
Abstract
Background
In Ontario, Canada, province-wide initiatives supporting safer opioid prescribing in primary care include voluntary audit and feedback reports and academic detailing. In this process evaluation, we aimed to determine the fidelity of delivery and receipt of the interventions, the observed change strategies used by physicians, potential mechanisms of action, and how complementary the initiatives can be to each other.
Method
Semi-structured interviews were conducted with academic detailers and with physicians who received both interventions. Academic detailer interviews were coded using the Behavior Change Technique Taxonomy; physician interviews were coded to the Theoretical Domain Framework. Change strategies were summarized based on academic detailer intentions and physician-reported practice changes. Potential mechanisms of action were identified using the Theories and Techniques Tool and the literature. Patient partners informed the interpretation of results through ongoing group discussions of preliminary findings.
Results
Interviews were conducted with eight academic detailers and 12 physicians. Change strategies described by academic detailers to support physicians’ opioid prescribing included problem solving, instructions on how to perform the behavior, adding objects to the environment, credible source, shaping knowledge, and social support. Physicians mentioned that academic detailing validated current opioid practices or increased their belief about capabilities and their intentions, mediated by increased skills and the impact of environmental context and resources. Potential mechanisms of action included behavioral regulation, behavioral cueing, and general attitudes/beliefs. On its own, receiving the audit and feedback report did not lead to changes in beliefs about prescribing practices; however, for some physicians, it provided validation and reassurance. Physicians saw unrealized potential for complementarity.
Conclusions
New interventions are often implemented in a complex ecosystem with other competing interventions. In this study, we show how examining the fidelity of the intervention from initial design through to delivery can identify opportunities for potential optimization.
Plain Language Summary
Two large-scale programs that support safer opioid prescribing in primary care include an audit and feedback report and academic detailing (educational outreach). Although these two programs are effective in general, we aimed to help improve ongoing delivery.
Interviews with academic detailers (pharmacists trained to support physicians to implement evidence-based best practices regarding opioid prescribing) and family physicians who received both programs were conducted to understand how these programs impact opioid prescribing. Physicians said that academic detailing either changed the way they prescribed by increasing their confidence and intentions to safely prescribe opioids more generally or validated their current prescribing practices. Physicians reported that academic detailing improved how they communicated with their patients about opioids. Although physicians did not say they changed their behavior after receiving the audit and feedback report, the report did provide physicians reassurance about how they were prescribing opioids.
When asked about how these two programs worked together, academic detailers saw challenges, while physicians saw potential. This difference in opinion highlights the importance of considering how a new program fits within the system from the perspective of the developers, the recipients, and those impacted by the program.
By examining both programs in detail, we identified if/how each program led to physician behavior change and suggestions for improvement. When designing new programs, and informing ongoing delivery, knowing how the program changed from initial design to final delivery can help identify opportunities for improvements.
Keywords
Introduction
There has been a steady increase in opioid-related harms (Public Health Ontario, 2023). Canadians are among the world's largest consumers of prescription opioids (Hatt, 2022), and physicians play a central role in addressing this issue. In response to this complex crisis, healthcare improvement organizations have been implementing province-wide interventions that support safer opioid prescribing in primary care, particularly in Ontario, Canada, one of the provinces most affected by the crisis (Gomes et al., 2018). One of these interventions, received by over 3,000 physicians as of December 2020, is an audit and feedback (AF) report led by Ontario Health, the provincial advisor on quality in healthcare (Ontario Health, 2023). In AF, performance of a clinician or a clinical team is measured (audited), compared to a standard or target, and then reported back (feedback) with evidence-informed change ideas and resources (Brehaut et al., 2016; Ivers et al., 2012). Another provincial intervention is an academic detailing (AD) service led by the Centre for Effective Practice, an independent not-for-profit organization supporting behavior change in primary care (CEP, 2023). AD involves a trained pharmacist conducting a series of visits with a primary care physician to discuss how to implement evidence-based best practices. For this work, best practices focused on opioid and chronic pain-related topics, with resources provided to support improvements in care for patients with chronic non-cancer pain. This intervention had been delivered to around 800 physicians by February 2020. As both interventions were already used across the province, it provided a unique opportunity to study both interventions to understand fidelity from initial design to final delivery. AF and AD interventions are effective in general; it is unclear how to maximize their effectiveness (Ivers et al., 2012; O’Brien et al., 2007). It was anticipated that a deeper understanding of fidelity of each intervention, and the potential for the interventions to be complementary, could support optimization of both programs.
In partnership with Ontario Health and the Centre for Effective Practice, a quasi-experimental quantitative evaluation (Cook & Campbell, 1979) was conducted on the effectiveness of these interventions (alone and in combination) on opioid prescribing, using routinely collected administrative data. The evaluation found no significant change to opioid prescribing in the total group of physicians. The greatest significant reduction was seen in top prescribing physicians who received the AF intervention (Lacroix et al., 2024). To complement these results and inform improvements to ongoing delivery, we conducted a multi-method process evaluation. Process evaluations are designed to increase understanding of how an intervention functions within context and can provide direction on optimization (Skivington et al., 2021).
The first phase of the process evaluation included a document analysis and interviews with the AF report and AD developers to determine the intended mechanisms of action (MoA) that would lead to physician behavior change (McCleary et al., 2023). In the second phase, presented here, our primary objective was to determine the fidelity of delivery and receipt of the interventions, along with the observed change strategies and potential, yet unrealized, MoA. Our secondary objective was to establish if the AF report and AD could be complementary to support physician opioid prescribing. Figure 1 summarizes the evaluation.

Summary of the full process evaluation, which began with document analysis and interviews with intervention developers. The results from the darkest colored boxes are presented separately (McCleary et al., 2023)
Method
Study Design
Within the process evaluation, semi-structured telephone interviews were conducted with academic detailers who delivered AD and with primary care physicians who received the AF report and AD visits.
Context
This study took place in Ontario, Canada, where primary care physicians (typically family physicians) prescribe the largest total volume of opioid medications. These physicians see patients without co-pay or deductible and represent the first point of contact for patients within the healthcare system.
Interventions
Ontario Health MyPractice: Primary Care Report
Since 2013, every 6 months, all physicians in Ontario who had voluntarily registered electronically received the AF report, which provided information about their practice, including prescribing and screening rates across a variety of clinical topics. Individual trends in each performance indicator were compared to peers and “change ideas” were included with links to educational resources and practice-based tools to support quality improvement. The AF report is confidential and is not used for performance management. In 2017, four opioid prescribing indicators pertaining to non-palliative care patients were added to the report (see Table 1). A full mock report from 2020 is included in Supplement 1 with the updated version available online (Ontario Health, 2023).
Primary Indicators From the Audit and Feedback Report As Well As Visit Topics From Academic Detailing

The Centre for Effective Practice's AD Service
In 2018, the Centre for Effective Practice was funded by the Ontario Ministry of Health to deliver AD to primary care physicians across Ontario, focused on safer opioid prescribing and management of chronic non-cancer pain. Physician recruitment focused on regions with higher opioid prescribing rates and involved cold calls by academic detailers and warm introductions from local primary care leads. The intervention was delivered by trained pharmacists (academic detailers) who visited primary care physicians in their practice to deliver up to three educational outreach visits. Visit details in Figure 1.
Academic detailers are trained on the content and delivery of the detailing and provided with many documents to support each visit, including step-by-step guides for specific actions, screening tools, patient handouts, communication tools, and lists of local resources. Example tools are in Supplements 2 and 3.
Theoretical Frameworks
The guiding theoretical frameworks included the Theoretical Domain Framework (TDF), and individual Behavior Change Techniques (BCTs) (Michie et al., 2013). The TDF synthesizes 33 theories of behavior change and 128 corresponding constructs into 14 domains that may influence healthcare professionals’ behavior (Cane et al., 2012; Michie et al., 2005). A BCT is a specific strategy used in interventions to change behavior by targeting psychological or environmental mechanisms that influence how people act (Michie et al., 2013). MoAs refer to the processes through which an intervention influences behavior (Carey et al., 2019). Previously, we identified intended MoA based on interviews with those who designed the interventions (McCleary et al., 2023). In this paper, we add potential, yet unrealized, MoAs to be considered to further optimize the interventions. These unrealized MoAs are identified using the Theory and Techniques Tool (TTT), which was developed based on 277 behavior change intervention articles and a series of expert consensus processes. The TTT highlights techniques that may be best placed to help overcome specific barriers to change (Carey et al., 2019; Theory and Techniques Tool, 2024).
Sampling and Recruitment
Academic detailers delivering AD, and family physicians practicing in Ontario who had received AD and AF, were recruited to participate in an individual telephone interview. Based on the quantitative findings, the sampling frame was 5,925 physicians, but only 245 (4%) received both the AF report and AD (Lacroix et al., 2024). We aimed to speak with academic detailers with the largest caseloads, those who conducted visits to any family physician in their area, and those who conducted visits within their own Family Health Team (i.e., with their practice colleagues). The Centre for Effective Practice provided email addresses and availability of eligible academic detailers. NMc then obtained informed consent and conducted the interviews. All academic detailer interviews were conducted between April and June 2019.
Physician recruitment was conducted in phases, interrupted by the COVID-19 pandemic. In February 2020, a recruitment email was sent by the Centre for Effective Practice to physicians across Ontario who had participated in at least one visit focused on opioid tapering, chronic non-cancer pain, or opioid use disorder. Recruitment was then paused until February 2021 when they emailed any physician who had met eligibility criteria since the previous recruitment email. For Ontario Health, initial recruitment in February 2020 was through a recruitment question in an evaluation survey sent to all physicians who received the report. Recruitment was restarted in July 2021 with specific recruitment emails sent by Ontario Health in two batches (∼500 per round). Recruitment e-mails from both organizations highlighted the eligibility criteria of needing to have participated in both interventions. No other recruitment restrictions were applied. All physician interviews were conducted between February and December 2020.
Data Collection
A semi-structured interview guide for the academic detailers was informed interviews with AD developers (McCleary et al., 2023). Academic detailers were asked to describe the process of conducting a visit, as well as whether and how they used each of the specific detailing materials. The interview guide for physicians was designed to unpack the extent to which the physicians received and engaged with both the AF report and AD visits; the perceived influence of the initiatives on their prescribing behaviors; and if/how the initiatives could be complementary. Barriers and enablers to implementing safer opioid prescribing practices were explored, such as tapering regimens for those at high risk (Ceasar et al., 2016; Owston, 2016; Trafton et al., 2010). A subset of TDF domains were included in the interview guide based on previous research (Desveaux et al., 2019). Interviews were conducted by NMc (academic detailers) and NK (physicians), neither of whom had any prior relationship with the participants. Academic detailers did not receive remuneration; physicians received a $100 gift card.
Analysis
All interviews were audio-recorded and then transcribed verbatim. Similar methodology was followed for both sets of interview analysis, with an initial coding framework developed for each set. Two researchers (NMc and CL for academic detailers; NK and TS for physicians) independently coded the first two interviews in each set to inform development of the codebooks, which consisted of a coding scheme and decision rules to facilitate consistent coding of the remaining interviews (Thompson et al., 2004). Academic detailer coding included BCTs (Michie et al., 2013) used to support practice change, while the physician codebook used the TDF. Inductive coding was applied in both sets of interviews to generate themes not captured within the a priori codes. Coders met regularly to refine the themes, with input from the wider team, which included individuals with lived experience. These Lived Experience Advisors provided their perspective on identified themes and their interpretation of specific physician quotes. NVivo 11 (QSR International) qualitative software was used. For physician interviews, an additional analysis was conducted by NK to specify if the physician was discussing the AF report or AD visits.
BCTs identified in academic detailer interviews were mapped to TDF domains identified in the physician interviews and then mapped to the MoA identified within the TTT to identify potential, yet unrealized, MoA to be considered to optimize the interventions.
Results
Interviews were conducted with eight academic detailers and 12 physicians. Academic detailers had been practicing pharmacists for an average of 14 years (range 5–25 years), 37.5% (n = 3) had prior experience as an academic detailer, 50% (n = 4) concurrently worked in a Family Health Team, with three of the four being the academic detailer for their Team. Academic detailer interviews lasted between 36 and 55 min (M = 48 min). BCTs described by academic detailers to support safer opioid prescribing by physicians included problem solving, instructions on how to perform the behavior, adding objects to the environment, credible source, shaping knowledge, and social support.
Physician interviews lasted 29–59 min (M = 42 min). Half of the physicians were female (n = 6), with an average age of 43 years, having been practicing for 2–37 years, with an average of 9.5 years in the current clinic (Table 2). Ninety-two percent (n = 11) of physicians were in primarily capitation payment models. The AF did not change physician's self-perceived prescribing practices; however, for some, it provided reassurance and validation of their current opioid prescribing. AD validated current opioid practices or increased physicians’ belief about capabilities and their intentions, mediated by increased skills and the impact of the environmental context and resources. This validation by either intervention was a positive effect if the physician was already prescribing in a way that aligned with best practice or could be a negative if it validated unsafe prescribing practices.
Demographics of Physicians Interviewed
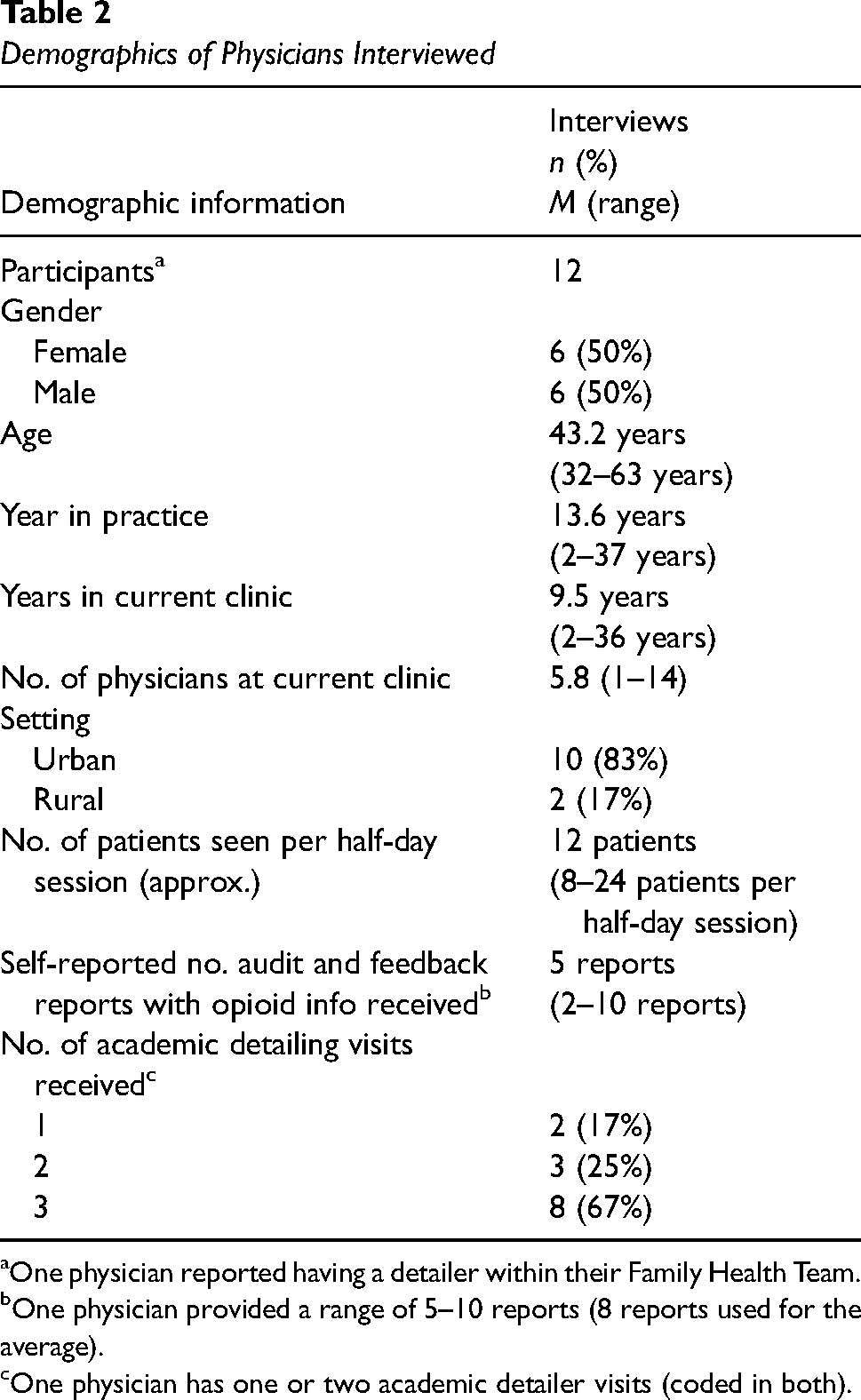
One physician reported having a detailer within their Family Health Team.
One physician provided a range of 5–10 reports (8 reports used for the average).
One physician has one or two academic detailer visits (coded in both).
There was alignment between how the academic detailers intended to support physicians in changing their behavior and how physicians discussed their change, although practice change was also mediated by system factors (environmental context and resources). Potential, yet unrealized MoAs, as identified using the TTT, included behavioral regulation, knowledge, behavioral cueing, general attitudes/beliefs, attitude toward the behavior, and social influence. Academic detailers mentioned that the AF report and AD visits could be somewhat complementary but saw significant challenges. Physicians saw strong potential for the interventions to be complementary, saying that each intervention had a unique way to support them in addressing this complex crisis.
Academic Detailer Interview Responses
Delivery of AD Visits
Academic detailers were trained on clinical content and delivery methods, and there was a sequence to a typical visit (Table 3). As topics were complex and controversial, the information had to be actionable and tailored for the physicians, with materials used to support, not drive, the conversation. As the academic detailer was not typically in the circle of care, specific patients were not discussed; however, case examples were used to provide actionable strategies that aligned with the evidence.
Steps Typically Followed by an Academic Detailer During an Academic Detailing Visit

How Academic Detailers Reported Supporting Physician Behavior Change
When probed about the behaviors that physicians should be able to enact following a visit, the academic detailers mentioned specific behaviors related to the three visit subtopics. Since each visit was adapted to physician needs, the specific behavior targeted varied visit to visit. However, all academic detailers discussed their goal of supporting physicians to safely prescribe opioids (i.e., the overall behavioral target as mentioned in Table 1). BCTs identified in the academic detailers’ descriptions of strategies used to encourage change included problem solving, instructions on how to perform the behavior, adding objects to the environment, credible source, social support (unspecified), and an additional theme focused on shaping knowledge. Details are in Table 4.
Behavior Change Techniques Used by Academic Detailers to Support Safe Opioid Prescribing by Physicians

Note. AD = academic detailer.
Problem Solving
Aligned with adapting to physician needs, problem solving was the most common strategy as academic detailers supported physicians to work through case examples, talked through specific situations, and provided strategies for conversations which the physicians had indicated they found more challenging. Academic detailers typically recommended “Talking Points,” which provided specific phrases for physicians to use. These points were developed by the Centre for Effective Practice in consultation with primary care providers and persons with lived experience to be better aligned with patients’ needs. “I give it [Talking Points document] to all the physicians actually, whether they ask for it or not because usually it's [using appropriate language] a challenging piece for all physicians” (AD 3).
Instructions on How to Perform the Behavior and Add Objects to the Environment
Both BCTs were a frequent part of the visit. Instructions were provided based on the request of the physicians, supported by evidence-based tools and guidelines. The detailing materials provided a lot of information regarding specific steps and the academic detailer worked with the physician to see how and when these steps and tools could be applied. Some of the tools were designed to be embedded in the electronic medical record system or could be used directly with a patient. For example, the tool generally referred to as the “four-tire analogy” (Supplement 3) helped explain how multiple pharmaceutical and non-pharmaceutical options were needed in the management of chronic non-cancer pain, akin to needing air in all four tires of a car. This tool could be used by physicians when talking to patients as either a physical tool (an object added to their environment) or explained orally.
Credible Source
Having the academic detailer seen as a credible source was said to facilitate visits and physician engagement. Academic detailers mentioned that the physicians trusted that the materials were evidence-based and appreciated that although this style of visit was better known to be delivered by pharmaceutical representatives, there was no commercial interest from the organization or the academic detailers. “If we did not come off credible, they [the physician] would not come back for a second visit” (AD 2).
Shape Knowledge
The academic detailer also used the tools and conversations to shape physician knowledge, often working through questions raised by physicians about the risks and benefits of opioids and the associated evidence base (i.e., knowledge-based question). Academic detailers also increased physicians’ knowledge of local supports and programs where physicians could refer their patients to help manage their pain.
Social Support
Overall, the social support mentioned to be provided through these visits was said to be a trusted source for physicians to speak with about this complex topic.
Physician Response to AD
Physicians appreciated the AD visits, particularly as the conversations were one on one and tailored to their needs. “The detailer was very open about or responsive to sort of directing the visit around particular issues that I might be facing” (Physician (P) 12). Physicians often mentioned wanting to discuss specific patients; however, as the academic detailer was not typically in the circle of care, only examples could be discussed. Physicians understood this limitation, yet felt it could be a disadvantage to the service. All physicians self-reported that the AD improved or validated their opioid prescribing practices.
Physicians Who Mentioned Improvement in Their Opioid Prescribing Practices Following AD
Among physicians who self-reported improvements in their opioid prescribing following the AD visits, this change was driven by improved beliefs about capabilities, represented as increased confidence, such as in tapering and speaking to their patients about the process. Physicians also mentioned increased intentions, represented as increased motivation, including to have, or retry, those conversations which physicians felt could be more challenging. All practice change was dependent on the environmental context and resources. Physicians mentioned difficulty in improving their practices due to lack of access to local services, such as a specialty clinic that was not accessible to patients who needed daily treatment. For some physicians, beliefs about capabilities and intentions were mediated by increased skills, as the physician tools and patient handouts were said to improve communication skills by the “Talking Points,” or how to taper by using the “Opioid Tapering Template” (Figure 2; Table 5).

Physicians who increased their beliefs about capabilities and their intentions to improve their opioid prescribing practices following visits from academic detailers were all mediated by system factors within environmental context and resources. For some physicians, the use of the tools and patient handouts improved their skills, which then increased their beliefs about capabilities and intentions. These practice changes were all leading to physician self-reported improvements in opioid prescribing
Impact of Academic Detailing on Physician Prescribing Practice by Domain of the Theoretical Domain Framework for Those Who Self-Reported Improvements

Note. P = physician.
Beliefs About Capabilities
Physicians mentioned feeling increased confidence in knowing that the strategies they were applying were evidence-based and in having clear directions on how to support their patients. Physicians also discussed increased comfort in talking to their patients about their opioid use. Physicians felt they were more in control of these conversations, which meant they could better support the patient, rather than making immediate referrals, such as to a pain clinic. “I felt like I had more control, that I could initiate the conversation and encourage change rather than kind of keeping things status quo” (P1).
Intentions
Intentions to improve prescribing practices increased. Academic detailer visits motivated physicians to try something different, such as using the Talking Points to approach conversations in a different way. Physicians mentioned being motivated to re-engage with patients where they felt they had not previously been able to provide appropriate support. “I felt like it motivated me to work harder with people on high doses of prescriptions” (P9).
Interactions
Belief about capabilities and intentions interacted with each other and were both impacted by environmental context and resources. System factors were typically viewed as health system issues that made appropriate prescribing more difficult. Even physicians who changed their practice (e.g., using new approaches for talking to patients) felt restricted by the lack of local support (access to Suboxone, physiotherapy, etc.), although AD provided information about additional options.
The use of tools and patient handouts was said to impact skills for some physicians, which mediated changes in beliefs about capabilities and intentions. Tools supported improvements in skills such as tapering, switching medication, and having more effective and patient-centered conversations with patients. The tools were typically praised by physicians, and some were integrated into physician workflow, such as being directly integrated into their EMR systems, and patient handouts used during appointments.
Physicians also mentioned using the Talking Points tool to improve their skills in discussing this complex topic with their patients, as did working through the four-tire analogy with their patients. “Some of the handouts, like the car with the four flat tires handout, things like that, that I use now all the time with my patients that I wasn’t using before” (P10).
Validating Physician's Current Prescribing Practices
Of the physicians who felt AD visit(s) validated their current practice, many mentioned already being aware and supportive of the information provided by the academic detailer. “I was already convinced that this was the way to go, so this has just reinforced what I already kind of knew” (P8). The visit was said to be a good review of material, and they appreciated the tools and handouts; however, it did not change their workflows or the way they interacted with patients. “I think I’m doing things okay. … [detailing was] just making sure and reminding us of all the things we should be doing or messaging or just tips and tricks of like and some fine tuning” (P11).
Some physicians reported increased intentions, which typically presented as increased motivation. However, for various reasons, including feeling they had already done what they could for their patients, and negative system factors previously discussed, this intention did not lead to changes in practice.
Observed Change Strategies and Potential MoA
Observed change strategies identified by academic detailers were mapped to TDF domains identified in the physician interviews and then compared to potential MoA identified within the TTT (Table 6). Potential, but unrealized, MoA based on the TTT included behavioral regulation, knowledge, behavioral cueing, general attitudes/beliefs, attitude toward the behavior, and social influence.
Observed Change Strategies Identified by Academic Detailers, Mapped to Change Mechanisms for Physicians Who Self-Reported Improvements in Practice and Potential Mechanisms of Action Identified Through the Theory and Techniques Tool

Note. AD = academic detailer.
Link identified in the Theory and Techniques Tool.
Link identified as inconclusive in the Theory and Techniques Tool.
Identified in the Theory and Techniques Tool, but not by the academic detailer or physician interviews.
Academic detailers mentioned using problem solving, including tailoring their visit to meet physician needs and working through case examples. Physicians recognized this tailoring and use of examples as part of increasing their beliefs about capabilities, such as by working through case examples, which also impacted on skills such as tapering and communicating with patients, while still impacted by environmental context and resources. Within the TTT, problem solving had been linked to beliefs about capabilities, with inconclusive evidence for environmental context and resources and skills. The TTT had evidence for behavioral regulation as another potential mechanism for problem solving.
Although social support was mentioned by academic detailers as a strategy for changing practice, physician behavior change did not appear to be driven by social influence. Physicians did not report to be changing their practice because of the interpersonal processes and the social interaction with the academic detailer. The combination of the academic detailer with the resources seemed to lead to physicians reporting changes in their prescribing practices, not solely the interaction with the detailer.
Physician Response to the MyPractice Report
Physicians mentioned opening the AF report at least once after the email prompt and reviewing the general trends for how they compared to themselves in previous reports and to others. Many physicians mentioned doing a more comprehensive review when there was a change since their last report, or if they were prescribing higher than others. Most physicians felt the report was useful, although a few mistrusted the data, felt their patients were different from others, and worried about high rates of prescribing by others. On its own, receiving the AF report did not lead to changes in beliefs about prescribing practices; however, for some, it provided validation and reassurance (Table 7).
Impact of the Audit and Feedback Report on Change in Physician Practice

Note. AF = audit and feedback; P = physician.
Physicians who felt that reviewing the report validated their practice typically already believed they were providing appropriate care. For them, the AF report was a good reminder, a validation of their current practice, and a reassurance. “It doesn’t change what I would do drastically, but it helps confirm if my thinking was on the right track or just give me some supporting reassurance” (P1). Other physicians were neutral to the report and did not mention feeling validated or reassured.
When asked about the “Change Ideas” page, which includes a list of suggestions and resources for making practice improvements (Supplement 1), many physicians mentioned already doing these suggestions. “I think they’re [Change Ideas] pretty straightforward as to things that I would normally be doing anyway” (P6).
Complementarity of Interventions
When asked about how the AF report and AD complemented each other, this was typically the first time either academic detailers or physicians had considered this question. Academic detailers and physicians did not usually discuss the AF report. Some academic detailers saw challenges in considering these together, particularly as they felt they already had a lot to cover and were skeptical about the AF report for including old or inaccurate data and difficulty when specific patients cannot be listed.
Many physicians felt the AF report could specify where improvement was needed, while the AD visit(s) could help make those improvements; both were needed to address this complex crisis. While reflecting on this question, some physicians concluded that it would have been quite helpful to bring up the report during their AD visit. “I think the reports are to tell you about your own practice, and then the detailing gives you kind of the general overview of how to do things. And now that I think about it, it might’ve been helpful if we had the reports for the detailing, which we didn’t do” (P7).
Reflections of Lived Experience Advisors
Throughout the analysis, the Lived Experience Advisors on the project team emphasized the need for further work to consider fidelity between intentions for the interventions and patient experience with physicians who have received them. Patient experience with the physician may not necessarily match the physician's belief about their capabilities. Physicians may believe they are communicating well with their patients, but patients may have different perspectives. For example, the “four-tire” tool (Supplement 3), shared often by detailers and used frequently by the physicians, was felt to be objectifying and lacking nuance. Individuals with lived experience might help improve the design of these interventions. Details on the perspectives of lived experience advisors in this project are elsewhere (Nicholas Angl et al., 2024).
Discussion
Interviews with academic detailers and physicians were conducted as part of a multifaceted evaluation to understand the impact of an AF report and/or AD on opioid prescribing by primary care physicians across Ontario, Canada. A linked publication explores the causal assumptions in the development and design of these interventions (McCleary et al., 2023). In this study, we show how examining the fidelity of the intervention from initial design through to final delivery can identify opportunities for optimization.
For AD, change strategies described by academic detailers to support safer opioid prescribing by physicians included problem solving, instructions on how to perform the behavior, adding objects to the environment, credible source, social support, and shaping knowledge. Of the physicians who reported they changed their behavior in response to AD, this was attributed to increased belief about capabilities and intentions, mediated by increased skills for some physicians, and environmental context and resources for all physicians. The AF report provided validation and reassurance to some physicians, but many reported no effect.
Interestingly, the process evaluation results differed from the quantitative evaluation, which found no significant change in total prescribing, and that the greatest significant reduction was in top prescribing physicians who received the AF intervention (Lacroix et al., 2024). Potential reasons for the discrepancy included that the focus of the AD did not directly align with the outcomes measured, and the perceived benefits of detailing (better communication with patients, increased problem solving, etc.) are not measured. Another reason may be due to sampling bias as physicians with the most room for improvement may not have agreed to an interview but could mean that the interventions themselves were not targeted to those with the most room for improvement. The data also looked at the impact of both interventions, yet the interventions were not coordinated and did not provide complementary support. Finally, physicians may not always know what leads them to change their behavior. These discrepancies highlight the importance of considering quantitative and qualitative results within process evaluations, as, on their own, the results may not present the full impact.
We observed fidelity between the intervention intentions and delivery, but variation in how physicians responded to the interventions. This variation aligns with the concept of “voltage drop,” which is particularly common for interventions delivered at scale, when there is a change from the initial design to actual delivery and receipt (Chambers et al., 2013). Context and environment played a strong role as patient roster, access to patient support services, and geographic location were all said to impact physician prescribing as well as their response to the interventions, which aligns with prior research (Desveaux et al., 2019; Gugala et al., 2022; Kennedy et al., 2019). There was a range of physician beliefs about capabilities, from those who mentioned extensive experience with opioid prescribing and were already highly capable, through those who mentioned that so few of their patients had an opioid prescription that the interventions were not relevant. As AD requires trained pharmacists, it may be worth considering having this resource reserved for physicians with higher potential or need for change, to maximize impact (Lacroix et al., 2023). This pool could include physicians with a higher number of patients with an opioid prescription or those with prescribing practices that differ from their peers. However, having a higher number of patients on an opioid prescription does not imply a clinical need for improvement nor the desire to improve.
AF literature recommends increasing actionability (Desveaux et al., 2021; Willis et al., 2022); co-interventions, such as AD, may be one approach to increase actionability. When asked to consider the two interventions together, academic detailers saw challenges while physicians saw potential. Physicians reported that both interventions potentially had unique but complementary roles in addressing this complex crisis, highlighting that future collaboration might increase impact, particularly for physicians with room for improvement. In intervention design, knowing how the intervention fits within the current context and in relation to other interventions is important (Baker et al., 2010; Damschroder et al., 2022; Murray et al., 2010); however, the differing perspectives we found between detailers and physicians further highlights the need to consider the perspectives of those delivering, receiving, and impacted by, the intervention.
Ontario Health anticipated that the AF report would provide physicians with a clearer understanding of their own prescribing patterns in comparison to others. Document mapping suggested behavior change would be driven by feedback on behavior and social comparison (McCleary et al., 2023). Physician interviews found that the AF report could validate or provide reassurance of current practice. The emphasis was on reflection (i.e., understanding physicians own prescribing data) and less about action, which aligned with the physician interview results. These results are also aligned with the Clinical Performance Feedback Intervention Theory, which emphasizes that the understanding of data is a key way that AF leads to change (Brown et al., 2019). As receiving the AF report was voluntary, there was an inherent bias in that many of the physicians receiving the report were already focused on quality within their practice and already had some knowledge of where and how to find resources and other practice supports.
Using the TTT to suggest potential new MoAs was a novel way to inform intervention delivery. Further work is needed to confirm if these potential, yet unrealized, MoAs could play a role in increasing effectiveness of these interventions. Crawshaw et al. identified the 10 most common BCTs used within randomized control trials that included AF (Crawshaw et al., 2023). Of these 10, three overlap with the AD MoAs; however, the seven additional MoAs mean the AF intervention may be complementary by adding several ways to support physician behavior change. These seven include feedback on behavior, social comparison, education (unspecified; created for the review), social support (practical), prompts/cues, discrepancy between current behavior and goal, and restructuring the social environment. The combined impact of these interventions is also difficult to articulate, since all physicians received the report and knew their process was being tracked; thus, it may have had more of an impact than would be found through interviews.
Limitations
We focused on self-reported change (or lack thereof); actual prescribing change of participants is unknown. MoAs could only be identified among physicians who reported they changed their practice. Physicians were predominantly from urban areas, half were in a Family Health Team, and 67% had received three or more AD visits. As such, interviewed physicians may have been more actively engaged with quality improvement efforts to improve their prescribing than other physicians. However, the insights from such physicians remain useful regarding missed opportunities for complementarity of the interventions.
As physician recruitment began in February 2020, the COVID-19 pandemic limited the number of physicians interviewed and recruitment ended due to recruitment challenges rather than data saturation. Since the opioid-specific detailing was conducted between March 2018 and March 2020, a long time passed between receiving the AD visit(s) and the interview; thus, physicians had difficulty remembering the specifics of the visits, making further recruitment futile.
To capture the impact on patient experience, a final phase included interviews with patients of interviewed physicians. The limited physician recruitment severely restricted our ability to recruit patients, and this project was cancelled. A separate study could explore the patient-level impact, particularly regarding the use of patient handouts and the Talking Points.
Conclusions
This theory-informed process evaluation of two large-scale interventions to improve opioid prescribing examined both interventions in detail to identify if/how these interventions led to perceived physician behavior change and ways to improve ongoing delivery. Physicians indicated AD increased’ belief about their capabilities and their intentions, mediated by increased skills and the impact of the environmental context and resources, or validated their current opioid prescribing practices. As AD requires the involvement of trained pharmacists, supporting physicians with more room for improvement may maximize effectiveness and efficiency. The AF report provided reassurance and validation to some physicians. Physicians saw strong potential for the interventions to be complementary. By fully exploring fidelity of the intervention designs through to their delivery and receipt, and exploring potential, yet unrealized, MoAs, this study helps inform potential strategies for improving ongoing delivery of two, large-scale, interventions.
Supplemental Material
sj-pdf-1-irp-10.1177_26334895241307638 - Supplemental material for Changing or validating physician opioid prescribing behaviors through audit and feedback and academic detailing interventions in primary care
Supplemental material, sj-pdf-1-irp-10.1177_26334895241307638 for Changing or validating physician opioid prescribing behaviors through audit and feedback and academic detailing interventions in primary care by Celia Laur, Natasha Kithulegoda, Nicola McCleary, Emily Nicholas Angl, Michael Strange, Barbara Sklar, Thivja Sribaskaran, Gail Dobell, Sharon Gushue, Jonathan M. C. Lam, Lindsay Bevan, Victoria Burton, Lena Salach, Justin Presseau, Laura Desveaux and Noah Ivers in Implementation Research and Practice
Supplemental Material
sj-pdf-2-irp-10.1177_26334895241307638 - Supplemental material for Changing or validating physician opioid prescribing behaviors through audit and feedback and academic detailing interventions in primary care
Supplemental material, sj-pdf-2-irp-10.1177_26334895241307638 for Changing or validating physician opioid prescribing behaviors through audit and feedback and academic detailing interventions in primary care by Celia Laur, Natasha Kithulegoda, Nicola McCleary, Emily Nicholas Angl, Michael Strange, Barbara Sklar, Thivja Sribaskaran, Gail Dobell, Sharon Gushue, Jonathan M. C. Lam, Lindsay Bevan, Victoria Burton, Lena Salach, Justin Presseau, Laura Desveaux and Noah Ivers in Implementation Research and Practice
Supplemental Material
sj-pdf-3-irp-10.1177_26334895241307638 - Supplemental material for Changing or validating physician opioid prescribing behaviors through audit and feedback and academic detailing interventions in primary care
Supplemental material, sj-pdf-3-irp-10.1177_26334895241307638 for Changing or validating physician opioid prescribing behaviors through audit and feedback and academic detailing interventions in primary care by Celia Laur, Natasha Kithulegoda, Nicola McCleary, Emily Nicholas Angl, Michael Strange, Barbara Sklar, Thivja Sribaskaran, Gail Dobell, Sharon Gushue, Jonathan M. C. Lam, Lindsay Bevan, Victoria Burton, Lena Salach, Justin Presseau, Laura Desveaux and Noah Ivers in Implementation Research and Practice
Supplemental Material
sj-pdf-4-irp-10.1177_26334895241307638 - Supplemental material for Changing or validating physician opioid prescribing behaviors through audit and feedback and academic detailing interventions in primary care
Supplemental material, sj-pdf-4-irp-10.1177_26334895241307638 for Changing or validating physician opioid prescribing behaviors through audit and feedback and academic detailing interventions in primary care by Celia Laur, Natasha Kithulegoda, Nicola McCleary, Emily Nicholas Angl, Michael Strange, Barbara Sklar, Thivja Sribaskaran, Gail Dobell, Sharon Gushue, Jonathan M. C. Lam, Lindsay Bevan, Victoria Burton, Lena Salach, Justin Presseau, Laura Desveaux and Noah Ivers in Implementation Research and Practice
Footnotes
Acknowledgments
The authors wish to thank Ontario Health and the Centre for Effective Practice for collaborating on this research and supporting the recruitment of physicians. Additional thanks to all academic detailers and physicians who participated in the interviews.
Authors' Note
Nicola McCleary is currently affiliated with Child Health Evaluative Sciences Program, The Hospital for Sick Children – Research Institute, Toronto, ON, Canada; and Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, ON, Canada.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GD, SG, and JL were employed by the organization administering the audit and feedback report at the time of the study. LB, VB, and LS were employed by the organization conducting the academic detailing at the time of the study. No other authors have a conflict of interest.
Ethical Approval
Research ethics approval was received by the Women's College Hospital Research Ethics Board (REB #2019-0144-E) and the Ottawa Health Science Network Research Ethics Board at the Ottawa Hospital Research Institute (20180885-01H).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project is funded by the Canadian Institutes of Health Research (CIHR) and Strategy for Patient-Oriented Research (SPOR). CL was funded through a CIHR Health System Impact Fellowship (2019–2021).
Informed Consent
All participants were sent an information letter and informed consent form prior to the interview and were asked to review, sign, and return the form prior to the interview. If written informed consent was not obtained in advance, verbal informed consent was taken before the interview began. Participants were assured that all transcripts would be deidentified and that no identifiable information would be available to their employer. All participants consented for the results to be published.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.