and range and differences were compared using independent samples t-test. Categorical variables were expressed as counts and percentages. Missing data and implausible patient characteristics were assigned to a separate missing category and included in the regression model. Chi-square tests were used to assess statistically significant differences. Statistical significance was set at an alpha level of 0.05.
Log-binomial regression was used to explore the association between patient sociodemographic and clinical characteristics and reaching 80% positivity, presented as risk ratios (RR) and 95% confidence intervals (CI). Variables with p values ⩽0.20 in bivariate analysis were considered potential covariates for a multivariable log-binomial regression model. Subsequently, the Akaike information criterion (AIC) was used to select a parsimonious model among all possible models using the variables selected. The model with the lowest AIC was considered to exhibit the optimal fit and selected as the final model. All statistical tests were two-sided and considered significant at p < 0.05. Statistical analyses were performed with SAS Software, version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Patients in the 80% or greater endometriosis lesion pathology-positive group were older than patients in the <80% lesion-positive rate (34.2 years versus 32 years, p = 0.007) (Table 1). Among BMI categories, there were no significant differences in the distribution of patients who reached the 80% pathological positivity threshold. Most of the surgeries were conducted by reproductive endocrinologists (REI) or minimally invasive gynecologic surgeons (MIGS), accounting for a total of 63.3% of the study population compared to 30.9% of cases which were performed by general Ob/Gyns. Among patients for whom race and ethnicity were present in our record, the highest likelihood of reaching 80% pathologic positivity was seen in White non-Hispanics (74.1) followed by Black non-Hispanics (70.9) and Hispanics (50%) (p = 0.04). Women more likely to reach 80% pathological positivity did not have a prior laparoscopy for endometriosis (76.5% versus 66.5%, p = 0.03), had a bilateral oophorectomy at the time of surgery (92.7% versus 70.0%, p = 0.002), and underwent concomitant hysterectomy (83.5% versus 68.8%, p = 0.005). There was no statistically significant difference in the rate of 80% positivity comparing women with or without a prior hysterectomy. Although women who had an associated pathological diagnosis of fibroids or adenomyosis were more likely to reach 80% pathological positivity compared to women without any other coexisting pathology, these differences did not reach statistical significance. Among patients with preoperative suspicion of adenomyosis based on clinical history and imaging, 68.2% reached 80% pathological positivity for endometriosis compared to 72.8% of patients without a clinical diagnosis of adenomyosis (Table 1).
Demographic and clinical characteristics by whether 80% or more of lesions biopsied were positive.

Data are presented as means (standard deviation), or n (%) unless otherwise specified. Counts may not add up to the total because of missing data. Percentages may not add up to 100 because of missing data.
p Value from independent samples t-test (continuous variables) or chi-square/Fisher’s exact test (categorical variables). p Values <0.05 considered statistically significant (bold).
MIGS, minimally invasive gynecologic surgeons; REI, reproductive endocrinologists.
The results from the log-binomial regression model with the lowest AIC (best fit) are presented in Table 2. Increasing age of the patient was significantly associated with an increased risk of reaching 80% positivity (RR: 1.01, 95% CI: 1.01–1.02). Compared to White non-Hispanics, Hispanic patients were 30% less likely to reach 80% positivity (RR: 0.70, 95% CI: 0.49–1.02), although not statistically significant. Similarly, women with prior hysterectomy were less likely to reach 80% positivity (RR: 0.79, 95% CI: 0.58–1.09). Having a prior surgery for endometriosis was significantly associated with a decreased risk of reaching 80% positivity (RR: 0.85, 95% CI 0.75–0.96) (Table 2).
Relative risks and 95% CIs for the association between patient characteristics and reaching 80% positivity in pathological confirmation of endometriosis lesions.
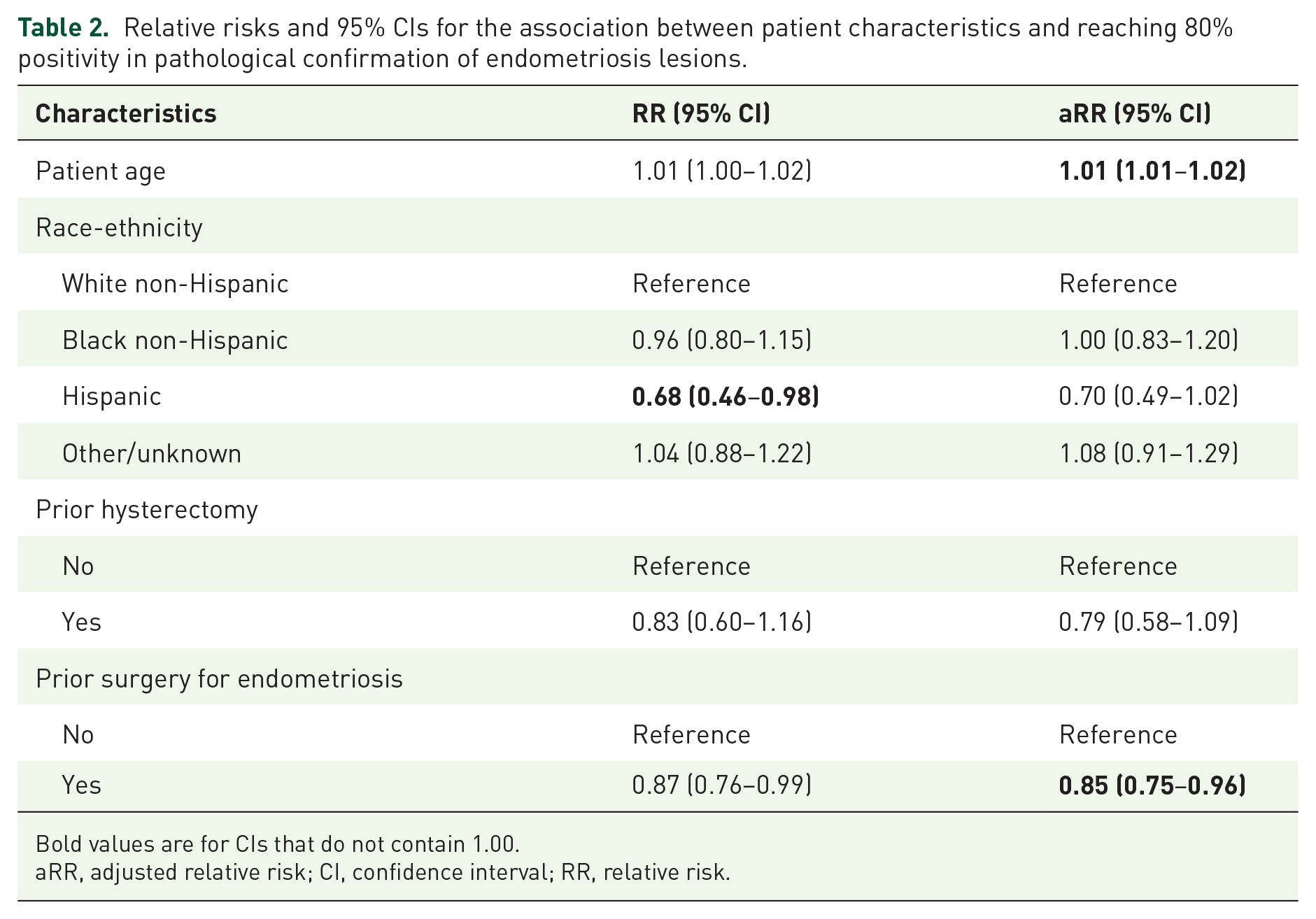
Bold values are for CIs that do not contain 1.00.
aRR, adjusted relative risk; CI, confidence interval; RR, relative risk.
Discussion
In this retrospective study, we found that among patients with clinical suspicion of endometriosis who underwent laparoscopy, the proportion of patients reaching ⩾80% pathological positivity rate of endometriosis excision was highest among older patients and patients who underwent concomitant hysterectomy and/or bilateral oophorectomy. Endometriosis is often regarded as mainly affecting patients between ages 20 and 40. Studies have demonstrated that endometriosis remains a top differential for pelvic pain in older patients as the severity and stage of the disease appear to increase from adolescence until the fourth decade when symptoms escalate and prompt surgery. 14 In Haas et al.’s 15 retrospective epidemiological studies, a total of 16,969 patients (40.33% of the study population) admitted to the hospital and treated for endometriosis were over age 40. It was noted that the proportion of patients reaching the 80% pathological positivity threshold was lower in patients who had prior surgery for endometriosis suggesting that prior surgical intervention might cause tissue alterations, resulting in the under-detection of endometriosis during subsequent surgeries or reduce the likelihood of recurrence.
According to endometriosis prevalence theory, the incidence of endometriosis was higher among White, middle-class women who had put off childbearing. 11 Bougie et al. 10 also reported in a meta-analysis that endometriosis is less commonly diagnosed amongst Black non-Hispanics and Hispanics, compared to White non-Hispanics. This conclusion neglects to account for the impact of socioeconomic status and barriers to healthcare access for patients of a certain race. In our study, since White non-Hispanic women were found to not have a statistically significant difference in rates of 80% pathologic positivity rates compared to Black non-Hispanic and Hispanic women, this suggests that, in fact, they have similar rates of diagnosis of endometriosis when surgery is performed. The difference in rates of diagnosis shown in prior studies between White non-Hispanics and minority groups may be explained by a combination of social factors that prohibited minority groups from achieving definitive diagnosis and care as White non-Hispanic women may recognize pelvic pain or infertility earlier as a health concern and obtain access to excellent diagnostic and treatment facilities. 16
Our study shows that the 80% pathological positivity rate of endometriotic lesions in women undergoing reoperation was lower than laparoscopy naïve patients. There are several possible explanations for this observed difference, the first being that patients with previous surgery are more likely to have pelvic adhesive disease which can influence the surgeon’s visualization and ability to accurately identify endometriotic lesions. 17 In addition, fibrosis may make the excision of suspected lesions more difficult, and as a result, surgeons may choose not to excise them. Among women, adhesions are thought to contribute to pelvic pain and dyspareunia,18–20 leading to additional surgeries that are less likely due to endometriosis. 20
Another significant finding our study showed was that women who underwent hysterectomy and oophorectomy during their laparoscopic procedure were more likely to achieve an 80% pathological positivity rate. This finding likely relates to the anatomic location of endometriosis, with the ovary being the most frequent site accounting for 54–66% of all lesions.21–23 Rizk et al. 24 showed that ovarian conservation carries a 6.1-fold risk of recurrent pain and an 8.1-fold risk of reoperation. Shakiba et al. 25 similarly showed that 19.2% of women with ovarian preservation after hysterectomy required reoperation versus 8% who underwent initial bilateral salpingo-oophorectomy. The removal of the uterus and ovaries during laparoscopy likely captures patients with extensive disease requiring complete hysterectomy and hence pathology samples had more endometriosis lesions detected. This intervention decreases the rate of recurrence and need for reoperation compared to initial resection. 26
Our study showed that concomitant gynecologic diagnoses, including adenomyosis and leiomyomas, were not associated with a significant difference in pathological positivity rate. Previous studies have described that uterine fibroids were detected in 25.8% of patients with endometriosis. 27 Further studies with larger populations to increase data power could elucidate whether there is in fact a difference. In patients with chronic pelvic pain, dismissing the diagnosis of endometriosis during surgical intervention for leiomyomas may lead to suboptimal treatment. 28
Strengths of the study include the availability of detailed clinical data regarding operative notes with biopsy information and associated pathology reports with histopathological description. In addition, our findings are based on biopsy-proven endometriosis, specifically confirmed by histopathology and its correlation with race and other existing pathology. One limitation of our study includes that any patients who underwent a surgical approach other than laparoscopy were excluded, thereby eliminating patients who could have potentially been of different races who at times are more likely to have open cases. 29 There is concern that Black non-Hispanic patients are misdiagnosed preoperatively with abnormal uterine bleeding and pelvic pain assumed exclusively due to leiomyomas which decreases the preoperative concern for endometriosis. 30 Our study excluded patients whose primary indication for surgery was not endometriosis, thus potentially missing minority patients with coexistent endometriotic lesions.
Conclusion
In summary, no significant racial difference was found when comparing the rates of 80% pathological positivity of suspected endometriosis lesions. BMI subgroups and a concomitant diagnosis of leiomyoma or adenomyosis did not show any significant differences in pathological positivity rates. In addition, prior laparoscopic surgery for endometriosis might cause tissue changes that decrease the pathological positivity rate of endometriosis lesions.