
Abstract
Background
Evidence-based intervention (EBI) effectiveness is hindered by low rates of caregiver home practice, or caregiver rehearsal of intervention skills at home. Although home practice is essential to intervention success, we know little about what makes home practice difficult to complete. We sought to identify the challenges caregivers face when attempting home practice assignments within the context of community implementation of a family-based preventative EBI. We also aimed to identify barriers, perceived need, and implementation-related factors that may contribute to frequency of home practice challenges.
Methods
The family-based preventative intervention Bridges was delivered to caregivers and adolescents in three public middle schools in North America within a randomized efficacy-effectiveness hybrid trial. Caregivers (N = 233) completed worksheets in which they reported challenges to home practice of intervention skills. Caregiver-endorsed challenges were coded for emergent themes and categorized into higher-order home practice challenge domains. Additional data was gathered through multiple methods. In addition to descriptive analyses, multilevel linear regressions were conducted to identify factors associated with frequency of home practice challenge domains.
Results
Over 85% of caregivers reported one or more home practice challenges. Challenges fell into six domains: daily stresses, cognitions/beliefs about the intervention/practice, caregiver wellness/regulation, adolescent responsiveness, relevance/acceptability of intervention or assignment, and external barriers to practice. Adolescent externalizing symptoms, academic performance, and caregiver participation in the English-language intervention group (compared to Spanish-language delivery) were associated with greater frequency of reported challenges.
Conclusions
Among caregivers already attending intervention sessions, specific support to overcome challenges in daily stresses and beliefs about the intervention/practice can support greater home practice compliance, which in turn may impact overall intervention effectiveness. Findings suggest that providing services in caregivers’ preferred language may avert potential challenges. Further research into home practice challenges is necessary to identify appropriate home practice implementation supports.
Plain Language Summary
Low rates and poor quality of caregiver home practice of intervention skills hampers intervention effectiveness, but no prior studies have identified the difficulties caregivers face when attempting home practice of intervention skills and their rates of occurrence. Within a community implementation of a family-based preventative intervention, we found that difficulties were common and largely fell in the domains theorized to impact engagement, such as daily stresses and beliefs about the intervention/practice. Findings also suggest that providing services and materials in caregivers’ preferred language may avert potential home practice challenges. By identifying common home practice challenges and correlates of different challenges, our findings point to a need to develop appropriate and effective home practice implementation support.
Background
Prevention scientists have identified numerous evidenced-based interventions (EBIs) that prevent adolescent mental and behavioral health problems (Caldwell et al., 2019; Skeen et al., 2019). In particular, family-based and caregiver-mediated EBIs are cost-effective, efficacious, and can have lasting preventative effects on adolescent mental illness, substance use, and risk behaviors (Foster et al., 2006; Furlong et al., 2012; Ladis et al., 2019; Van Ryzin et al., 2016). However, low engagement and participation in intervention activities hinders EBI effectiveness and durability. Of these, home practice, or caregiver rehearsal of EBI skills at home, is crucial to the translation of intervention effectiveness into the real-world (Garland et al., 2008; Kazantzis et al., 2010). Caregiver home practice impacts EBI outcomes over and above attendance and mediates program effects on parenting skills, parent-child relationships, and child internalizing and externalizing symptoms (Berkel, Mauricio, et al., 2018; Berkel, Sandler, et al., 2018; Clarke et al., 2015). Increasing caregiver home practice increases program effects (Jones et al., 2014), especially among ethnic minority families (Berkel, Sandler, et al., 2018). Yet, documented caregiver home practice rates are low, ranging from 35–65% non-compliance (Chacko et al., 2008, 2016; Danko et al., 2016; Pinna et al., 2017). Low home practice rates limit the uptake of effective parenting skills (e.g., positive reinforcement, consistent discipline) that are proven mediators of youth outcomes (Gonzales et al., 2018; Stadnick et al., 2015).
Although home practice is an essential ingredient in numerous EBIs, there is little insight into why caregivers struggle in completing home practice. Prior research has almost exclusively focused on strategies to increase EBI attendance and in-session participation (Fawley-King et al., 2013; Haine-Schlagel & Walsh, 2015; Nock & Ferriter, 2005). For example, technology-enhanced behavioral parenting programs are often built to increase opportunities for feedback and support to caregivers that subsequently increase caregiver engagement in home practice activities (Jones et al., 2013, 2014). Although these programs targeting caregiver home practice and skill generalization show boosts in program effects, they do not reveal the difficulties that preclude home practice firstly. The real-world challenges that make home practice difficult are largely unknown. To our knowledge, no studies have examined caregiver-endorsed challenges that occur during home practice. We know of only two studies that documented reasons for home practice non-compliance. In one, caregivers most commonly reported they did not complete home practice because they forgot, had insufficient time/availability, and had difficulties with implementing the home practice (Chacko et al., 2013). Caregivers also frequently reported attitudinal barriers such as low acceptability, fit, and confidence in the home practice assignment's utility (Chacko et al., 2013). In another, researchers reminded and encouraged parents to complete assigned home practice activities via text messages and included role-plays to problem-solve barriers to home practice within its curriculum, which resulted in high compliance rates (Lachman et al., 2018). Within this high-support context, caregivers reported missing a previous intervention session, parent/child illness, and perceived low self-efficacy in assigned skills as reasons for non-compliance. However, these are barriers noted only among parents who did not complete or attempt home practice assignments. We have yet to identify the broader challenges that preclude home practice as well as the challenges that occur during home practice attempts. Though EBI providers often speculate on the challenges of home practice, caregivers’ own perceptions of these challenges are needed to identify specific and efficacious implementation supports.
We sought to identify the challenges caregivers face when attempting home practice assignments within the context of a family-based preventative EBI. We expected caregiver-endorsed challenges to fall within Staudt's framework of engagement contributors (Staudt, 2007). We also aimed to identify potential contributors to increased challenges with home practice and to specific types of home practice challenges. Considering home practice and home practice challenges as one facet of intervention engagement, correlates of other types of engagement (e.g., attendance, participatory behaviors) may also contribute to understanding caregivers’ home practice challenges (Martinez & Haine-Schlagel, 2018). Within engagement research, three major categories of challenges are potential barriers, perceived need, and implementation factors.
Potential barriers include parent psychopathology and stress, poverty, and systemic barriers, which are associated with lower caregiver intervention participation, including home practice completion rates (Haine-Schlagel & Walsh, 2015; Nock & Ferriter, 2005; Patterson & Chamberlain, 1994). Caregiver depression is consistently associated with both poorer EBI engagement and parenting skills (which are frequently the target of caregiver-mediated EBIs). Caregivers and families with substantial social disadvantages such as negative life events (e.g., job loss, housing instability, loss of family member), poverty, and psychopathology face greater barriers in accessing and utilizing services (Bornheimer et al., 2018; Hodgkinson et al., 2017). These same barriers likely preclude caregivers’ ability to engage in home practice and other intervention activities.
Perceived need, or relevance of the intervention and activities to participants, is also central to EBI engagement (Nock & Ferriter, 2005; Staudt, 2007). Perceived need is linked to higher levels of caregiver participation, greater responsivity to recruitment efforts, and attendance (Gorman-Smith et al., 2002; Perrino et al., 2001; Winslow et al., 2009). Perceived need may have similar effects on caregiver home practice. Caregivers with higher baseline need may be more motivated and therefore more likely to complete home practice and experience fewer difficulties during home practice. However, some studies found no link between perceived need and behavioral participation (Coatsworth et al., 2018; Dumas et al., 2007) or found that it was associated with lower participation and attendance (Fisher et al., 2018; Perrino et al., 2018). These inconsistent findings suggest that a more nuanced examination of the link between need and engagement is warranted. As perceived need may vary across the many intervention elements in a program, examining associations between the perceived need for specific intervention elements and engagement in program content relating to specific elements may be important. Within the context of a family-based preventative EBI targeting positive parenting, family relationships, adolescent academic engagement, and adolescent mental health, it is plausible that perceived need and thus home practice engagement and challenges will vary across these elements. Caregivers with high perceived need for positive parenting and academic support skills and less experience using these skills may be more likely to engage in home practice related to these skills but may also experience more challenges during home practice. For example, adolescent disruptive behaviors make it simultaneously more necessary and important to complete home practice. Similarly, caregiver depression may deter caregiver home practice, but depressed caregivers may also find program activities the most relevant and needed. Conceptualized either as a perceived need or barrier, it is important to examine caregiver and family characteristics’ impact on the potential difficulties that caregivers face during home practice implementation.
Finally, we examined implementation factors that may pose challenges to caregiver home practice such as program language, program fidelity, and number of caregivers participating in the EBI (Haine-Schlagel & Walsh, 2015). Program fidelity, number of participating caregivers, provider background, and program length are often linked to attendance, which in turn is associated with intervention participation (Dumas et al., 2007; Dumas & Albin, 1986; Jensen & Grimes, 2010; Schoenfelder et al., 2013). However, no prior studies have examined the impact of implementation factors on home practice challenges. Community providers frequently cite that EBIs and their assigned activities need to be tailored for minority and immigrant-background families (Chavira et al., 2017; Valentine et al., 2017), which may be reflected in caregivers in non-English intervention programs reporting greater challenges with home practice. It is also plausible that interventions delivered with low fidelity may translate to difficulties when caregivers practice skills at home. Additionally, having two caregivers participate in the program would likely facilitate greater understanding and a shared commitment to home practice assignments thus resulting in fewer challenges (Crane, 1995; Dumas & Albin, 1986; Jensen & Grimes, 2010).
The current study sought to: 1) identify common challenges to intervention home practice assignments and the frequency of their occurrence among caregivers who submitted home practice worksheets, 2) identify factors associated with caregivers’ home practice challenge frequency, and 3) identify factors associated with the most common types of challenges to home practice. Data used in this study was gathered through multiple methods observational coding, caregiver-report, school archival data, program data). Though causation was not formally tested, perceived barriers, need, and implementation factors are conceptualized as contributors of home practice challenges. Additionally, different factors could be implicated for different challenges caregivers face (e.g., time constraints vs. low acceptability of the intervention activity). Nonetheless, identifying which of the above factors is associated with increased report of home practice challenges will help identify areas to increase support to caregivers and families.
Methods
Participants
Study data were drawn from a randomized efficacy-effectiveness hybrid trial of the universal family-based preventative intervention Bridges (trial post-randomization N = 663). Of the 414 families randomized to participate in Bridges, this study utilized a subsample of primary caregivers who submitted at least one assigned home practice worksheets (n = 233; 61.4% Hispanic, 6.0% mixed Hispanic, 16.3% non-Hispanic White, 6.9% non-Hispanic Black, 5.1% non-Hispanic Native American, 4.3% non-Hispanic ‘Other’ race/ethnicity). All caregivers had a child participate in the companion adolescent groups (45.9% female adolescents). Most caregivers in our sample were from two-caregiver households (n = 154, 66.4%). Among the 233 caregivers, 147 caregivers (63.1%) were the sole caregiver participating in the intervention and 86 (36.9%) had a partner also participate. Caregiver participants were predominantly female (94.9%). Caregivers attended intervention groups delivered in either English or Spanish (49.8% Spanish) based on their preference. Annual household income ranged from less than $5,000 to over $100,000 (Median = $30,001-$35,000).
In our sample of 233 caregivers, there were more Spanish-language participants compared to the 181 caregivers who also participated in the intervention but did not submit any home practice worksheets (49.8% vs. 33.7%; χ2(1) = 10.77, p < .01). The ethnoracial makeup of our sample also differed from the 181 caregivers not included (49.2% Hispanic, 8.3% mixed Hispanic, 15.5% non-Hispanic White, 12.7% non-Hispanic Black, 10.5% non-Hispanic Native American, 3.9% non-Hispanic ‘Other’; χ2(5) = 11.13, p < .05). The study sample attended more sessions (M = 3.52) than those not included (M = 0.73; F(1) = 1183.86, p < .001). The two samples did not vary regarding proportions of caregiver sex (χ2(1) = 0.01, p > .05), adolescent sex (χ2(1) = 3.54, p > .05), numbers of caregivers in the household (χ2(1) = 0.21, p > .05), number of caregivers participating in program (χ2(1) = 0.59, p > .05), and household income (χ2(20) = 19.64, p > .05).
Procedures
Data were collected across three cohorts (2016–2018). Adolescents and caregivers were recruited via school events, phone, and mail from three Title I middle schools with high Hispanic student enrollment. Eligibility criteria were: 1) adolescent enrollment in the 7th grade and no plan to change schools; 2) adolescent enrollment in general education classes; 3) at least one caregiver participating who could speak English or Spanish; 4) participating caregiver had sole or shared custody, lived with the adolescent 15 + /month; and 5) family agreed to be randomized to participate in either Bridges or a control workshop condition. Families were not blinded to study condition. In the 7th grade Fall semester, caregivers and adolescents gave written informed study consent or assent, respectively, prior to completing pretest interviews in their homes in their preferred language (English or Spanish). Participants received $50 for the interview.
The four-session Bridges intervention targets youth and family competencies shown to promote youth school engagement and prevent risk for mental health and substance use problems across adolescence and into early adulthood (Gonzales et al., 2012). Volunteer schoolteachers and staff delivered Bridges over seven weeks during the spring semester of seventh grade. Separate caregiver and adolescent groups were conducted simultaneously each week, with combined caregiver-adolescent family groups held at the end of the first and final sessions. Caregivers learned skills for positive parenting and to strengthen family relationships, adolescent behavior management and monitoring, and caregiver mindfulness and emotion regulation to reduce negative parenting and family conflict.
Participants received a program guidebook that included home practice worksheets. Worksheets delineated skills taught within the intervention and asked caregivers about their home practice experience. Worksheets included open-ended questions asking caregivers what made it difficult to use each of the assigned skills. During sessions, intervention facilitators prompted participants to complete and submit the home practice worksheets, including worksheets from previous sessions. Research staff attempted to collect worksheets from all participants. Additional worksheets and pens were available to caregivers who forgot materials. Group leaders prompting completion and collected worksheets in the middle of the session to avoid missing worksheets from tardy participants. Over 90% of caregivers received text reminders to complete home practice and to attend upcoming sessions. All study procedures were approved by the university's Institutional Review Board.
Measures
Potential barriers
Perceived need
Implementation factors
Outcome
Home practice challenges codes and higher order domains.

Note. Home practice challenge domains are italicized with individual codes listed below. n = number of challenges reported by primary caregivers in each respective challenge code among the 642 write-in responses with enough information to code. Some responses reported more than one challenge, resulting in a total of 729 challenges reported by primary caregivers. Proportions (%) calculated out of total number of challenges reported (N = 729).
Analytic plan
All analyses were conducted in Stata 16.1 (StataCorp, 2021). In Aim 1, we sought to identify common home practice challenges and the frequency of their occurrence across all caregivers in the intervention who completed the home practice worksheets. We tabulated the total number of challenges reported among responses, the total number of challenges reported in each domain, and their proportions out of the total number of challenges reported across domains. We then ran descriptives on caregivers’ home practice challenge frequency scores.
In Aim 2, we aimed to identify factors associated with home practice challenge frequency among caregivers who submitted a home practice worksheet. Given the two-level structure of the data (i.e., caregivers nested within intervention groups), we conducted a multilevel linear regression with maximum likelihood estimation to account for five cases with incomplete data. A null model was conducted to assess the variance attributed to between-group variance. Then, home practice challenge frequency was regressed on all hypothesized predictors simultaneously. Caregiver-level variables were potential barriers (i.e., household income, negative life events, depressive symptoms), perceived need (i.e., adolescent GPA, parent-reported positive parenting, negative parenting, family cohesion, and adolescent internalizing and externalizing symptoms), number of caregivers from the same family enrolled in Bridges, and caregiver sex. Group-level variables were group intervention language and program fidelity. Adolescent sex (0 = Female, 1 = Male) and caregiver program attendance (M = 3.52, SD = .74) were included as covariates.
For Aim 3, we repeated the multilevel analyses. Outcomes were the frequency of the challenge domains reported by at least 25% of caregivers who submitted a home practice worksheet. We did not examine predictors of other domains due to their low base rate.
Results
Aim 1. Caregiver-reported challenges to home practice of intervention skills
Of the 233 caregivers in the sample, 199 (85.4%) reported one or more home practice challenges. A summary of the total number of caregiver-reported home practice challenges and their respective higher order domains is presented in Table 1. The most reported domain was daily stressors (39.9% of reported challenges) followed by cognitions/beliefs about the intervention/practice (20.3% of reported challenges). Challenges that fell within the domains of adolescent responsiveness and caregiver wellness/regulation represented approximately 14% of reported challenges each. Relevance/acceptability of intervention or assignment and external barriers to practice each represented less than 5% of reported challenges. Forty (5.5%) write-in responses described a challenge but did not fall into one of the above domains or codes. Figure 1 presents the number of responses in each challenge domain and their proportion among reported challenges.
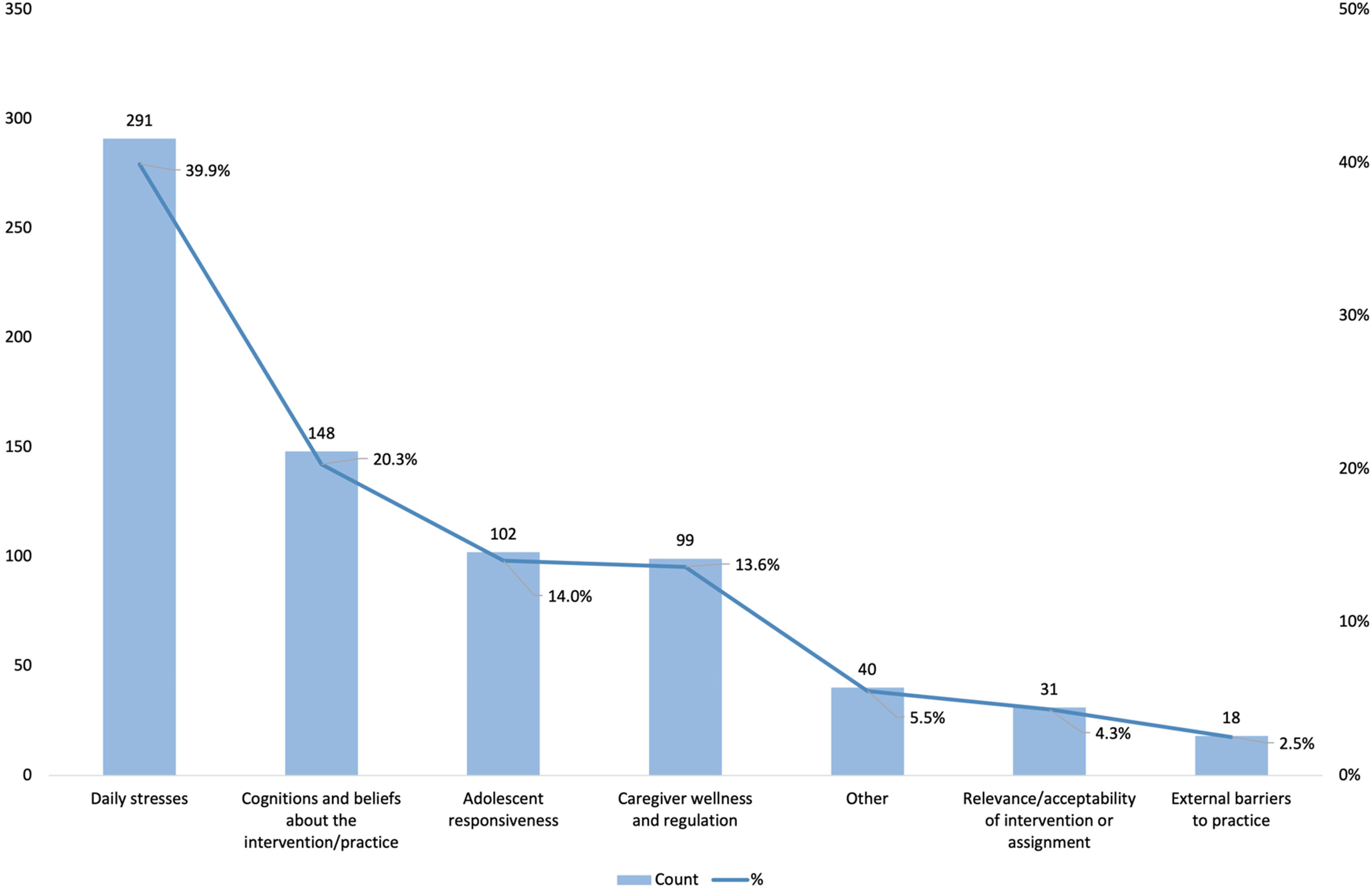
Count of caregiver-reported challenges and proportion relative to total number of challenges reported
Of the 233 caregivers who submitted a home practice worksheet, 134 caregivers (57.5%) reported one or more daily stresses challenges, 84 (36.1%) reported cognitions/beliefs challenges, 70 (30.0%) reported caregiver wellness/regulation challenges, and 65 (27.9%) reported adolescent responsiveness challenges. Relevance/acceptability challenges and external barriers challenges were reported by 11.2% and 7.3% of caregivers, respectively. The proportions of caregivers reporting challenges in each home practice domain are presented in Figure 2 with the average frequency for each domain. Caregivers reported an average of 1.33 challenges per worksheet (SE = .06, Range = 0–4), 0.49 daily stresses challenges per worksheet (SE = .04, Range = 0–2), 0.24 cognitions/beliefs challenges per worksheet (SE = .03, Range = 0–2), 0.19 caregiver wellness/regulation challenges per worksheet (SE = .02, Range = 0–2), 0.19 adolescent responsiveness challenges per worksheet (SE = .02, Range = 0–2), 0.05 relevance/acceptability challenges per worksheet (SE = .01, Range = 0–1), 0.02 external barriers challenges per worksheet (SE = .02, Range = 0–1), and 0.09 other challenges per worksheet (SE = .02, Range = 0–2).
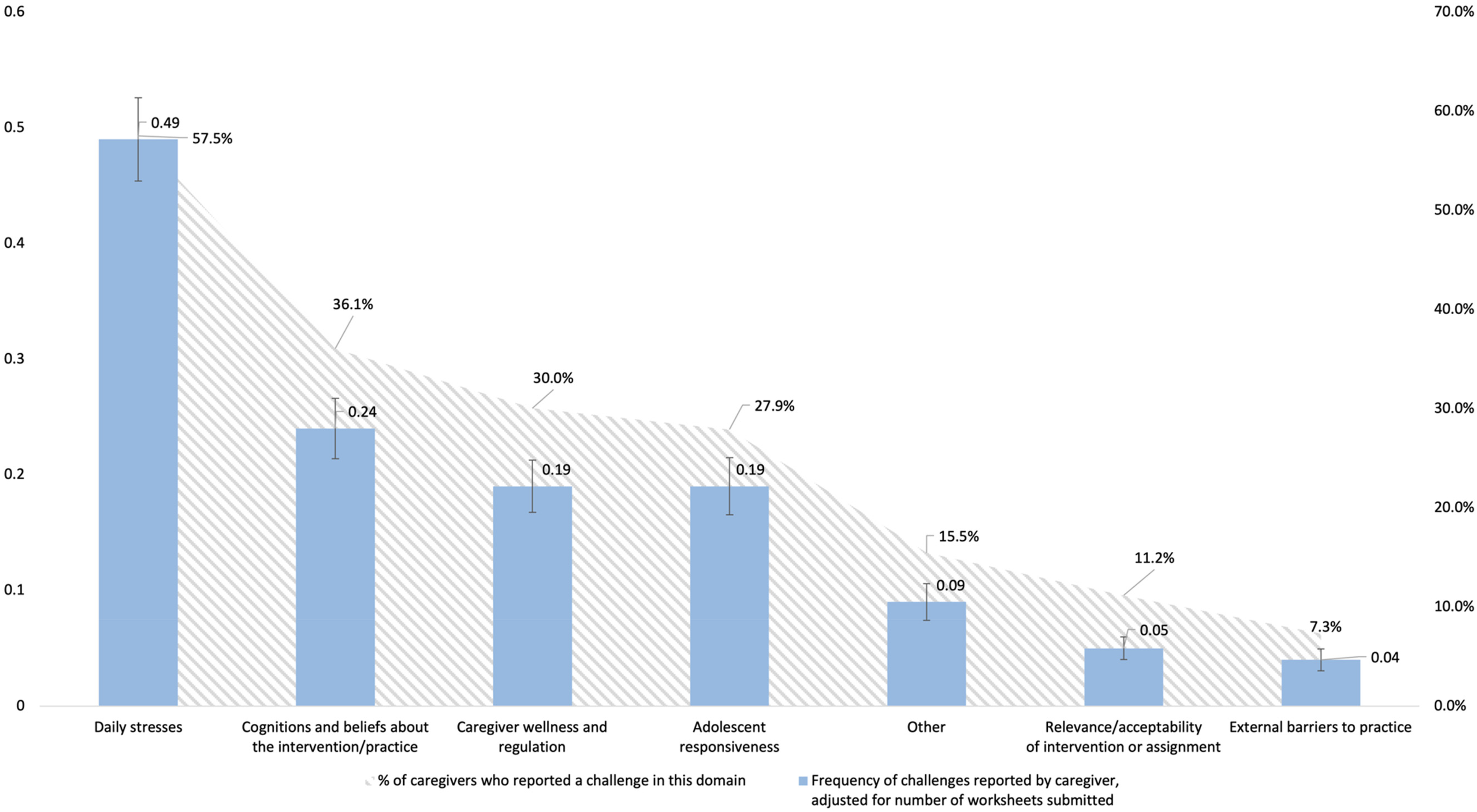
Frequency of challenge domains and proportion of caregivers reporting each challenge domain
Aim 2. Predictors of frequency of home practice challenges
Table 3 presents the results for Aims 2 and 3. The null model revealed that 12.8% of the variance in frequency of reported home practice challenges was attributable to intervention group differences (ICC = .128, SE = .06). In the multivariate model, caregiver-reported adolescent externalizing symptoms (b = 0.03, 95% CI [0.01, 0.04], p < .001) and adolescent GPA (b = 0.28, 95% CI [0.09, 0.47], p < .01) were associated with more frequent report of home practice challenges. Caregivers who participated in the Spanish-language Bridges groups reported fewer challenges than their counterparts in the English groups (b = -0.38, 95% CI [-0.67, −0.08], p < .05). No other variables were significant predictors of frequency of home practice challenges.
Multilevel linear regressions predicting frequency of challenges (N = 228).
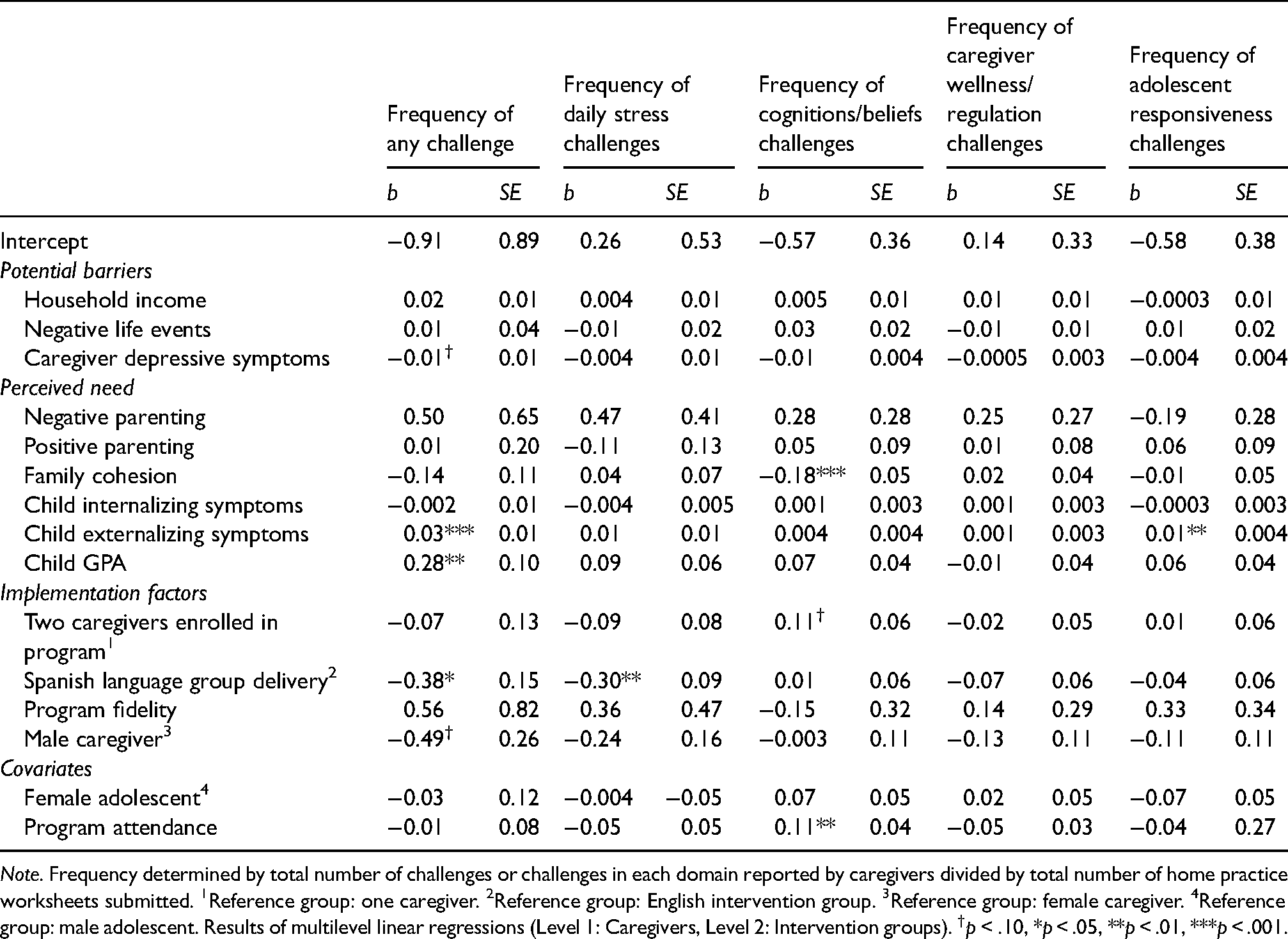
Note. Frequency determined by total number of challenges or challenges in each domain reported by caregivers divided by total number of home practice worksheets submitted. 1Reference group: one caregiver. 2Reference group: English intervention group. 3Reference group: female caregiver. 4Reference group: male adolescent. Results of multilevel linear regressions (Level 1: Caregivers, Level 2: Intervention groups). †p < .10, *p < .05, **p < .01, ***p < .001.
Aim 3. Predictors of frequency of specific home practice challenge domains
Intraclass correlations based on null models are presented in Table 2. Differences among intervention groups accounted for up to 8.5% of the variance in frequency home practice challenge domains.
Intraclass correlations (ICC) of intervention group level (N = 233).

Discussion
Building an evidence-base of caregivers’ challenges in the face of home practice assignments will allow future studies to identify specific and efficacious strategies to support caregiver follow-through of home practice with high accuracy and fidelity to the assignment. We identified common challenges that caregivers experience when attempting to complete home practice intervention assignments, documented the frequency of challenges, and identified factors associated with home practice challenges. All analyses were restricted to caregivers who submitted a home practice worksheet. Over 85% of caregivers reported one or more home practice challenges. In order of frequency, challenges fell into six domains: daily stresses, cognitions/beliefs about the intervention/practice, caregiver wellness/regulation, adolescent responsiveness, relevance/acceptability of intervention or assignment, and external barriers to practice.
Consistent with Chacko et al. (2013) examination of homework barriers, the most endorsed difficulties fell in the domain of daily stresses (reported by 57.5% of caregivers). In order of prevalence, almost 40% of difficulties in this domain were related to not having enough time, distractions in the environment, lack of practice opportunities (e.g., limited face-to-face time with child), and forgetting to do the assignment. Though rates of forgetting to do the assignment were reported less frequently than by Chacko and colleagues, our participants received text message reminders to complete home practice. In the current study, caregivers reported more difficulties finding the time or opportunity to follow through (vs. remembering to do the home practice), suggesting caregivers could benefit from in-session time to schedule times for home practice completion and to set behavioral intentions. Worth noting, the reported difficulties related to time were solely based on caregivers’ own perceptions of the difficulties they faced. The current study did not have access to participants’ schedules or data from other informants about time constraints. Reports of time constraints could also reflect caregivers’ prioritizing other activities over home practice or difficulties with task switching. Objective measures of time constraints and multi-informant data may clarify this finding and provide greater insight into the implementation supports caregivers need.
Cognitions/beliefs challenges represented 20.3% of all reported challenges and were reported by 36.1% of caregivers. Here, caregivers most often reported unfamiliarity with the parenting skill assigned for home practice, followed by listing the skill itself as a difficulty, suggesting that caregivers may require more scaffolding or role-plays with facilitator feedback within EBI sessions prior to home practice. Caregiver report of these challenges may signal need for repeated practice until the new skills become more familiar. Of note, low understanding of the assignment was rarely reported in our sample. The present sample of caregivers who attended sessions and completed part of the home practice worksheets do not appear to struggle with understanding the assignment.
Interestingly, challenges associated with relevance and acceptability of the intervention or assignment were only reported by 11% of caregivers. Among our sample of caregivers who attended EBI sessions and submitted home practice worksheets, concerns about relevance and acceptability were not frequent concerns. However, 43.7% of caregivers who enrolled in the intervention did not submit any home practice worksheets. It is plausible that challenges in this domain would be amplified if we surveyed these participants who did not submit home practice worksheets and/or prematurely dropped out of the program. Nonetheless, findings suggest that commonly touted engagement strategies such as psychoeducation and motivational exercises may be too broad and less relevant to caregivers already bought into EBI activities and submitting home practice worksheets (Becker et al., 2015; Lindsey et al., 2014). Assessment of specific challenges followed by supportive problem solving or rehearsal of challenges are likely more effective for such caregivers.
Regarding factors associated with home practice challenge frequency, none of the potential barriers included in our models were significant predictors of home practice challenges in the final predictor models. Despite evidence that caregiver depressive symptoms may interfere with intervention attendance and participation (Mendez, 2010; Nix et al., 2009), depressive symptoms were marginally associated with frequency of overall reported challenges. Poverty, negative life events, and caregiver depression are often implicated as barriers to attendance (Kazdin et al., 1997), but findings suggest that these factors do not operate as challenges to home practices for caregivers who successfully initiate and attend intervention sessions. Notably, of the 13 predictor variables and 2 covariates included in each of the five regression analyses, only four predictor variables and 1 covariate were significantly associated with overall or domains of home practice challenge frequency. Despite being commonly linked to numerous measures of intervention engagement in the literature (e.g., in-session participation, attendance), few of the theorized predictors were significantly associated with home practice challenge overall or specific domains in our study.
Instead, caregiver-reported adolescent externalizing symptoms, school-reported adolescent GPA, and English intervention group enrollment were associated with greater frequency of challenges. The positive association between adolescent externalizing symptoms and frequency of overall home practice challenges (and frequency of adolescent responsiveness challenges) is logical (Mauricio et al., 2018). Adolescents’ disruptive behaviors beget disruption in the home, making it difficult to follow through on EBI-assigned skills that often center around increased parent-child communication and parental monitoring of child activities. Additionally, caregivers may perceive themselves less effective during home practice activities in the face of disruptive adolescent behaviors. Although we expected caregivers whose adolescents had higher GPAs (i.e., lower perceived need) to report fewer challenges, we found the opposite association. Instead, caregivers with higher achieving students may have had more difficulties with the home practice assignments given that much of the program activities target increasing students’ school engagement by way of caregiver monitoring and scaffolding. Though not reflected in our relevance/acceptability challenge domain, it is possible that the mismatch between program aims and families’ needs resulted in more frequent challenges.
Finally, caregivers in our Spanish intervention groups reported overall challenges and daily stresses less frequently than those in English groups. Qualitative accounts often suggest that EBIs are less acceptable and feasible with non-English delivery and that non-English-speaking participants are less engaged (Barrera et al., 2017; Youn et al., 2019). This was not the case for Bridges, which was initially developed for Mexican-heritage families (Gonzales et al., 2012), suggesting EBIs specifically designed for cultural groups are engaging for the target families. Caregivers in our Spanish language groups were also significantly more likely to submit home practice worksheets, demonstrating that when an appropriate language option is available, Spanish-speaking caregivers participate in EBI activities at higher rates than non-Spanish-preferred caregivers.
Importantly home practice challenges are not necessarily a metric of “barriers” to home practice. Indeed, increasing research on in-session participation and engagement suggests that what we once traditionally considered “barriers” or difficulties with home practice may be a normative part of the learning process, potentially indicating greater engagement in the intervention (Bamberger et al., 2014). Caregivers’ home practice intentions and home practice attempts may be precisely what gives rise to greater difficulties as caregivers strive to master and implement new behaviors. Further, these home practice difficulties may present opportunities for problem solving and adapting home practice skills for specific families (Guan et al., 2017, 2019). The very rationale for home practice is that intervention skills are not always easily implemented, necessitating repeated practice during program sessions and at home.
Alongside in-session support, mobile health applications offer viable implementation support strategies when caregivers face home practice challenges (Jones et al., 2013, 2014; Lindhiem & Harris, 2018). With technology use increasing exponentially, digital interventions and adjuncts demonstrate efficacious, scalable, and sustainable solutions (Lindhiem et al., 2015; Morrison, 2015; Yardley et al., 2015). In-app reminders and planning features can tackle daily stresses. Cognitions/beliefs, adolescent responsiveness, and relevance/acceptability challenges could be addressed by digital content libraries for skill review, modules scaffolding tailoring of intervention elements to the user, and increased program skill exposure at home. These implementation support solutions are ubiquitous among mobile health platforms and already being used to bolster parenting interventions (Lindhiem & Harris, 2018; Morrison et al., 2012). For instance, Jones et al. (2014) added technological adjuncts to a behavioral parenting training intervention and found that digital support strategies such as daily smartphone-delivered surveys, mid-week video-calls to problem-solve obstacles, caregiver video-recording of their own home practice, and home practice reminders resulted in increased home practice compliance, skill generalization, and attendance compared to caregivers who did not receive the technology enhanced program. Additionally, caregivers reported the added benefit of being able to easily share and review intervention skills with their partners not participating in the program sessions.
Certainly, study findings are limited by the context of how write-in responses were collected. The only data available are from caregivers who attended at least one program session and who complied with instructions to submit home practice worksheets at least once during the intervention, which represented 56.3% of the full intervention sample. As such, caregivers who experienced barriers to program attendance or did not submit home practice worksheets were not included in the study, and their experience of home practice challenges are not represented in the current study. Study findings only reflect the challenges reported by caregivers who are already somewhat “bought-in” to the program goals and home practice objectives. Indeed, 91% of the caregivers in our sample attended three or four sessions, whereas 86% of the caregivers who did not submit a worksheet attended one or zero sessions. The full range of challenges experienced by caregivers when attempting to implement EBI skills at home are not represented here. It is plausible that cognitions/beliefs surrounding the EBI and assigned home practice may be much more frequently experienced among caregivers who do not attend the program or adhere to program instructions to complete and submit home practice worksheets. For this subset of caregivers, it may be most beneficial to first address barriers to session attendance before addressing home practice challenges. Additionally, though we attempted to systematically codify home practice challenges and document their frequency, our list of codes and domains are not exhaustive of caregiver challenges. Finally, study findings need to be replicated with a larger sample of responses and caregivers. In addition to the need for replication generally, it is possible that the current study was underpowered to detect factors associated with specific challenge domains. Relatedly, we could not examine factors associated with other challenge domains due to low base rates.
This is the first study to codify the challenges caregiver face when completing home practice of EBI-assigned skills. Despite the ubiquity and theoretical importance of home practice in caregiver-mediated treatment and prevention services, the challenges that caregivers face are under-documented, and strategies to overcome challenges have been non-specific. Understanding the challenges caregivers face continues to be a necessary step toward identifying and providing appropriate home practice implementation supports to caregivers.
Supplemental Material
sj-pdf-1-irp-10.1177_26334895211055994 - Supplemental material for What got in the way? Caregiver-reported challenges to home practice of assigned intervention skills
Supplemental material, sj-pdf-1-irp-10.1177_26334895211055994 for What got in the way? Caregiver-reported challenges to home practice of assigned intervention skills by Joanna J. Kim, Nancy A. Gonzales, Hardian Thamrin, Anne Mauricio, Mary Kuckertz and Daisy Camacho-Thompson in Implementation Research and Practice
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study was considered as having minimal risk at ethical review (Arizona State University Institutional Review Board, IRB ID: STUDY00000967). Participants were given written information and provided informed consent prior to participating in study procedures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse (grant number R01 DA035855, T32 DA039772).
Supplemental material
Supplemental material for this article is available online.
Trial registration
The parent clinical trial is registered at ClinicalTrials.gov (Identifier: NCT03125291, Registration date: 4/13/2017).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.