
Abstract
Background
There is a priority need to make community-based care widely available for people living with schizophrenia (PLwS) in low- and middle-income countries. An innovative approach for increasing access could be to integrate clinical services available in tertiary care hospitals with community-based care through a task-sharing approach. We describe such an integrated intervention that was implemented at Tezpur in northeast India in collaboration with the Lokopriya Gopinath Bordoloi Regional Institute of Mental Health (LGBRIMH).
Method
The objectives of the study were to illustrate the feasibility of integrating and implementing the intervention and to describe its individual, systemic, and public health impacts. Due to the limited resources available, we conducted a pragmatic single-arm longitudinal evaluation of the intervention cohort over 24 months.
Results
Of the 239 PLwS enrolled in the intervention, 198 (83%) were followed up for 24 months, with nearly three-quarters reporting a >70% reduction in disabilities, most notably between 6 and 18 months. There was a marked reduction in unmet needs across multiple domains, and at 24 months, 62% of the cohort was engaged in individual jobs or other market-linked livelihood opportunities. There was greater uptake and retention with outpatient contacts at the LGBRIMH, and PLwS experienced a marked (82%) reduction in inpatient admissions rates, as compared to before enrolment. Over a period of 24 months, primary caregivers reported that their families experienced significantly fewer social difficulties such as unemployment, interpersonal conflicts, and social isolation. The intervention had a significant public health impact, with an estimated 51.8% effective treatment coverage rate for the integrated intervention.
Conclusion
Our findings provide preliminary evidence of the feasibility of implementing the integrated intervention and its effectiveness. We believe that there is merit in further in-depth refinement and exploration of this implementation-related research and cost analysis while replicating the intervention in other tertiary care institutions.
Plain Language Summary
In low- and middle-income countries such as India, integrating clinical services available at tertiary mental health hospitals with community-based care through a task-sharing approach is an innovative way to make community-based care widely available for people living with schizophrenia (PLwS). The purpose of our study was to investigate the feasibility of implementing such an intervention in a community in Tezpur, northeastern India, in collaboration with a Lokopriya Gopinath Bordoloi Regional Institute of Mental Health (LGBRIMH), and to describe the individual, systemic, and public health effects of the intervention. Our findings suggest that integrating the intervention is feasible, has significant impacts on individuals and public health, and is an effective way to expand access to community-based care for PLwS through partnerships with existing tertiary care institutions.
Introduction
The continued lack of access to community-based and recovery-oriented care for people living with schizophrenia (PLwS) is a public health, social, economic, and human rights concern, especially in low- and middle-income countries (LMICs). Hence, one key objective of the WHO Mental Health Action Plan 2013–30 is to increase the service coverage for severe mental disorders globally by 50% by providing “comprehensive, integrated, and responsive mental health and social care services in community-based settings” (World Health Organization 2021a). Despite this and previous calls to action (Eaton et al., 2011; Lancet Global Mental Health Group, 2007), the expansion of community-based care in LMICs such as India has been sporadic (World Health Organization, 2021c), with continuing large treatment gaps (National Institute of Mental Health Neuro Sciences Bengaluru, 2016), resulting in an increasing burden of disability attributable to schizophrenia (Vos et al., 2020). In the absence of accessible care options, PLwS living in many LMICs continue to experience significantly high mortality (Liu et al., 2017), a range of psychosocial disabilities (Charlson et al., 2015; Sagar et al., 2020), and adverse social consequences such as widespread stigma and discrimination (Koschorke et al., 2014), poverty, and social exclusion (Lund et al., 2011). Thus, making effective community-based care more widely available in LMICs is a public health, developmental, and social justice priority (World Health Organization, 2021b).
Since the launch of the National Mental Health Program in India, there has been increased availability of community-based services for PLwS in the public health system through the District Mental Health Program (Gupta & Sagar, 2018). The District Mental Health Program provides treatments (mostly pharmacological) through district hospitals, outreach clinics in primary care facilities, and departments of psychiatry in teaching hospitals (Gupta & Sagar, 2018). While access to care has become easier, the relative lack of efforts to address demand-side barriers to treatment seeking like the stigma associated with seeking help, treatment cost, and a lack of interventions to promote PLwS social inclusion has continued to make treatment uptake and retention rather limited, as the recent treatment gap and burden of disability figures indicate (National Institute of Mental Health Neuro Sciences Bengaluru, 2016).
In the global mental health discourse around community-based mental health services in LMICs, the role of tertiary care mental hospitals in contributing to expanding access has been largely ignored. In India, mental hospitals will continue to be an important component of the public mental health system, receiving the largest share of budgetary support and the largest pool of specialist human resources (National Human Rights Commission, 2016). Some of these institutions provide community services through periodic outreach clinics in surrounding locations, indicating their readiness for incorporating community-based services. Tertiary care mental health hospitals could significantly expand treatment coverage and are likely to improve patient outcomes by implementing an integrated (between hospital and community) collaborative and recovery-oriented intervention for PLwS in their contiguous communities (Chatterjee, 2017). However, to the best of our knowledge, there is no such integrated care pathway approach in operation in India, which, in the context of low resources, represents a missed opportunity. In this context, we describe the development and impact of a collaborative integrated intervention that was conducted as a component of the “Integrated care for the needs of vulnerable people with severe mental disorders (INCENSE)” project in India (Murthy et al., 2017). The two main aims of this exploratory study were to:
Describe the processes and feasibility of integrating and implementing the intervention. Describe the individual, family, systemic, and public health impacts of the integrated. intervention
Method
The Innovation
The community-based rehabilitation (CBR) intervention has been demonstrated to be feasible and effective in multiple community settings, but not in an integrated manner with tertiary care hospitals (Chatterjee et al., 2003, 2009, 2014). The main implementation question addressed in this study was whether tertiary care institutions in India could be successfully engaged in increasing the availability of catchment area-based, recovery-oriented community services for PLwS. This is not the norm for such institutions, which usually provide a range of facility-based services with limited links to the community. The service innovation involved a method of shifting from an individual, facility-based service approach to a population-based one through an integrated care pathway straddling the hospital and the community that would comprehensively cater to the medical, psychosocial, and recovery-oriented needs of PLwS in a defined catchment area (Figure 1). This would involve the integration of the available clinical services in the hospital with a recovery-oriented, community-based intervention that would be available to all PLwS in the defined catchment area. The CBR intervention for PLwS was determined to be an appropriate fit for the community component of the integrated care pathway for three reasons: first, it was developed and tested in diverse community settings in India, including through a randomized controlled trial ((RCT); (Chatterjee et al., 2014) second, it addresses the key recovery domains of social and economic inclusion; and finally, it is feasible to implement through task sharing with lay health workers, peers, and caregivers from the local community.

Changes in the Care-Seeking Pattern
Settings
The integrated intervention was implemented in collaboration with the Lokopriya Gopinath Bordoloi Regional Institute of Mental Health (LGBRIMH), located in the urban conglomerate of Tezpur, situated in the Sonitpur district of the northeast Indian state of Assam. Established in 1873, the LGBRIMH is one of India's oldest mental hospitals, which transformed into a National “Center of Excellence.” The institute currently has 350 beds, providing mostly acute care and well-established postgraduate teaching courses across a range of disciplines. It is the only such tertiary mental health care institution in the whole of northeast India and provides a range of multidisciplinary clinical services to people in the region. Prior to the INCENSE program, the institute would conduct monthly outreach clinical services and medication in one subdistrict hospital in the Sonitpur district, with no community-based services available for PLwS in Tezpur town and the surrounding areas. Since there was no existing capacity available within LGBRIMH for implementing the CBR intervention, the hospital decided to collaborate with an external resource organization with the relevant expertise. As a result, the integrated intervention was developed and implemented through a collaborative partnership between LGBRIMH and two nongovernmental organizations with the necessary institutional and financial resources to implement the CBR intervention.
Intervention Development Process
The integrated intervention was developed in a collaborative manner, involving a series of consultations with key stakeholders. The process involved the INCENSE team, the senior staff of LGBRIMH, PLwS and their family members, and other influential people in the community such as local government officials, municipal councilors, and village council members. Key steps included institutional integration with LGBRIMH, engagement and discussion with PLwS and caregivers on their perspectives, and community participation and networks through a multisectoral platform. Through these processes, a consensus was reached to implement the program for PLwS across all 19 municipal wards of Tezpur and five surrounding rural “gram panchayats” (village councils), with a total population of 144,000 persons, as per the 2011 census (Chandramauli, 2011). The intervention followed a three-phased, phased implementation process to ensure successful integration. The first phase, which lasted 16 months, was primarily concerned with planning and integrating the innovation within LGBRIMH, determining the needs of patients and caregivers, and forming partnerships with organizations to address social determinants of recovery. The intervention was put into practice across LGBRIMH and the nearby community during the second phase, which lasted for 6 months. The third stage, which lasted for 18 months, concentrated on maintaining and normalizing the intervention, incorporating it into routine care, providing repeated training and feedback, and expanding previous partnerships with local and regional organizations to address the social determinants of recovery, such as real-life employment. See Supplemental Appendix A for a detailed description of the intervention's development and phased implementation.
Intervention Description and Delivery
Individual Level
The collaborative community-based care intervention (Chatterjee et al., 2014) was delivered by trained and supervised lay recovery support workers (RSWs) residing in the catchment area. RSWs were recruited by placing advertisements in the local newspaper, with specific selection criteria including being from the same geographic location, being proficient in the local language, and having a minimum of 12 years of education. Following a rigorous selection process, eight RSWs successfully completed the two-month training program based on the Care of People with Schizophrenia in India (COPSI) manual (Chatterjee et al., 2014), developed in India for working with people with schizophrenia and their families. These RSWs were continuously supervised and supported to ensure that patients and their families received effective and appropriate care.
The first step in individual-level intervention involved an assessment and diagnostic review of participants by psychiatrists at LGBRIMH and the initiation of psychotropic medications (typically risperidone or olanzapine), followed by a referral to the community team, which was also located in the outpatient (OP) clinics. For PLwS who were already in contact with the hospital, psychiatrists continued treatments and referred them to the community team for psychosocial interventions. This included collaboratively developing an individual care plan based on a structured needs assessment, improving illness management skills, encouraging medication adherence and regular medical reviews, improving personal care, taking care of physical health, encouraging social interactions, and planning to engage in paid work.
PLwS were encouraged to participate in group-based skill development activities in two drop-by centers or through home-based support for transitioning to individual local jobs and other income-generating livelihood opportunities. These included enhancing agricultural income through higher-value spices and organic farming practices, tailoring, handloom weaving, fish farming, and the sale of regional bamboo-based handicrafts. To further encourage their financial inclusion, PLwS received support in obtaining the necessary documents to operate bank accounts, accessing small business loans, and opening post-office linked savings accounts.
Family Level
In recognition of their critical role, all primary caregivers and significant others were closely involved in the intervention process. RSWs provided emotional support to family members as well as discussed illness management skills (including adherence management), attention to physical health, and managing difficult symptoms during their home-based sessions. Primary caregivers and other key family members were encouraged to actively participate in efforts to improve personal care, activities of daily living, social interactions and functioning at home, and transition to employment for their family member living with schizophrenia. RSWs also recorded social difficulties faced by families, for example, unemployment, substance abuse, legal difficulties, and social isolation, and attempted to address these through linkages with local government and social agencies. Family members were also provided with basic financial skills to manage household incomes as well as introduced to various low-risk financial instruments and accessible small business loans.
Peer, Caregiver, and Community Engagement
Community engagement was a core component of the integrated intervention to address demand-side barriers such as limited awareness about schizophrenia in the community, widespread stigma, discrimination, and social isolation. There were two main methods employed for the community engagement component: existing social agencies and direct interface with the community. In the initial phase, the INCENSE intervention was introduced across the catchment area through town hall meetings in each of the municipal wards and villages. This was followed by sustained interactions with local government officials, nongovernmental agencies, community groups such as women's and youth clubs, young people in schools and Tezpur University, and other influential community members. Active efforts were also made to engage with small businesses and local industry bodies to identify employment options, work with local financial institutions such as banks and post offices to promote financial inclusion and provide free legal aid services in the district. One example of systemic discrimination was the initial refusal of the banks to open accounts for the PLwS citing their lack of capacity to do so. This was resolved after it was brought to their attention that the Reserve Bank of India (which governs banking procedures in India) has guidelines that stipulate that anyone with psychosis is deemed to have the capacity to open and operate bank accounts unless proven otherwise.
As part of the engagement process, RSWs conducted small group meetings on an ongoing basis in their local communities to provide information about mental health, mental health conditions such as psychosis, the availability and benefits of treatments, common myths around schizophrenia, and the crucial need for community support for their recovery. The INCENSE and LGBRIMH teams organized a series of public meetings and interactions to promote awareness and stress that recovery is possible with treatments and social support. Over time, peers and caregivers became increasingly involved in conducting community engagement activities, and their personal testimonies had a powerful impact on improving community attitudes toward PLwS. As an unanticipated outcome of these efforts, by the second year, around 60 caregivers, young people, and other interested community members had registered as volunteers, undergone training, and supported PLwS in their neighborhood by befriending them and encouraging them to seek appropriate services at LGBRIMH, continue their treatments, and find employment.
Quality Assurance
To ensure the quality and safety of the CBR intervention, a well-defined supervision structure was implemented. RSWs were supervised by program coordinators on key tasks. In the early stages, intervention coordinators accompanied RSWs on house visits to ensure that RSWs met competence standards in their tasks. In addition, weekly team meetings were held to discuss challenging scenarios and continue skill enhancement.
Monitoring and Evaluation
The main objectives of the evaluation were to examine the feasibility of implementing the innovation and to describe the individual, family, and public health impacts of the intervention.
Design
For measuring individual and family outcomes, given the available resources, a pragmatic single-arm longitudinal evaluation of the intervention cohort was conducted over 24 months.
Enrollment of the Cohort
The intervention cohort was enrolled in two phases: between February and July 2013 (followed up until June 2015) and then from May to September 2015 (followed up until August 2017), covering a combined population of approximately 144,000 persons.
Evaluation Framework
The feasibility of implementing the intervention was assessed post hoc in a pragmatic manner across several key and measurable domains using a set of process indicators and individual outcome measures. The evaluation was based on the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework (Glasgow et al., 1999). The domains of the innovation, the indicators and measures, and the data collection procedures are summarized below and described in detail in Supplemental Appendix B.
Measures and Outcome
The RE-AIM framework was evaluated through a set of process indicators or output measures collected over the duration of the intervention, while the effectiveness domain included individual and family level outcome measures.
Process Indicators
The flow of participants in the intervention was monitored by collating the numbers enrolled, the numbers receiving the intervention, dropouts, planned discharges, and deaths due to any cause collected every month.
To document the treatment status, RSWs recorded whether PLwS in their caseloads had been regular, irregular, or nonadherent with medicines at the time of enrolment and then after 6, 12, 18, and 24 months.
To compare inpatient service utilization patterns of PLwS before and during the program, all inpatient admissions data for the two years prior to the intervention was recorded at the time of enrolment. During the intervention, RSWs recorded all subsequent episodes of admissions for individual PLwS.
For measuring the fidelity of the community-based intervention, the COPSI RCT session-by-session manual (Chatterjee et al., 2014) that specifies the key tasks to be conducted by RSWs was used as the benchmark, and a set of process indicators around contacts with PLwS and caregivers and sentinel events in the care pathway were recorded from the individual case records and collated monthly.
To ensure that the CBR intervention delivered was of adequate quality, a well-defined supervision structure was put in place. The RSWs were supervised by the senior program coordinators for key tasks such as obtaining informed consent, contacting families, carrying out home visits, completing individual case records, and collecting and entering data. In the early stages of the intervention, intervention coordinators would accompany RSWs on their house visits and observe the sessions to ensure that RSWs met competence standards in delivering them as per plans. In addition, weekly team meetings were held to discuss cases, identify problems, and clarify them through group discussion and continued knowledge and skill development. The information related to the number and type of supervision was recorded and compiled every month.
For evaluating the individual and family impact of the intervention, well-validated outcome measures were used and are briefly described below.
Indian Disability Evaluation and Assessment Scales
Disability was measured using the Indian Disability Evaluation and Assessment Scale (IDEAS; The Rehabilitation Committee of the Indian Psychiatric Society, 2002). The IDEAS assesses disability across four domains: self-care, interpersonal activities, communication and understanding, and work. Each domain is scored between 0 and 4, (no disability to profound disability), and adding the domain scores generates a total disability score between 0 and 16. The IDEAS has satisfactory content validity, criterion validity, and internal consistency, and is widely used in disability certification and research studies in India.
Adapted Camberwell Assessment of Needs Scale
RSWs conducted the needs assessment through discussions with PLwS and their primary caregivers by using the Camberwell Assessment of Needs Short Appraisal Schedule (Phelan et al., 1995), which had been adapted for Indian settings in a previous RCT (Chatterjee et al., 2014). The instrument assesses met, partially met, or unmet needs across 10 domains: managing symptoms, emotional well-being, social needs, role functioning, social relationships, leisure activities, self-care, physical health, stigma and discrimination, and spiritual needs.
Social Difficulties Checklist
To document the social difficulties faced by families, the Social Difficulties Checklist from an earlier RCT was used (Chatterjee et al., 2011). This measures 10 commonly reported social difficulties that were rated as present or absent by the primary caregiver, such as unemployment in family members other than the PLwS, interpersonal conflicts, substance abuse, and social isolation.
Data Management
The data was collected by a team of 12 RSWs who met with PLwS and their family members at their homes or, if preferred by the PLwS and family, at a different location. While care was taken to ensure privacy during these visits, this was sometimes a challenge, particularly when the entire family was residing in one room. All data were collected using paper and pencil and entered into a database by a dedicated data entry person. Entries were validated by the onsite program coordinator, and after final quality checks by the data manager, the final values were entered in the master data file. The data was stored as password-protected files on secure computers and anonymized backup versions were maintained on a separate device.
Ethical Issues
The foundational premise of the INCENSE program was the importance of participation and empowerment for people with severe mental disorders; hence, all individual data collection was done in a manner consistent with good clinical practice guidelines. Written informed consent from both PLwS and their caregivers was a precondition for enrollment in the program, using a structured consent procedure that has previously been used for PLwS in India (Chatterjee et al., 2015). The independent Technical and Ethics Advisory Committee was constituted to independently oversee key ethical aspects, including confidentiality, data preservation, and anonymity procedures. Since this was primarily an intervention program and not a research study, as per the existing frameworks in India at the time of the study, there was no requirement for additional ethical clearances.
Data Analysis
First, we describe the sociodemographic characteristics of PLwS who were enrolled in the program. Next, we report the baseline IDEAS scores and clinical factors, including duration of illness, pattern of treatment, and hospital admissions in the two years prior to enrollment. We also report the proportions and types of unmet needs in the cohort as well as the types and frequency of social difficulties experienced by their families at baseline. Then, we examine changes in the total IDEAS score for PLwS from baseline (enrollment) to 12 and 24 months. We categorized participants into three groups based on the change in their IDEAS score as (i) limited improvement (<40% change), (ii) moderate improvement (40%−70% change), and (iii) substantial improvement (>70% change) at 24 months. We also examined baseline factors associated with the change in IDEAS score using the nonparametric Kruskal–Wallis H test and performed a post hoc Dunn test to identify significant differences in pair-wise comparisons. Finally, we describe changes in unmet needs, social difficulties experienced by the participant's family, and employment outcomes at 12 and 24 months. We used the McNemar test to identify significant differences in unmet needs and social difficulties between the baseline and the end of the follow-up. All analyses were conducted using Stata version 16.1.
Results
Reach or Treatment Coverage Estimations
The National Mental Health Survey of India 2015–2016 reported the adult (18 and older) prevalence of schizophrenia in India as 0.4% (Gururaj et al., 2016). Based on this figure, after excluding about 45% of the total population who were below the age of 18, we estimated that there would be approximately 316 adult PLwS residing in the catchment area (population of 144,000). A total of 239 PLwS (75.6%) were enrolled in the program; of these, more than two-thirds, or 164 out of 239 (68.6%), were on regular treatments and reported a 40% or more reduction in their disability scores over 24 months. Using these as indicators of effective treatment, we estimated that the effective treatment coverage rate was 51.8% (164 out of 316).
Effectiveness Evaluation
The PLwS in the cohort had a total of 27 episodes of inpatient admissions during the 24-month intervention period. Compared with the admissions rate prior to enrollment (0.62 per participant per 24 months), admissions per participant during the 24-month intervention period (0.11) showed an 82% reduction.
Patient Characteristics and Baseline Measures
A total of 239 PLwS were enrolled in the intervention, of whom 198 (83%) were followed up for 24 months (Figure 2). Among the rest of the PLwS, 27 dropped out, 11 recovered sufficiently to warrant planned discharge before 24 months (and continue with OP care at LGBRIMH), and three died due to age-related physical health complications. The majority of PLwS who dropped out did so within the first six months after recruitment and were likely to be older than 50 (31% >50 years vs. 14% ≤50 years, p = .057) and with a shorter duration of illness (median duration: 5 years vs. 8 years, p = .002).

Enrollment and Follow-up of the Cohort
Nearly one-third of the participants (n = 76; 32%) were young adults, and more men (59%) enrolled in the program. Close to half of the cohort were single (49%; n = 118) and parents were most frequently the primary caregivers (40%). About 45% (n = 107) of participants had completed high school education or more, although, at enrollment, 155 or 65% of participants were not engaged in any meaningful work; 24 women living with schizophrenia were engaged in managing household activities, and 50 (21%) were either self-employed or working full- or part-time in mostly unskilled jobs. A large proportion (39%) of families reported serious financial distress, living below the designated poverty line in terms of household income (Table 1).
Sociodemographic Profile of the Cohort at Enrollment

The median duration of illness for the cohort was five years (range: 2–33 years), and 14% (n = 34) of participants had never received psychiatric treatment. In the 12 months prior to enrollment, the majority (n = 140; 59%) of participants were on sporadic treatments (less than six contacts at LGBRIMH), with less than one-third (27%) following up regularly (six or more contacts; Table 2). The proportions of PLwS reporting moderate or severe disability across the four domains of the IDEAS were: self-care (38%), interpersonal activities (49%), communication and understanding (49%), and work (56%). About 9% of participants reported moderate or more severe disability across all four domains. Nearly one-third of PLwS reported having at least one hospital admission in the previous two years, and the mean number of admissions per participant in the 24 months prior to enrollment was 0.62 (per 24 months).
Clinical and Disability Profile of the Cohort at Enrollment

Note. IQR = interquartile range; SE = standard error; IDEAS = Indian Disability Evaluation and Assessment Scale.
Table 3 shows the profile of unmet needs at the time of enrollment. More than 50% of the participants reported having multiple unmet needs. The most frequently reported unmet needs were managing symptoms and negative emotions, a lack of meaningful activities and friends, perceived discrimination from others, low self-esteem and feelings of shame, accessing disability benefits, an inability to manage money or use public transport, and excessive tobacco use. Table 4 shows the common social difficulties experienced by families at enrollment: unemployment (n = 103; 43%), serious interpersonal disputes (n = 56; 23.4%), substance abuse (n = 48; 20.1%), and social isolation (n = 50; 20.9%).
Unmet Needs Reported Based on Adapted Camberwell Assessment of Needs Scale

*Statistically significant (p < .05) change in the percentage of participants reporting unmet needs between baseline and 24 months.
Social Difficulties Reported by Families at Baseline, 12 Months, and 24 Months

*Statistically significant (p < .05) change in the percentage of families reporting social difficulties between baseline and 24 months.
Changes Over 24 Months
There was a consistent reduction in reported unmet needs at 24 months, except for access to disability benefits, which increased from 59.8% to 69.7%. PLwS reported marked changes in the management of symptoms and emotions, physical health concerns, having meaningful activities, functioning in the home and family roles, having friends, engaging in instrumental activities such as travel and money management, fear of disclosure, perceived discrimination, and self-esteem. At 24 months, significantly fewer families reported difficulties such as domestic violence, substance abuse, interpersonal conflicts, and social isolation. However, there was no significant change in the percentage of families facing social difficulties related to legal disputes, illness or disability in the family, and parenting issues.
Figure 3 summarizes the trajectory of the total and domain-specific IDEAS scores of the cohort over 24 months, showing that the largest reduction in disability scores occurred between 6 and 18 months of the program. Out of the 197 participants who completed outcome evaluations at 24 months, nearly three-quarters (74%, n = 146) experienced a >70% reduction from their baseline IDEAS total scores. As shown in Table 5, women, who were married (Dunn test; p = .009) and had their spouse as their primary caregiver (Dunn test; p = .037) were likely to report more than 70% improvement in their IDEAS scores at 24 months. In contrast, men, those who reported being single, and those who had two or more hospitalizations in the past two years were significantly more likely to have experienced <40% improvement in their disability scores in the same period.

Total and Domain-Specific Indian Disability Evaluation and Assessment Scale (IDEAS) Score* at Baseline, 6, 12, 18, and 24 Months
Change in IDEAS Score From Baseline to 24 Months
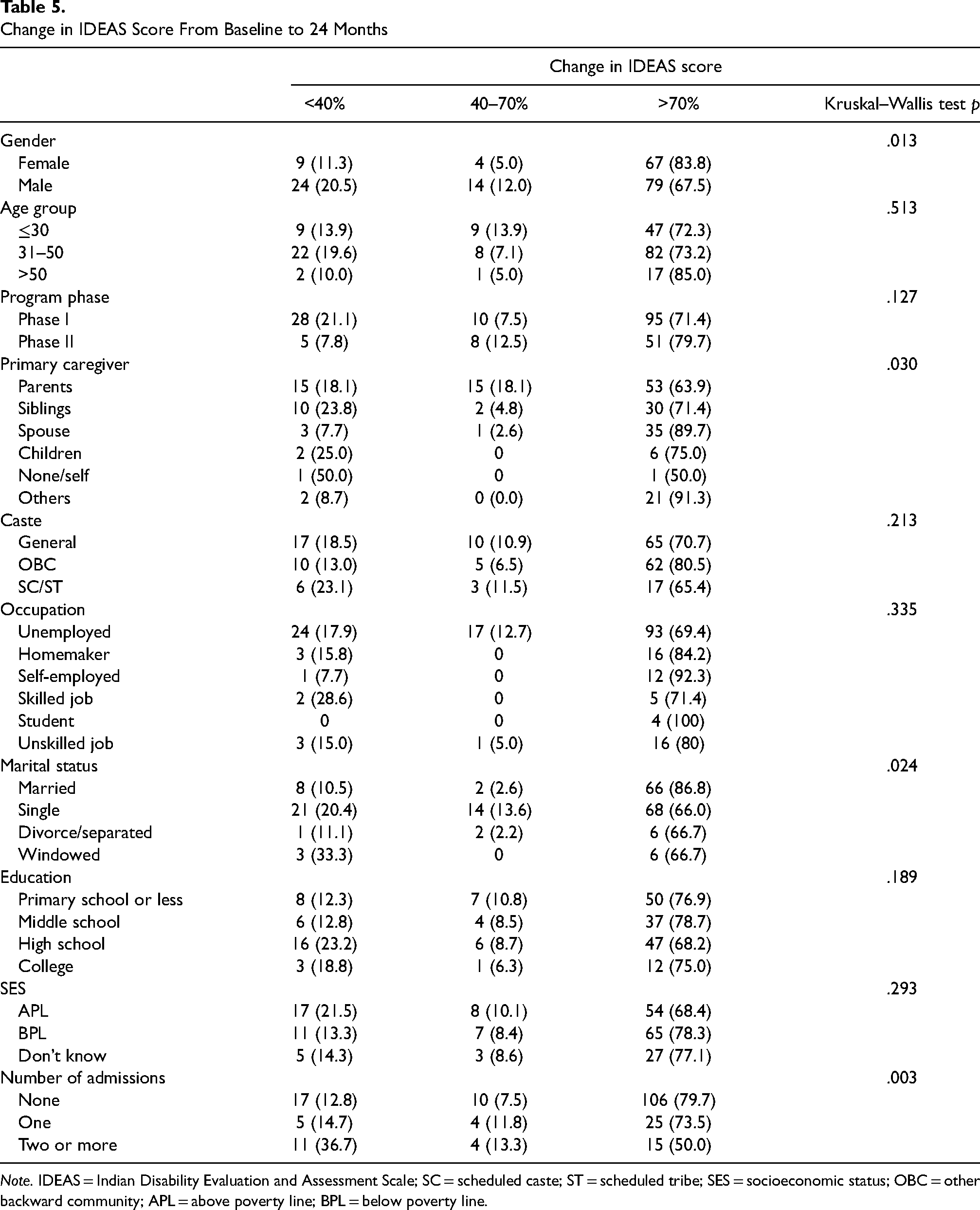
Note. IDEAS = Indian Disability Evaluation and Assessment Scale; SC = scheduled caste; ST = scheduled tribe; SES = socioeconomic status; OBC = other backward community; APL = above poverty line; BPL = below poverty line.
About one-third of the participants (n = 80) joined the livelihood skills development support component of the intervention. Men were slightly more likely to join (38% vs 27%; p = .07), as were those from households below the poverty line (43% vs. 27%; p = .017). While there was no difference in baseline disability scores between those who received skill development support and those who did not, there were significantly fewer hospitalizations in the former group. Among the 80 PLwS who received livelihood support and skills training, 72 found employment, and at 24 months, about 62% (n = 101) of the cohort were engaged in regular income-generating work.
Figure 4 shows the changes in treatment status of the cohort over the course of the program. Within 6 months, the majority of PLwS were on regular treatment, and overall, this trend continued over the 24 months of the intervention. The maintenance of the integrated intervention was indirectly estimated from the four-calendar-year period (phases 1 and 2 combined) of implementation and the 83% retention rates of PLwS and their caregivers over a substantial period of 24 months (Figure 2).

Change in Treatment Uptake Status of the Cohort Over 24 Months
Discussion
Given the gap between the need for and availability of community-based care for PLwS within the public mental health system in India, the INCENSE-integrated intervention was implemented and evaluated to explore whether tertiary care institutions in India can implement population-based and recovery-oriented services for PLwS in their immediate catchment areas through an integrated care pathway. While developing community-based services has been identified as a key component of the institutional reform process in India (National Human Rights Commission, 2016), there is an evidence gap about the feasibility and impact of such interventions in real-life settings.
We describe the phased process of implementing the innovation, providing details on the intervention's context, key individuals involved, and an evaluation of feasibility based on the RE-AIM framework's criteria. The results on domains of coverage (reach), systemic, individual, and family level effectiveness, high fidelity of implementation, improved treatment adherence, and the maintenance of results over a period of two years are promising and indicate that the integrated innovation was feasible to implement. For most of the cohort, especially women and those who remained married, there were substantial reductions in disability and unmet needs, improved rates of treatment uptake and retention, and significantly fewer admissions. These benefits were evenly distributed across various socioeconomic groups. However, due to the small sample size for gender-segregated analysis of outcome categories, which is one of our study's limitations, a more detailed examination of gender differences in these findings was not possible. Additionally, the absence of a control group and the possibility of measurement bias require cautious interpretation of individual outcome results.
The trajectory of changes in disability scores for the cohort suggests that it takes about six months before observing significant reductions in psychosocial disabilities, which continue to decrease until about 18 months before stabilizing. This finding indicates that a 24-month follow-up period is necessary to consolidate the clinical and social recovery gains of community-based interventions for PLwS. With the introduction of the CBR component of the integrated intervention, there was an early and sustained change in the way PLwS utilized the clinical services available at the LGBRIMH. From a pattern of intermittent uptake of OP services, limited adherence to such services, and multiple episodes of admission for acute care, PLwS shifted to regular OP follow-up accompanied by a steep reduction in episodes of inpatient care. Reduced inpatient admissions not only cause less disruption for PLwS and their families but may also help to ease the burden of care in inpatient settings. Improved uptake and adherence to treatments were found to be associated with reduced psychosocial disability and clinical improvements, resulting in greater social participation and successful transitions to employment. Another strength of the integrated intervention was the increased accessibility of acute inpatient care, which was required by some PLwS in the cohort. However, the study is limited by the lack of qualitative data examining the factors that influenced this significant behavioral change in PLwS and their caregivers, which may be a key mechanism of interest.
As highlighted during the consultations with PLwS and caregivers during the intervention development process, the lack of opportunities for meaningful, income-generating work is a significant barrier to their recovery and social inclusion in India and other LMICs (Balaji et al., 2012). Hence, dedicated efforts were made to support PLwS in making the transition to real-life work options in an informal economy context. Consistent with previous reports of the work status of community-living PLwS reported from other rural settings in India (Suresh et al., 2012), at the time of enrollment, about a third of the cohort was either working at home or as daily wage unskilled workers, and much less often, in formal jobs. The employment support component enabled an additional third of the cohort to make a successful transition to individual jobs and other market-linked livelihood options. In addition, as caregiving requirements reduced substantially, several family members were able to find employment, leading to increased family incomes.
Previous community-based programs and implementation studies have demonstrated improved contact coverage rates for PLwS, especially in settings with little or no preexisting community services (Hanlon et al., 2020; Jordans et al., 2017). However, there is little data on effective treatment coverage rates for community-based interventions for PLwS, the gold standard metric for evaluating the public health benefits of interventions (Tanahashi, 1978). Since the INCENSE intervention was implemented within a defined catchment area, it was possible to estimate the effective treatment coverage rate at more than 50% over 24 months. To the best of our understanding, this is the first demonstration of effective treatment coverage rates for a community-based program for PLwS in an LMIC setting.
Conclusion
In the field of global mental health, the discourse on tertiary care mental hospitals and community-based care has followed divergent and at times conflicting pathways. The INCENSE-integrated intervention suggests that this need not be the case. As the findings demonstrate, building on the available specialist care in these facilities with an evidence-based community intervention is feasible to implement in a catchment area-based method with substantial individual and public health impacts. Overall, the findings consistently indicate that this innovation is feasible for further expansion. In the future, the implementation process will need to be evaluated in a more explicit, theory-based, and structured manner, as well as address additional dimensions such as costs, sustainable financing mechanisms, research to track changes in stigma, and community knowledge and attitudes toward PLwS. Given these promising preliminary findings, the integrated care pathway approach should be replicated and refined for widespread adoption in India and other LMICs.
Supplemental Material
sj-docx-1-irp-10.1177_26334895231175528 - Supplemental material for Exploring the feasibility and public health impact of integrating a community-based recovery-oriented intervention for people living with schizophrenia in partnership with a tertiary care mental hospital in India
Supplemental material, sj-docx-1-irp-10.1177_26334895231175528 for Exploring the feasibility and public health impact of integrating a community-based recovery-oriented intervention for people living with schizophrenia in partnership with a tertiary care mental hospital in India by Hamid Dabholkar, Aravind Pillai, Dilip Gaonkar, Sonia Pereira Deuri, Smita Naik and Sudipto Chatterjee in Implementation Research and Practice
Supplemental Material
sj-docx-2-irp-10.1177_26334895231175528 - Supplemental material for Exploring the feasibility and public health impact of integrating a community-based recovery-oriented intervention for people living with schizophrenia in partnership with a tertiary care mental hospital in India
Supplemental material, sj-docx-2-irp-10.1177_26334895231175528 for Exploring the feasibility and public health impact of integrating a community-based recovery-oriented intervention for people living with schizophrenia in partnership with a tertiary care mental hospital in India by Hamid Dabholkar, Aravind Pillai, Dilip Gaonkar, Sonia Pereira Deuri, Smita Naik and Sudipto Chatterjee in Implementation Research and Practice
Footnotes
Acknowledgements
We wish to acknowledge the important contributions made by Mr. Pratheesh Kumar, Mr. Shahid Eqbal, and all other members of the INCENSE team in the implementation of the intervention. We are grateful for the support from the director and the care provided by clinicians and other departmental staff at LGBRMIH. We also gratefully acknowledge the role of the Technical and Ethics Advisory Committee members in providing their independent and valuable oversight. The INCENSE program was supported by Tata Trusts, Mumbai, India. The funding agency had no role in the collection, analysis, and reporting of the data, nor in the drafting of this paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Tata Trusts, Mumbai, India.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.