
Abstract
Background
Cancer patients who receive evidence-based tobacco-dependence treatment are more likely to quit and remain abstinent, but tobacco treatment programs (TTPs) are not consistently offered. In 2017, the U.S. National Cancer Institute, through the Cancer Moonshot, funded the Cancer Center Cessation Initiative (C3I). C3I supports 52 cancer centers to implement and expand evidence-based tobacco treatment in routine oncology care. Integration into routine care involves the use of health information technology (IT), including modifying electronic health records and clinical workflows. Here, we examine C3I cancer centers’ IT leadership involvement and experiences in tobacco-dependence treatment implementation.
Method
This qualitative study of C3I-funded cancer centers integrated data from online surveys and in-person, semistructured interviews with IT leaders. We calculated descriptive statistics of survey data and applied content analysis to interview transcripts.
Results
Themes regarding IT personnel included suggestions to involve IT early, communicate regularly, understand the roles and influence of the IT team, and match program design with IT funding and resources. Themes regarding electronic health record (EHR) modifications included beginning modifications early to account for long lead time to make changes, working with IT to identify and adapt existing EHR tools for TTP or designing tools that will support a desired workflow developed with end-users, and working with IT personnel to make sure TTPs comply with system and state policies (e.g., privacy laws).
Conclusions
The experiences of C3I cancer centers regarding the use of health IT to enhance tobacco-dependence treatment program implementation can guide cancer centers and community oncology practices to potentially enhance TTP implementation and patient outcomes.
Plain Language Summary
Almost a quarter of patients first diagnosed with cancer report current cigarette smoking. There are tobacco treatment programs (TTPs) that effectively help patients quit smoking to improve cancer treatment response, survival, and quality-of-life. In 2017, the U.S. National Cancer Institute (NCI) funded the Cancer Center Cessation Initiative (C3I) and supported 52 cancer centers to implement these TTPs. A key component of these programs is the information technology (IT) necessary to refer patients to the program and document their progress. As coordinators of C3I, our team conducted interviews with IT leaders at these cancer centers to learn about the implementation of the programs. IT leaders suggested that IT teams be involved early in the program implementation process and that leaders communicate with the IT team regularly to address necessary changes to referral and documentation systems. IT teams are important to involve early and regularly throughout the TTP implementation process because they have unique knowledge of how funding, policy, and existing technological tools will impact the implementation and success of the program. Our findings emphasize the importance of involving IT teams early in the planning process for such programs. Studies such as this focusing on the experiences and knowledge of specific team members, such as the IT team, enhance tobacco-dependence treatment program implementation and can guide cancer centers and community oncology practices to implement these programs to improve patient outcomes.
Introduction
Almost a quarter of patients first diagnosed with cancer report current cigarette smoking (Talluri et al., 2020). Evidence-based tobacco-dependence treatment is an effective way to improve tobacco abstinence, cancer treatment response, survival, and quality-of-life outcomes (Condoluci et al., 2016; Kassim et al., 2020; Ramaswamy et al., 2016; Warren, 2019). However, cancer centers with tobacco treatment programs (TTPs) do not consistently report these program outcomes (Day et al., 2019). Programs that have reported program outcomes also report implementation challenges and low patient reach (D'Angelo et al., 2019), with about half of the patients with cancer advised to quit (Price et al., 2019; Talluri et al., 2020) and even fewer referred to treatment (Price et al., 2019).
Electronic health record (EHR) system modifications, such as pop-up messages to screen patients for tobacco use, opt-out referral systems (i.e., patients with a documented smoking status are automatically referred to cessation services), and tools to enable the delivery of smoking treatment at the point of care increase patient referral, engagement, and smoking cessation in TTPs (Craig et al., 2022; Flocke et al., 2020; Jose et al., 2020; May et al., 2020; Ramsey et al., 2020). However, the factors impacting the implementation of such modifications are not well understood, especially in oncology settings.
The Cancer Center Cessation Initiative (C3I) was funded in 2017 by the NCI as part of the Cancer MoonshotSM program (Croyle et al., 2019) to integrate and enhance TTPs in routine oncology care. Three successive cohorts totaling 52 NCI-designated cancer centers (cohort 1: 22 centers; cohort 2: 20 centers; cohort 3: 10 centers) were funded to implement this work (Figure 1). The C3I Coordinating Center at the University of Wisconsin Carbone Cancer Center supports the centers by providing technical assistance, data collection to monitor the impact of the initiative, and knowledge integration and dissemination. Previous analyses identified that one year after funding the first cohort of centers, leaders reported challenges related to engaging information technology (IT) leadership and completing EHR modifications for identification and treatment referral of patients who smoke (D'Angelo et al., 2019; Hohl et al., 2022).

Cancer Centers Participating in Cancer Center Cessation Initiative (C3I) as Part of the NCI Cancer MoonshotSM Program
Research is still needed to understand how IT and EHR integration can best support TTP implementation. Both IT engagement and modification of the EHR are critical determinants of program implementation (Rizer et al., 2015; Sligo et al., 2017). Strategies such as reducing referral complexity, creating incentives for oncologists to use the systems, and using existing EHR tools may mitigate challenges associated with IT and EHR integration (LeLaurin et al., 2022; Rojewski et al., 2019). Furthermore, key IT-related goals of the TTP (e.g., deployment of EHR tools to prompt, facilitate, and track tobacco-dependence treatment delivery) depend heavily on IT team engagement in TTP implementation. While previous implementation studies included surveys of health IT personnel (Kooij et al., 2018; Ser et al., 2014), none to our knowledge focused specifically on health IT team leaders’ experiences implementing treatment programs in oncology settings. Identifying the challenges IT teams experienced in supporting TTPs, and the solutions that helped them overcome such challenges, can inform TTP implementation planning in future tobacco treatment initiatives. In this study, we address this gap by examining IT team leaders’ experiences of applying EHR capabilities to support TTP implementation in oncology settings.
Method
Study Design
The goals of this study were to: (a) characterize IT leaders’ experiences implementing and sustaining health IT infrastructure to support the TTP and (b) identify levels of IT engagement and EHR modification for evidence-based TTPs. We conducted a qualitative study using interviews conducted in 2018–2020 and survey data collected for the July–December 2019 reporting period as part of existing C3I evaluation activities. Our analysis included: (a) transcripts from interviews with program IT leaders and (b) survey data collected from 12 NCI-designated cancer centers participating in C3I. Research involving the interview and survey data was deemed exempt by the University of Wisconsin-Madison Institutional Review Board. Interview data were used to address our research questions regarding IT leaders’ experiences and engagement in implementing TTPs, and survey data were then used in the interpretation phase to contextualize levels of IT engagement and EHR modification alongside qualitative interview findings. This work is reported in alignment with the Consolidated Criteria for Reporting Qualitative Research (Tong et al., 2007).
Data Collection
Interview Data
The interviewers (BR and HD), both PhD-level researchers with training in qualitative approaches, conducted semistructured in-person interviews with team members at cohort 1 and 2 centers between September 2018 and March 2020. The 30–60-min interviews included 12 main questions (Supplemental Material 1) with probes to understand the process, barriers, and facilitators of implementing an evidence-based TTP in oncology care. Interview participants were informed of the purpose of the interviews, which were audio-recorded and professionally transcribed. For this analysis, we included transcripts from all interviews with IT leaders representing the 11 (of 22) cohort 1 and 1 (of 20) cohort 2 C3I centers that participated in the qualitative interviews and submitted quantitative report data for the July to December 2019 reporting period. Other cohort 2 visits and interviews were suspended due to COVID-19. Each C3I center director chose who would be interviewed and not all felt their IT teams were sufficiently engaged in program implementation to be included as interview participants. Some interviews included TTP IT leaders (N = 26) and other TTP members (some with more than one role), including clinicians (N = 3), cancer center directors (N = 1), and administrators (N = 2), with a total of 30 respondents representing 12 centers.
Survey Data
Every six months, the C3I Coordinating Center collects data from C3I centers via a web-based Qualtrics survey. Twenty-two items assess cancer center and TTP characteristics, the status of implementation activities, and aggregate data on program reach and effectiveness among patients for the prior 6-month period. The bi-annual report is described in more detail elsewhere (D'Angelo et al., 2019).
Data Analysis
We analyzed interview transcripts with C3I program IT leaders to explore experiences with health system IT infrastructure modifications and implementation within their centers’ TTP workflow, interactions with cancer center leadership and staff involved in EHR modification for the TTP, and experiences with potential application to other oncology settings. Moreover, we sought to identify strategies for successfully integrating health IT to effectively support TTP implementation.
Transcripts of interviews with program IT leaders and other TTP team members (N = 30 respondents) across 12 C3I centers that submitted data reports for the July–December 2019 reporting period were uploaded into NVivo (released in March 2020; QSR International Pty Ltd, 2020). Two coders (JB and CN) performed structural coding of each interview transcript by applying content-based phrases (e.g., facilitator and barrier) to text segments (Saldaña, 2015). Coders were trained by the project scientist (SH) and supervised by the principal investigator (BR), who have experience in qualitative and mixed-method studies. Discrepancies in coding were discussed and resolved during weekly meetings. As part of a conventional content analytic approach (Hsieh & Shannon, 2005), coders further reviewed all quotes associated with the codes and developed themes. The research team agreed upon emergent themes and selected representative quotes for inclusion in the paper.
To identify levels of IT engagement and EHR modification, we analyzed the survey item evaluating nine implementation activities to assess cancer centers’ involvement in IT and implementation of the EHR and workflow with the following response options: not started, in progress, completed, and in maintenance (Table 1). Survey data were analyzed using SAS (Version 9.4; SAS Institute Inc., 2013). Descriptive statistics were calculated for IT levels of engagement for the cancer center TTPs (Figure 2).

Progress of N = 12 Centers on Activities Related to IT Involvement in Implementing the TTP During the July–December 2019 Bi-Annual Survey, N = 11 Received Funding from 2017 to 2019, and N = 1 Received Funding From 2018 to 2020
Response Levels for Implementation Activities Related to EHR Modification in the C3I July–December 2019 Bi-Annual Survey
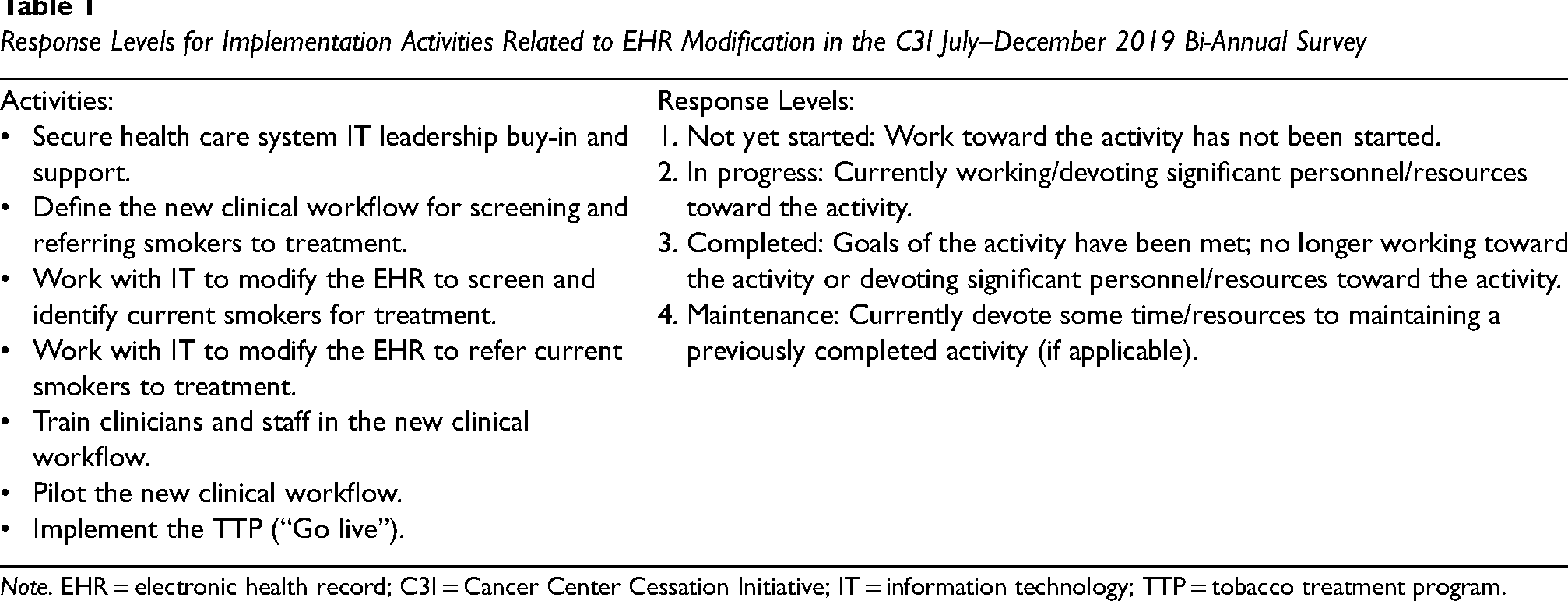
Note. EHR = electronic health record; C3I = Cancer Center Cessation Initiative; IT = information technology; TTP = tobacco treatment program.
Results
We grouped emergent themes into two categories: (a) IT personnel roles and engagement and (b) EHR modification, which was a process involving changes to the existing EHR and the development of new prompts, workflows, and collection of patient information (Table 2).
Emergent Themes on Factors Related to Impacting TTP Implementation From C3I IT Interviews Conducted From September 2018 to March 2020

Note. TTP = tobacco treatment program; C3I = Cancer Center Cessation Initiative; IT = information technology; EHR = electronic health record.
IT Personnel Roles and Engagement
IT leaders described the importance of clarifying specific responsibilities and functions related to TTP implementation early in project planning. For successful implementation of the TTPs, IT leaders expressed a need for IT personnel specifically dedicated to the TTP, early involvement of the IT team, an understanding of the roles and influence of IT among IT personnel and other TTP team members, and consideration of IT funding factors.
IT Personnel Dedicated to the TTP
Most (10 of 12) centers’ IT leaders expressed that IT and analyst support was integral for modifying and maintaining EHR workflows and running bi-annual reports of centers’ TTP outcomes to send to the C3I coordinating center. These reports included aggregate data on patient screening, TTP services offered, engagement in the TTP, and demographics. The purpose of collecting these reports was to track the implementation of the TTPs and to report their benefits. As one IT leader stated: [W]ithout a good analyst, I don’t know how sites can get reporting like they should. (Respondent 1, Center 1) Probably the heaviest maintenance piece for us … was running the reports. And that has more to do with two things. One, [EHR vendor's] data structure is not the easiest to get data out of. And two, we have a centralized data reporting team that is completely overwhelmed, and so we stepped in to provide support for this. (Respondent 7, Center 4)
Early IT Team Involvement
IT leaders expressed a need for early involvement of the IT team in relation to TTP implementation. Two centers reported being in the “in progress” stage for the activity “secure health care system IT leadership buy-in and support” (Figure 2). The remaining 10 centers were in the “completed” or “maintenance” stages. In qualitative interviews, IT leadership at half of the centers (6 of 12) expressed challenges related to involving IT teams too late in the implementation process. These challenges hindered IT leaders’ capability to determine what resources for EHRs were available and to integrate the EHR efficiently and effectively with the TTP. As one IT leader expressed, the initial communications between IT and the TTP team involved a discussion of what EHR resources would be appropriate for the program: The initial planning phase had a couple barriers maybe just because the initial ask was to create an [EHR vendor] registry, and we didn't think that was a good use for a…registry. …there was a little bit of back and forth as to what we could do on the project. (Respondent 18, Center 8) I think one of the challenges was not really understanding from the very beginning exactly what was needed…. I think that's been kind of the root to some of the challenges is getting what they needed on time. (Respondent 17, Center 7)
Involving IT as early as the adoption decision-making or initial implementation planning phases may facilitate implementation, as one IT leader suggested: And I think that's kind of a problem just for the university itself is letting the right people know that they're doing these grants because even the research group[s] [including the IT team] don't always know of all of the things that have been submitted…. (Respondent 16, Center 7)
Beyond early involvement of IT and modification of the EHR, about half (7 of 12) of centers’ IT leadership expressed the importance of consistent communications between IT and other TTP team members throughout the TTP implementation: [C]ommunication is key, obviously, staying in touch with… the rest of the team and making sure that I understand what their request is. So when they say, hey, we want all patients that… have cancer as a history, there's so many different ways that you can interpret that. …And, really, validating it along the way is super important because you can reach different conclusions with data, as we all know, depending on how your process plays out. So it's really vital that we stay on the same page. And communication is key through that. (Respondent 19, Center 9)
Understanding the Roles and Influence of IT
IT leadership also expressed their capabilities and limits of their influence in EHR workflow design and utilization. Many (9 of 12) of the centers’ IT leadership expressed limited power or influence within their roles, such as over whether clinicians utilized the EHRs. One IT leader pointed to a need for TTP leaders and cancer center directors to encourage the utilization of EHR prompts: [Requests for clinicians to utilize the TTP related prompts] should come from the top down, you know, if it's going to be a major change to so many people's lives and all their workflows…. That was by far the most labor intensive as far as meetings and pushback and all that. (Respondent 14, Center 6) I think one of the biggest… things that we're facing right now is just making sure that the clinicians 100% understand the charting and understand what they're selecting and why. …Is it a matter of do we need more end user education, or is it a matter of it's not clear enough, maybe we need to change some of the wording? (Respondent 26, Center 11)
Matching Program Design With IT Funding and Resources
Additionally, how the IT team was funded affected the IT team's ability to prioritize the TTP implementation process and program design. Several (5 of 12) of the centers’ IT leadership explained that their IT team worked on several projects and may not have charged specifically for work related to the TTP or had an IT team that was hired or compensated as part of the project. In centers where IT teams worked on several projects at once, the IT team was often not able to prioritize the TTP or specific research and there subsequently were delays or long lead time before the TTP could “go live,” whereas IT teams hired as part of the grant or were funded with the TTP project were often able to prioritize the work required to implement and maintain the EHR for the TTP. TTP leadership did not always understand that lack of funding specifically for the TTP project would lead to such delays: [I]f we come to the table with funding, it just makes things easier to have those conversations and actually have the [TTP] implemented. … I try to make sure that folks understand, this is just a logistical part of the whole picture… it just makes easier for any organization… to accommodate, to prioritize then…. It will take people's time. It does take effort. (Respondent 4, Center 2)
EHR Modification
IT leaders described modification of the EHR for the TTP as a process that involved changes to the existing EHR and, potentially, the development of new prompts, workflows, and collection of patient information. In the July–December 2019 survey, a couple (2 of 12) of centers reported they were in the “in progress” stage for the activities “work with IT to modify the EHR to screen and identify current smokers for treatment” and “work with IT to modify the EHR to refer current smokers to treatment” (Figure 2). The remaining 10 centers were in the “completed” or “maintenance” stages. Three themes related to EHR modification included: (a) planning for the long lead time required to make EHR changes, (b) leveraging existing EHR tools, and (c) understanding the impact of internal and external policies on what was possible within the EHR.
Long Lead Time to EHR Modification
Planning for the long lead time to modify the EHR for the TTP was emphasized as an important factor in implementing the TTP, with many (9 of 12) centers’ IT leadership commenting on the impact of time required to devote to EHR modification. Whereas early involvement of IT teams was encouraged as a step toward understanding appropriate tools and timelines, beginning modification of the EHR was discussed as an important step that would inevitably take time and troubleshooting before full implementation for the TTP. There was a general understanding among IT leaders that several months would be spent on these steps before the EHR could “go live” and be used by clinicians. One IT leader described this process: Well, I think that's how we spend over the course of working with them… like 2 months maybe, probably about 15, 20 hours total. Some of that time was in explaining things and gathering, reporting requirements, some of that on my own, building out reports. (Respondent 17, Center 7)
Using Existing EHR Tools
Participants shared how their experience with and knowledge of existing EHR tools could facilitate changes to the EHR and workflow for faster implementation of the TTP. Many (9 of 12) of centers’ IT leadership offered suggestions for setting up EHR workflows, which often included adopting or adapting existing tools within EHR systems: [EHR vendor] had the toolkit, and we pretty much, with very little changes, we just followed the toolkit. … [I]t saved a lot of time. … And so the build wasn't that difficult. (Respondent 23, Center 9) [We] created what we refer to as smart data elements. And our smart data elements function similarly to how flow sheets handle data. But the smart data elements can be embedded inside a note…. (Respondent 18, Center 8)
Understanding and Engaging End-Users
Participants often suggested working with end-users of the EHR referral systems used for the TTP workflow to determine what EHR modifications would be needed for the TTP. A common suggestion for implementing EHR modifications was to work backward from the desired TTP workflow: So I think to describe it succinctly, I would say we looked at the requirements and recommendations of the program, worked our way backwards, and then built our own version on top of that. (Respondent 18, Center 8) So we ask questions about how quickly do you need to know that an event occurred, or certain data has been recorded in the system, or certain data is being generated? That allows us to understand how we should be integrating an external system with EMR [Electronic Medical Record], or how we should have notifications come up, or how we should have the research study team manage their study to the degree necessary within the EMR…. (Respondent 4, Center 2)
Furthermore, IT leaders emphasized the importance of surveying end-users, such as clinicians, to pilot and troubleshoot workflows: But with anything in charting, there's that potential that there could be a little bit of confusion. And I think utilizing… some surveys or something with the end users to make sure that if we make changes… that we don't confuse them further. (Respondent 26, Center 11)
Impact of Internal and External Policies
According to IT leadership at half (7 of 12) of the centers, policies at the health system and state levels affected EHR modification. Many of these policies were not under the control of IT leaders or other TTP team members. For example, it was common for centers to have different systems or workflows being used across clinics. One IT leader explained how their team was able to adapt EHR workflows for each clinic: Some of our clinics function differently. So…we do adopt or adapt. So the first option is, we have a great workflow, you just adopt it out of the box how it is. But if your clinic functions a little bit differently, then we'll adapt it. (Respondent 8, Center 5) …it was a much smaller lift to do the initial extract to [vendor] and then have [vendor] be brought back for use. It's a much bigger lift to bring data back. And we had legal involved. We had security involved. We had privacy involved. (Respondent 4, Center 2)
Similarly, one IT leader offered advice that policies involving contracting an EHR system vendor require time, and to expect delays: I think that's one of the lessons learned, I think, for other sites. I guess what you're trying to get at is contracting can take a really long time…. (Respondent 20, Center 9)
According to one IT leader, state laws can restrict personal health information allowed in the EHR, which prohibits the collection of information when it falls under the mental health or addiction realms. These legal issues present issues for the scalability of such programs, according to one IT leader: We’ve got issues where patients want to get more information and can’t because we can’t put that information in the EMR based on… state law. [The] state law is very restrictive on mental health and who has access to mental health information. And that puts a barrier for research in general…. [F]or this particular program, smoking cessation, I don’t think has as many barriers. But if you were looking at scalability and looking at other addiction, the EMR has a lot of challenges with addressing addictions and patient privacy. (Respondent 7, Center 4)
Discussion
In this qualitative study, we analyzed interviews and survey data to (a) characterize IT leaders’ experiences implementing and sustaining health IT infrastructure to support the TTP and (b) identify levels of IT engagement and EHR modification for evidence-based TTPs. Our study is unique in that we interviewed IT leadership on their experience implementing a health program and related EHR modifications, in this case for tobacco-dependence treatment programs, which has not to our knowledge been done before. We discovered strategies for the involvement of the IT team and EHR modification to implement TTPs. These themes are important for leaders of TTPs to consider when planning the involvement of IT personnel and modification of EHR and workflows in their cancer centers. TTP implementation is possible across diverse settings, but it is important to understand the context and involvement that is required to avoid delays. Here, we highlight successful strategies for implementing TTPs for patients of cancer centers.
Involving the IT Team: Involve IT Early and Consider Role and Funding Implications
A key takeaway from our analysis is the suggestion to involve IT early to gather input on what is possible for the TTP's EHR functionality and workflow, and to reduce delays. In our quantitative analyses, most centers had secured buy-in from their IT teams near the time of the qualitative interviews, which took place one to two years after they had received funding for the TTP. However, IT leadership expressed their wishes to have been involved sooner and suggested that some delays and troubleshooting could have been avoided had they been so. Specifically, IT leaders could be involved as early as the grant writing or planning stages of the TTP to share input on what EHR or analysis plans are possible.
Employing dedicated IT analysts who can prioritize the TTP was also emphasized as an important component for EHR modification and producing data reports for research and program evaluation. A lack of dedicated IT leaders who can prioritize and provide guidance on EHR modification has been found to be a key reason for EHR projects stalling or failing (Aldosari, 2017). TTP leaders should know how funding will impact the IT and analyst teams’ time and dedication to the TTP, and subsequently impact time to EHR modification.
Centers with IT and analysts funded for work specifically on the TTP and EHR were better able to prioritize implementation, whereas those who did not have funding or prioritization specifically for the TTP reported delays in addressing EHR modifications. Therefore, when creating expected timelines for TTP implementation, it is important to understand how IT funding and prioritization will impact the time for EHR modification. IT leadership also expressed benefits to consistent communication between IT personnel and the larger TTP team. Consistent feedback to the IT team likely allowed troubleshooting of the EHR and dialogue about how to improve the TTP workflows and data outputs.
Furthermore, IT leaders described their roles in the TTP implementation process, and the limits of their influence in some key domains (e.g., workflow design, TTP program component acceptability, and utilization among clinicians). These themes are consistent with research highlighting the roles that health system leaders and end-users play in addition to IT in EHR modification and utilization (Tutty et al., 2019). In our study, some of the challenges mentioned by IT leaders highlighted the TTP factors they did versus did not have control over. For example, IT personnel were able to address issues related to confusion over EHR prompts by troubleshooting the work flows or wording with clinicians. However, IT leadership expressed a need for leader buy-in and support to encourage clinicians to use the EHR prompts. Therefore, TTP leaders need to know that IT leaders are important team members whose ability to support the utilization of the EHR may be limited.
Modifying the EHR: Begin Modification Early, Consider Existing Tools and End-User Engagement, and Understand Policy Implications
A consistent understanding among IT leaders in our analysis was that the EHR modifications to support the TTP will take several months. Most centers by the time of qualitative interviews had completed modifications of the EHR and workflow for their TTP, and IT leaders were able to share experiences of the process. Beginning modifications to the EHR as soon as possible could lead to faster implementation of the TTP, as the initial workflow will require piloting and troubleshooting. Beginning EHR modification early has also been recommended in previous studies of EHR implementation (Aguirre et al., 2019). By beginning modification of the EHR as early as possible, the overall timeline to implement the TTP may be shortened.
Additionally, there were several suggested strategies for EHR modification from the IT leaders. One suggestion was to use existing toolkits within systems, such as smart data elements and flow sheets. Another suggestion was to work backward from the desired workflow when modifying the EHR. It was suggested to ask end-users questions about the desired workflow, how frequently events occur, what data needs to be recorded in the EHR, and how data would be utilized or exported from the EHR. These findings are consistent with previous research demonstrating the importance of surveying clinician end-users for EHR workflow modification (Khairat et al., 2021; Murphy et al., 2019).
IT leaders were also aware of system-level factors that impacted EHR modification, such as contracts with software companies that could impact what changes to the EHR were possible—factors academic researchers and clinicians may not be aware of. These factors included state-level policies, such as privacy laws, that could impact what information could be entered into the EHR or shared for research purposes. These factors are not surprising given the impact of policy and regulatory impacts on EHR utilization (Tutty et al., 2019) and the inherent privacy concerns of EHRs; however, these issues may change as future technology for EHRs evolves (Evans, 2016). Considering these state and system policies early in EHR modification can reduce surprises and delays.
Limitations
This study addresses an important gap in implementation research by providing health IT leaders’ experiences with modifying and implementing health IT infrastructure to support TTP implementation in oncology settings. However, the experiences represented in this study are from health IT leadership in cancer centers that already had a health IT team engaged in the TTP. The health IT leaders included in this study may have had more involvement and support regarding the modification of health IT for the TTP than IT leadership at centers without such support; however, there were varying levels of engagement and dedicated time from the IT teams for the TTP.
Conclusions
Our findings suggest EHR modification for TTP implementation may be facilitated by involving IT early, communicating with IT regularly, understanding IT personnel roles and influence in the TTP, and matching program design with IT funding and resources. Furthermore, EHR modification may be facilitated by planning for EHR modifications early, adopting or adapting existing tools, engaging end-users for desired workflows, and exploring how policies may impact implementation processes. The experiences of C3I cancer centers regarding the use of health IT to enhance TTP implementation can guide cancer centers and community oncology practices to implement these programs and enhance patient outcomes. By engaging IT personnel as integral team members and utilizing and modifying EHR capabilities efficiently, TTPs can be implemented faster to reach patients within less time for greater cancer survivorship outcomes.
Supplemental Material
sj-docx-1-irp-10.1177_26334895231185374 - Supplemental material for Using information technology to integrate tobacco use treatment in routine oncology care: Lessons learned from the U.S. Cancer Center Cessation Initiative Cancer Centers
Supplemental material, sj-docx-1-irp-10.1177_26334895231185374 for Using information technology to integrate tobacco use treatment in routine oncology care: Lessons learned from the U.S. Cancer Center Cessation Initiative Cancer Centers by Jennifer E. Bird, Claire VT Nguyen, Sarah D. Hohl, Heather D’Angelo, Danielle Pauk, Robert T. Adsit, Michael Fiore, Mara Minion, Danielle McCarthy and Betsy Rolland in Implementation Research and Practice
Supplemental Material
sj-pdf-2-irp-10.1177_26334895231185374 - Supplemental material for Using information technology to integrate tobacco use treatment in routine oncology care: Lessons learned from the U.S. Cancer Center Cessation Initiative Cancer Centers
Supplemental material, sj-pdf-2-irp-10.1177_26334895231185374 for Using information technology to integrate tobacco use treatment in routine oncology care: Lessons learned from the U.S. Cancer Center Cessation Initiative Cancer Centers by Jennifer E. Bird, Claire VT Nguyen, Sarah D. Hohl, Heather D’Angelo, Danielle Pauk, Robert T. Adsit, Michael Fiore, Mara Minion, Danielle McCarthy and Betsy Rolland in Implementation Research and Practice
Footnotes
Acknowledgments
The authors would like to thank IT directors and personnel at the NCI-designated cancer centers who completed C3I reports and provided their time and insight as interview participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the NCI (ICF Contract #17GZSK0031).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.