
Abstract
Human growth hormone has found favour as a co-gonadotrophin in assisted reproduction particularly in the circumstances of a poor response to stimulation. Its use has been based on animal studies suggesting insulin-like growth factor-1 enhances granulosa and cumulus cell function and possibly oocyte quality. While there is limited ovarian cellular information in women, the use of human growth hormone is alleged to improve egg numbers, embryo quality, clinical pregnancies and live birth in women with a poor ovarian response. A number of cohort studies have claimed these benefits compared with prior nil treatment, but there are a limited number of quality randomised controlled studies. The few good randomised trials indicate an enhanced ovarian response in terms of oestradiol secretion and oocyte maturity with controversial improvement in ongoing pregnancy and live birth. Given the cost of the medication, the lack of convincing data on enhanced clinical outcomes and the theoretical possibility of side effects, we propose it is still too early to determine human growth hormone’s true cost-benefit for widespread use. However, a number of emerging randomised trials may tilt the equation to a positive outlook in the future. Meanwhile, the hormone should only be used after full informed consent from the patient as to its effectiveness and efficacy.
Keywords
Introduction
The problem of poor ovarian response in assisted reproductive technology cycles is one that has vexed clinicians for many years and is becoming increasingly important as access to in vitro fertilisation (IVF) treatment expands, and women are increasingly seeking treatment at an older age. 1 The inability to garner large numbers of eggs in an IVF cycle leads to a reduced number of embryos being generated, and consequently a lower cumulative pregnancy rate per cycle overall. Attempts to increase egg numbers by using large doses of gonadotrophins and the relative lack of evidence for many adjuvants including dehydroepiandrosterone acetate (DHEA), androgens and antioxidants2–4 means that clinicians and patients continue to search for alternative therapies to boost ovarian response to treatment.
Human growth hormone has a long history of being investigated, and promoted, as a biologically active agent on the ovary5–12 and the hypothalamic pituitary axis (possibly through kisspeptin mediation). Its biological effects in natural puberty, growth and metabolism have been extensively described over several decades and long-term use for growth hormone deficiency has been generally shown to be both effective and safe.
As a result of these physiological observations, a confused literature has been developed about its role in improving IVF outcomes. 13 However, with numerous conflicting reports from cohort and randomised control trials, we still do not know the truth of whether this therapy is effective or not. Recently, in 2020, two quality meta-analyses were published with conflicting results based on the same data.14,15 Past and current Cochrane reviews on growth hormone use in poor responders continue to suggest this therapy may be effective in a subgroup of IVF patients with respect to ongoing pregnancy and live birth. 12
Adjuvant treatment with growth hormone is expensive, and of uncertain safety, and it would be expected that truth about its efficacy would be available before its widespread adoption in assisted reproduction procedures. This does not appear to be the case for a number of reasons we will discuss later. We attempt in this article to examine some of the reasons for the confusion that surrounds the evidence and discuss the latest interpretations of the data regarding the use of growth hormone for poor responders and poor ovarian reserve.
Definition of poor responders
One of the difficulties in interpreting the literature is that poor responders to IVF hormone stimulation have been defined in different ways. The first systematic effort to define women with poor response to stimulation as reflected in collected egg numbers was described in 2011, as the so-called
Advanced maternal age, greater than or equal to 40 years or any other risk factor.
A previous poor ovarian response with cycles cancelled, or less than three oocytes recovered.
An abnormal ovarian reserve test, including antral follicle counts, or anti-Mullerian hormone.
The Bologna Criteria have been criticised due to the heterogeneity of the population described and the recognition that many of these criteria need to be revised and substituted.
The current popular view for classification is the
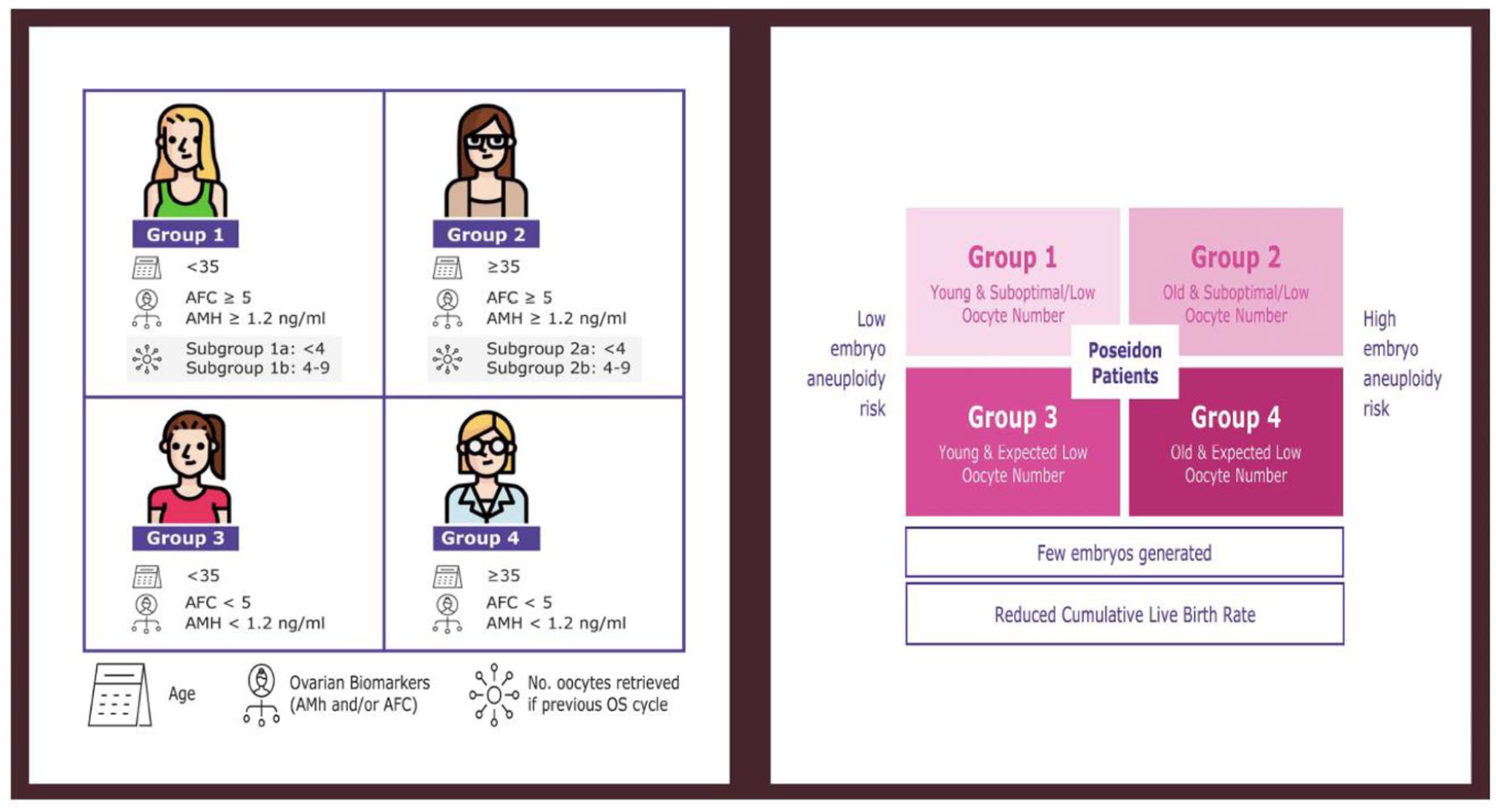
Poseidon criteria of low prognosis patient with assisted reproductive technology. Art drawing by Chloe Xilinas. 19
Review of the papers on the use of growth hormone frequently have not subdivided patients according to the Bologna or Poseidon criteria and have merely used clinical criteria based on poor ovarian response in previous cycles. It is difficult to determine the value of papers prior to 2011 because these criteria have not been used, and indeed some papers, including our own, 20 have not sought to classify any patient on these criteria, instead to try and replicate real-world clinical situations in which women have poor responses to gonadotrophin stimulation.
Overreliance on cohort studies by advocates of human growth hormone
There have been numerous studies that have claimed efficacy of human growth hormone based on cohort studies in individual or large clinics.8,21–31 Often these are before and after comparisons, either previous cycles or in previous time periods. This is well recognised to be a poor comparison given the lack of control for numerous other factors. Some of the main advocates for human growth hormone have utilised these potentially biased cohort studies to question any resistance to the belief that human growth hormone is effective in these cycles.8,9 It is hard to argue with a clinician who promotes patient experiences where in a number of cycles a pregnancy did not occur, followed by a success with human growth hormone where pregnancy did commence. Selection bias, changing clinical and laboratory techniques and increased clinical attention are alternative explanations. There is also an apparent publication bias towards positive outcomes from growth hormone therapy.
Poor quality and numbers of randomised controlled trials
There are relatively few randomised control trials, and certainly these are very heterogeneous including different descriptions of inclusion and exclusion criteria, blinding, use of placebo and methods of testing of the efficacy of the growth hormone administered.20,32–42 Every randomised controlled trial appears to differ in dose, length of treatment and appropriate blinding of patients, as well as the endpoints, with many emphasising the number of eggs and embryos obtained, rather than live birth. Some promote clinical pregnancy rather than birth of a healthy child. However, other included trials incorporate additional adjuvants to enhance response and there is heterogeneity of stimulation techniques and length of growth hormone use. The relatively small difference between placebo and treatment groups in the best trials suggests that very large numbers and a high financial cost is necessary to perform a definitive randomised trial to answer these questions. 20
Uncertainty about the action of growth hormone in the human ovary
Most publications on growth hormone action on the ovary have been in animal models where resulting insulin-like growth factor-1 (IGF-1) biological functions on the ovary have been well documented.10,11,43–47 While the rise in IGF-1 can be documented in the serum in women, there is little direct experimental evidence of its function in the human ovary in vivo and there is a much weaker biological plausibility for its effectiveness in improving granulosa and cumulus support of the oocyte. While there may well be a place for growth hormone in the patient with hypothalamic or pituitary disease,5,6,48 the evidence and biological plausibility for a direct action in the normal patient remains to be established.
Outdated and diverse systematic review and meta-analysis
The Cochrane Review for human growth hormone is out of date 12 (although a new one will be published within months) and systematic reviews and meta-analyses seem to give differing results. Clear advice for the practicing clinician and for the patient is lacking while non-evidence-based treatment using growth hormone is expensive and may be ineffective. In addition, there may be significant publication bias in that negative studies may not be reported and the difficulty in doing controlled studies due to the substantial expense of growth hormone added to an already expensive IVF cycle.
A recent meta-analysis of 12 randomised controlled trials (RCTs) included 536 women who received growth hormone and 553 who were in a control group. 14 A second analysis in the same year reported 15 RCTs with 1448 patients, highlighting the discrepancy between trial selection for analyses of this type. 15 According to Cozzolino and colleagues, whose literature search yielded 230 potentially relevant trials and 12 appropriate RCTs with 1139 patients, there were a number of problems that needed to be addressed to perform a meta-analysis. These included the following:
Different stimulation protocols, ranging from agonist to antagonist studies.
Different doses, and days of starting human growth.
Six studies, not providing information about the method of allocation and unclear and with an unclear risk of bias.
Lack of blinding of outcome assessments, half being high or unclear risk of bias.
Incomplete outcome data.
Selective data reporting.
Lack of power analysis in large numbers.
Poor recruitment, with some studies, ending early.
The results of the most two most recent systematic reviews and meta-analyses are shown in Figures 2 and 3 and overall these numbers are extremely small when trying to assess key parameters such as live birth rate.

Forest plot for outcomes of (a) live birth and (b) clinical pregnancy rate with human growth hormone as published by Yang et al. 15

Forest plot for outcomes of (a) live birth and (b) clinical pregnancy rate with human growth hormone as Published by Cozzolino et al. 14
Emphasis on the ovary rather than other targets of growth hormone
In recent years, there have been publications suggesting that human growth hormone may act on the endometrium and that purported benefits may occur through enhanced endometrial receptivity, rather than an effect on the ovary and the oocyte. 49 The same could be applied to the hypothalamic pituitary axis with various neuromodulators that may influence its secretion. Much of the data is based on animal studies and is highly speculative, but if growth hormone has any effect at all, it cannot be assumed that it is all entirely ovarian in nature.
Current evidence-based views of the role of human growth hormone
So, what can we conclude, regarding the role of human growth hormone in IVF cycles?:
1. Consistent effects of human growth hormone. Most studies suggest that the administration of human growth hormone produces
More oocytes and embryos which should theoretically increase the chance of achieving a pregnancy.
An earlier time to oocyte maturity which may suggest an improvement in the egg quality.
Probable increased oocyte competence and embryo utilisation.
Higher serum oestradiol levels prior to egg recovery.
An earlier time to egg pickup.
Lower gonadotrophin doses to achieve egg recovery.
These improved biological effects come at a financial cost however, with an estimation that growth hormone in addition to an IVF cycle could lead to double the expense for the stimulating drugs required for the patient. If the cost of growth hormone was lowered, this view could well change. The increased number of eggs, mature oocytes and embryos, does not, however, seem to be translated into an increased number for embryo transfer.
2. Unproven effects of human growth hormone.
There is some uncertainty about whether the clinical pregnancy rate is enhanced by growth hormone, with Cozzolino’s study 14 suggesting that the odds ratio was 1.34, with a lower margin of 1.02 and Yang and colleagues 15 claiming an odds ratio of 1.65 (CI: 1.31–2.08) (Figures 2 and 3).
There is no convincing evidence that live birth rate is increased with Cozzolino using the five randomised control trials where the relative risk was 1.34 (CI: 0.88–2.05) and Yang claiming eight studies with a value of 1.74 (CI: 1.19–2.54). Zhu and colleagues 50 studied 3080 patients with poor ovarian response in Beijing and showed no increase in live birth rate with growth hormone (OR: 1.27, CI: 0.88–1.85). The latest Cochrane review to be published, however, does suggest a benefit in live birth (personal communication). There is also uncertainty about whether more women achieve an oocyte retrieval in the growth hormone group, as opposed to those in placebo.
Selection of the most appropriate cases for growth hormone supplementation is in its infancy and not yet of clinical value. There would appear to be little value in measuring the hormone before treatment and stimulation tests of growth hormone secretion, such as the clonidine test, await validation.51,52
3. Lack of effect of growth hormone. It is widely accepted that the use of growth hormone does not improve outcomes in patients with a normal response to gonadotrophins undergoing an IVF cycle.
Conclusion
The role of human growth hormone for poor ovarian response remains as unclear as it has been over the past decade. Enthusiasts using cohort studies have promoted its use despite poor quality evidence and the considerable additional expense to the patient. Those who have relied on randomised control trials have not universally subcategorised poor ovarian responders to see whether there is a better chance in certain subgroups. Overall, there is no strong evidence of an increase in live birth rates (Figure 4). Given the expense of human growth hormone, the lack of convincing evidence for an improved meaningful clinical outcome and the potential complications, although small, of administering such a hormone in an IVF cycle seeking a pregnancy, there should not be a great deal of confidence that this treatment should currently be part of the repertoire of the practicing reproductive endocrinologist and infertility specialist. At present, the use of human growth hormone falls into the uncharted waters of adjuvant therapy for human reproduction and needs to be treated with significant caution. It is unlikely that a definitive trial will be available in the near future given the cost and difficulty of recruitment, and the uncertainty is likely to persist for a long time to come.

Network meta-analysis of the effectiveness of adjuvant treatments compared with controls on clinical pregnancy rates. 4