
Abstract
Background:
Substance use disorders (SUDs) among people with HIV are both prevalent and problematic. The Substance Abuse Treatment to HIV care project was funded to test the Implementation and Sustainment Facilitation (ISF) strategy as an adjunct to the Addiction Technology Transfer Center (ATTC) strategy for integrating a motivational interviewing-based brief intervention (MIBI) for SUDs within HIV community-based organizations.
Methods:
Using a cluster-randomized, type 2 hybrid trial design, 39 HIV organizations were randomized to either (1) ATTC (n = 19) or (2) ATTC + ISF (n = 20). Each HIV organization identified two staff members to be prepared to implement the MIBI (N = 78). Subsequently, during the implementation phase, HIV organizations in each condition randomized client participants (N = 824) to one of the two intervention conditions: usual care (UC; n = 415) or UC + MIBI (n = 409). Both staff-level outcomes and client-level outcomes were examined.
Results:
The ISF strategy had a significant impact on the implementation effectiveness (i.e., the consistency and the quality of implementation; β = .65, p = .01) but not on time-to-proficiency (β = −.02) or level-of-sustainment (β = .09). In addition, the ISF strategy was found to have a significant impact on the intervention effectiveness (the effectiveness of the MIBI), at least in terms of significantly decreasing the odds (odds ratio = 0.11, p = .02) of clients using their primary substance daily during follow-up.
Conclusion:
The ISF strategy was found to be an effective adjunct to the ATTC strategy in terms of implementation effectiveness and intervention effectiveness. It is recommended that future efforts to integrate the project’s MIBI for SUD within HIV organizations use the ATTC + ISF strategy. However, given the ISF strategy did not have a significant impact on level-of-sustainment, implementation research testing the extent to which the ATTC + ISF strategy can be significantly enhanced through effective sustainment strategies is warranted.
Plain language abstract
Substance use among people living with HIV is associated with increased mental health problems, worse medication adherence, and worse HIV viral suppression. Increasing substance use-related services in HIV community-based organizations is an important public health need. The Substance Abuse Treatment to HIV care project tested two strategies for helping HIV organizations implement a brief intervention (BI) designed to motivate clients to decrease their substance use. The project also tested if receiving a BI improved clients’ outcome. Two staff from each of the 39 participating organizations were taught how to deliver the BI using the Addiction Technology Transfer Center (ATTC) training strategy (online and in-person training, monthly feedback, and coaching). Half of the organizations also received the Implementation and Sustainment Facilitation (ISF) strategy, which included monthly meetings with an ISF coach for the two BI staff and one or more leadership staff from the organization. Organizations that received both the ATTC and ISF strategies delivered more BIs and higher quality BIs than organizations that only received the ATTC strategy. In addition, clients receiving BIs at organizations that received both strategies were more likely to decrease their substance use. However, receiving both strategies did not improve how quickly staff learned to deliver the BI or improve the number of BIs delivered during the project’s 6-month sustainment phase. Future research focused on implementing BIs within HIV organizations should consider using the ATTC and ISF strategies while also seeking to enhance the strategies to improve sustainment.
Keywords
Substance use among people with HIV is a significant public health issue given it has been found to be associated with increased psychiatric problems (Gaynes et al., 2008), poorer HIV viral suppression (Arnsten et al., 2002; King et al., 2009; Lucas et al., 2001), poorer HIV medication adherence (Azar et al., 2010; Friedman et al., 2009; Hendershot et al., 2009; Malta et al., 2008), and increased likelihood of engaging in risk behaviors that result in infection transmission to others (Hutton et al., 2019; Palepu et al., 2003; Satre et al., 2020). Increasing its public health significance further, research suggests approximately half of the people with HIV have a substance use disorder (SUD) (Hartzler et al., 2017).
Complementing HIV primary care, HIV community-based organizations (hereafter HIV organizations) provide medical and non-medical case management services and are a major source of care for people with HIV (U.S. Department of Health and Human Services, Health Resources and Services Administration, Bureau of Primary Health Care, 2017). Thus, in 2014, as part of its effort to help improve the integration of substance use services within HIV service settings, the National Institute on Drug Abuse funded the Substance Abuse Treatment to HIV care project. The project’s primary aim was to test the Implementation and Sustainment Facilitation (ISF) strategy as an adjunct to the Addiction Technology Transfer Center (ATTC) strategy for helping HIV organizations and their staff integrate a motivational interviewing-based brief intervention (MIBI) for SUDs. Given the importance of context (Aarons et al., 2011; Damschroder et al., 2009) and given research on the effectiveness of MIBIs for SUDs in HIV settings was limited (Aharonovich et al., 2006, 2012; Hasin et al., 2013), the project also examined the impact of the ISF strategy on intervention effectiveness (the effectiveness of the MIBI on improving client-level outcomes) (Garner, Gotham, et al., 2017; Helfrich et al., 2007; Klein et al., 2001; Klein & Sorra, 1996; Weiner et al., 2009). Written in accordance with both the Consolidated Standards of Reporting Trials (CONSORT) guidelines for cluster-randomized trials (Campbell et al., 2012) (see Supplemental File 1 for checklist) and the Standards for Reporting Implementation Studies (StaRI) guidelines (Pinnock et al., 2017) (see Supplemental File 2 for checklist), this article presents the main findings from the project.
Rationale for trial design
We used a cluster-randomized design (HIV organizations were the unit of randomization) to minimize the likelihood of contamination across the project’s two implementation conditions and because cluster-randomized designs had been noted as being preferred over other designs, including stepped-wedge designs (Kotz et al., 2012a, 2012b; Mdege et al., 2012). However, beyond the use of a cluster-randomized design, we used a type 2 hybrid trial design given Curran et al.’s (2012) recommendation of it as an innovative design “in support of more rapid translation” and to “provide more valid estimates of potential clinical effectiveness.”
Rationale for testing a MIBI for SUDs as an adjunct to usual care within HIV organizations
As highlighted by DiClemente et al. (2017), multiple reviews have supported the efficacy and effectiveness of MIBIs for reducing alcohol use (Kaner et al., 2009; Lundahl et al., 2010; McQueen et al., 2011; Stewart, 2012) and cannabis use (Baker et al., 2009, 2010; Dennhardt & Murphy, 2013; Lundahl et al., 2010). However, supporting our rationale for integrating a MIBI for SUDs within HIV service settings was research conducted within HIV service settings and found MIBIs can be effective for reducing alcohol use (Aharonovich et al., 2006; Hasin et al., 2013) and the use of other substances (Aharonovich et al., 2012).
To help maximize the external validity of the project and its findings, we aimed to examine the effectiveness of the project’s MIBI for SUD as an adjunct to usual care (UC) within HIV organizations (UC + MIBI compared with UC only). Regarding UC within HIV organizations, we found standardized substance use screening was rare, with it being even rarer for HIV organizations to employ staff adequately trained to address substance SUDs. Rather, we found UC for SUDs within HIV organizations was primarily referral to treatment.
Rationale for testing the ISF strategy as an adjunct to the ATTC strategy
The combination of staff training, performance feedback, and coaching has been found to be one of the most effective strategies for helping prepare individuals to implement MIBIs with proficiency (Barwick et al., 2012; Darnell et al., 2016; de Roten et al., 2013; Madson et al., 2009, 2019; Martino, 2010; Miller et al., 2004). The ATTC Network has long used this multifaceted strategy to help addiction treatment organizations improve the integration of motivational interviewing for SUDs. As such, the ATTC strategy was identified as one of the most promising strategies for helping HIV organizations and their staff integrate the project’s MIBI. However, given implementation and sustainment are acknowledged as multilevel processes (Aarons et al., 2011; Proctor et al., 2009), the ATTC strategy, which mostly focuses on individual staff training (i.e., staff-focused), was hypothesized to be necessary but not sufficient. Thus, building upon research that identified facilitation as a promising strategy (Baskerville et al., 2012; Cully et al., 2012; Gustafson et al., 2013; Harvey et al., 2002; Kauth et al., 2010; Kitson et al., 2008; Liddy et al., 2011; Owen et al., 2013; Parchman et al., 2013; Seers et al., 2012; Stetler et al., 2006), we aimed to test the ISF strategy, which focuses on training the staff in MIBI and the organization’s leadership (i.e., team-focused) to support MIBI implementation.
As detailed by Garner, Zehner, et al. (2017), the ISF strategy is a multifaceted strategy with facilitation as the overarching approach, encompassing six additional discrete strategies. Grounded in the theory of implementation effectiveness (Helfrich et al., 2007; Klein et al., 2001; Klein & Sorra, 1996; Weiner et al., 2009), the ISF strategy seeks to improve implementation effectiveness (the consistency and the quality of implementation of the clinical intervention) and intervention effectiveness (the clinical intervention’s effectiveness in terms of improving client outcomes) through improving implementation climate (the extent to which implementation is expected, supported, and rewarded). Guided by the Exploration-Preparation-Implementation-Sustainment (EPIS) framework (Aarons et al., 2011), we sought to expand the theory of implementation effectiveness in two ways. Specifically, by examining the extent to which the ISF strategy would help decrease staff time-to-proficiency and increase staff level-of-sustainment. In addition, the ISF strategy was grounded in motivational interviewing principles (Wagner & Ingersoll, 2012), which is similar to how Kauth et al. (2010) employed motivational interviewing techniques as part of their multifaceted facilitation strategy for improving the implementation of cognitive behavioral therapy. Thus, as part of each ISF strategy meeting, the ISF facilitator attempted to (1) engage the implementation team, (2) help focus the implementation team on the project’s key goal(s), (3) help evoke from the implementation team’s pros and cons related to the project’s key goal(s), and (4) help the implementation team plan how best to achieve the project’s key goals and sustain those achievements over time.
Primary aims and hypotheses
The primary aim of the project was to test the ISF strategy as an adjunct to the ATTC strategy for helping HIV organizations and their staff integrate a MIBI for SUDs. Guided by the theory of implementation effectiveness (Helfrich et al., 2007; Klein et al., 2001; Klein & Sorra, 1996; Weiner et al., 2009) and the EPIS framework (Aarons et al., 2011), we hypothesized that the ISF strategy would have significant impacts on three staff-level outcome measures (see Figure 1). In addition, as detailed by MacKinnon (2011), integrating moderators into research design is important to understand the generalizability by first examining the extent to which there are any differential effects that would impede interpretation of a main effect. Thus, consistent with the decomposed-first strategy (Preacher et al., 2016), we started with moderation-focused hypotheses to avoid biases associated with conflated effects. We hypothesized that the impact of the ISF strategy on these staff-level outcomes would be moderated by the components of the Consolidated Framework for Implementation Research’s (CFIR) (Damschroder et al., 2009) characteristics of individuals domain (prior experience with motivational interviewing, personal recovery status) and inner setting domain (implementation climate, implementation readiness, and leadership engagement). Finally, we hypothesized that the ISF strategy would moderate the effect of MIBI on client outcomes.
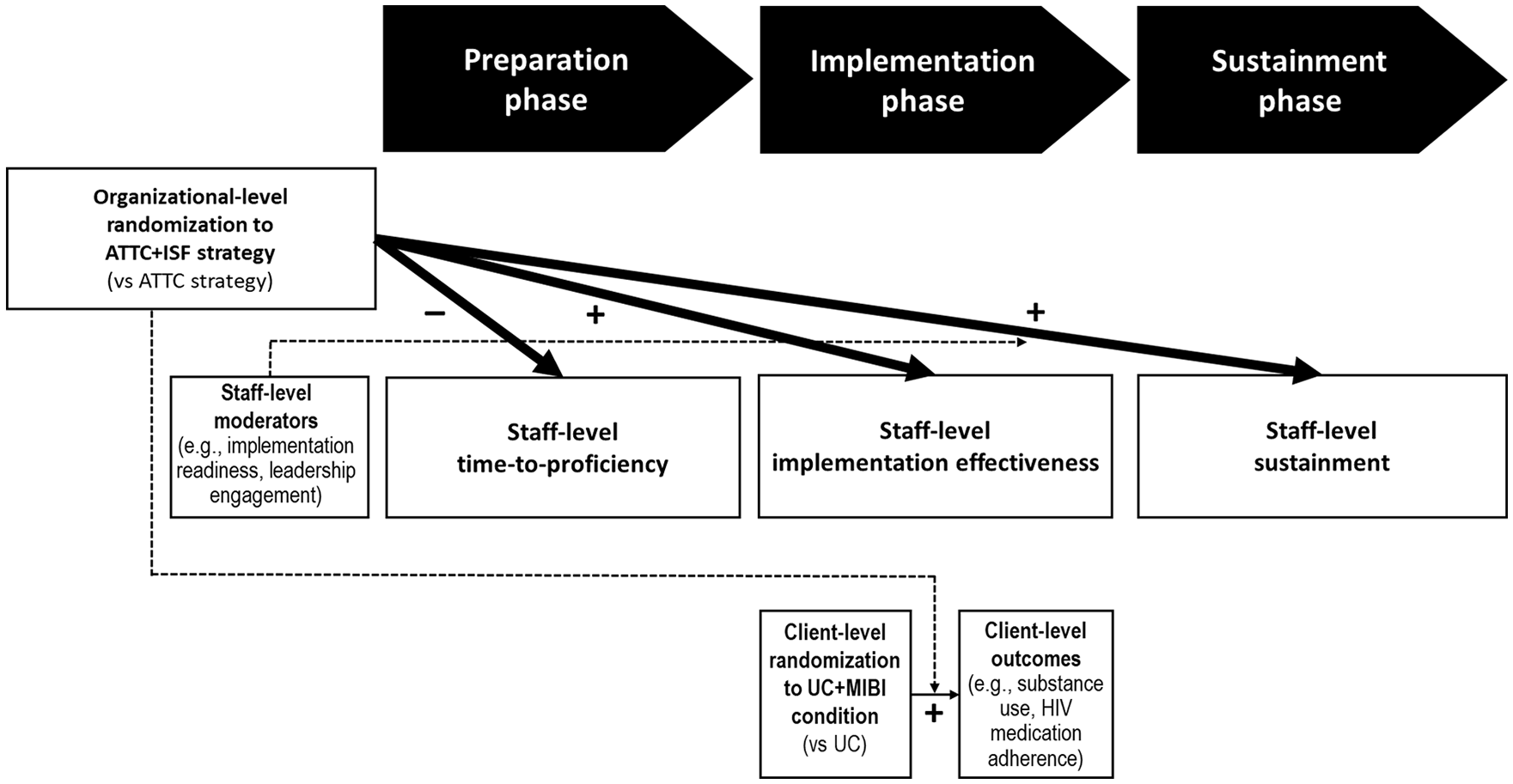
Aims and hypotheses.
Methods
Trial design
The trial design was a cluster-randomized, type 2 hybrid trial. Following an exploration phase in which HIV organizations were recruited, HIV organizations (and their staff) were randomized to one of the two strategies: (1) the ATTC strategy or (2) the ATTC + ISF strategy. Following randomization, the trial was deployed using a multiphase design that included three 6-month phases corresponding to the preparation, implementation, and sustainment phases of the EPIS framework (Aarons et al., 2011). During the implementation phase, HIV organizations recruited and randomized client participants to one of the two clinical intervention conditions: UC or UC + MIBI. Institutional Review Board (IRB) approval and oversight of all research activities were provided by RTI International’s IRB.
Context
HIV organizations, located in 23 states and the District of Columbia within the United States, provided the context for the project.
Participants
Staff participants
To be eligible to participate, an HIV organization was required to serve a minimum of 100 individuals living with HIV per year; have at least two staff members willing to be prepared to implement a MIBI for SUDs; and have at least one leadership staff member (e.g., supervisor, manager, director) willing to help ensure that MIBI staff were given sufficient time to participate. There were no exclusion criteria. Each collaborating HIV organization identified two staff to be prepared to implement the MIBI as part of the project’s implementation phase and to be recruited for participation in staff surveys. Each HIV organization also identified one to three leadership staff to be recruited for participation in staff surveys. After staff provided informed consent, which was obtained electronically, staff completed surveys prior to randomization (before the preparation phase), after the implementation phase (Month 13), and after the sustainment phase (Month 19), and received a US$25 e-gift card per survey. For more details, see the study protocol paper (Garner, Zehner, et al., 2017).
Client participants
Client eligibility was assessed by HIV organization staff through the project’s standardized screener. Eligibility criteria included having been diagnosed with HIV; being above 18 years of age; and acknowledging the use of at least one substance in the past 28 days with self-reported endorsement of two or more of the 11 Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria (American Psychiatric Association, 2013) for SUD for that substance during the past 12 months. An exclusion criterion was not being able to speak English, which was due to the project’s research staff and MIBI proficiency raters being monolingual. Clients who met eligibility criteria were recruited for study participation by one of the several trained HIV organization staff. It was one of the two MIBI staff members from each HIV organization who was trained to obtain written informed consent, administer the baseline assessment, follow-up locator form, and open the randomization envelope with client participants. Each HIV organization was provided compensation to cover staff time to complete these research-related activities. Clients randomized to the UC + MIBI condition received the MIBI at no cost. Clients received a US$20 gift card for completing the baseline assessment and US$20 for completing a 4-week follow-up assessment administered by research staff blinded to all condition assignments.
Implementation strategies
Complementing the comprehensive descriptions provided as part of the open-access study protocol paper (Garner, Zehner, et al., 2017) and information provided at www.ISFstrategy.org, Table 1 defines and specifies the 10 discrete strategies in the ATTC strategy, as well as the 7 discrete strategies in the ISF strategy. For the ATTC strategy, the HIV organization’s two recipient MIBI staff were given the opportunity to receive 12 months of MIBI training and technical assistance: training (5-hr online didactics and 2-day in-person workshop), performance feedback (standardized feedback on one to three MIBIs during the preparation phase and standardized feedback on all MIBIs during the implementation phase), and consultation (up to three 1-hr individual consultation calls during the preparation phase and monthly 1-hr group consultation calls during the implementation phase). Thus, the maximum possible dose of the ATTC strategy was 30 hr per MIBI staff. For the ISF strategy, the HIV organization’s recipient MIBI staff and leadership staff were given the opportunity to receive 18 months of external facilitation led by one of the project’s ISF facilitators (monthly virtual meetings lasting up to 60 min, up to two in-person facilitation meetings lasting up to 6 hr each). Thus, the maximum possible dose of the ISF strategy was 30 hr for each of the HIV organization’s staff working on the project. To maximize the extent to which the ISF strategy was implemented with consistency and quality, the project’s lead developer of the ISF strategy trained each ISF facilitator, reviewed randomly selected ISF session recordings (each virtual ISF facilitation meeting was video-recorded for the quality assurance purposes), and regularly supervised the ISF facilitators (no less than monthly, usually weekly).
Discrete strategies included within the ATTC strategy and the ISF strategy.

Note. See the study protocol paper (Garner, Zehner, et al., 2017) for justification of each discrete strategy. ATTC = Addiction Technology Transfer Center; ISF = implementation and sustainment facilitation; MIBI = motivational interviewing-based brief intervention.
Clinical interventions
UC consisted of referral to formal addiction treatment, mutual help services, or both. Clients randomized to UC + MIBI received the project’s 20- to 30-min MIBI for SUD provided by one of the HIV organization’s prepared/trained MIBI staff. The MIBI was designed to motivate individuals living with HIV who have an SUD to change their substance use by examining their reasons for change, receiving feedback about common negative interactions of substance use and HIV-related health issues, further developing the importance or confidence to reduce or stop their primary substance use, and making a plan for change. For more details, see the study protocol paper (Garner, Gotham, et al., 2017).
Outcome measures
Organized by phase (preparation phase, implementation phase, and sustainment phase), Table 2 details the staff-level outcome measures (time-to-proficiency, implementation effectiveness, and level-of-sustainment) and client-level outcome measures (days of primary substance use, number of substance-related problems, times engaging in risky behaviors, days of substance use treatment, and days of medication non-adherence) collected.
Outcome measures.

Note. Intervention effectiveness was assessed in terms of the impact of the ISF strategy on each of the client outcome measures. MIBI = motivational interviewing-based brief intervention; SUD = substance use disorder; MI = motivational interviewing; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, 5th ed.
Moderator measures
Table 3 details the staff-level measures (implementation readiness, implementation climate, leadership engagement, tension-for-change, motivational interviewing experience, and personal recovery status) hypothesized to moderate the impact of the ISF strategy on the staff-level outcomes.
Staff-level moderator measures.

Note. MIBI = motivational interviewing-based brief intervention; SUD = substance use disorder.
Targeted sample size
The targeted sample size was estimated through power analyses with Optimal Design Software (Raudenbush et al., 2011). For analyses of staff-level outcomes, it was estimated that 78 MIBI staff nested within 39 HIV organizations would provide 80% power to detect a statistically significant (p < .05) difference for effect sizes .67 or greater (Garner, Zehner, et al., 2017). For analyses of client-level outcomes, it was estimated that 1,872 clients, nested within 78 MIBI staff members, nested within 39 HIV organizations would provide 80% power to detect a statistically significant difference for effect sizes .20 or greater (Garner, Gotham, et al., 2017).
Randomization sequence generation
For randomization of HIV organizations (the clusters), each HIV organization was allocated to one of the two implementation strategy conditions (ATTC; ATTC + ISF) through an urn randomization process (Stout et al., 1994). Specifically, using survey data collected during the exploration phase from HIV organization staff, seven organizational-level factors (importance of substance use screening, importance of brief intervention for substance use, innovation-value fit, implementation strategy-value fit, implementation climate for MIBI, implementation readiness for MIBI, and implementation effectiveness for MIBI) were entered into an urn randomization program (Charpentier, 2003) that optimized the balance of the two implementation strategy conditions based on these factors.
During the project’s implementation phase, HIV organizations randomized client participants to one of the two intervention conditions (UC; UC + MIBI) through a blocked randomization sequence (blocking size of 6) generated through a blocked randomization program (Sealed Envelope, n.d.). Within each participating HIV organization, each MIBI staff had a lock box containing 36 sequentially numbered tamper-evident security envelopes containing a randomization slip indicating condition assignment. The randomization envelope was opened in front of the client participant. Staff updated a centralized recruitment tracking log monitored multiple times per week by research staff.
Blinding
It was not possible to blind HIV organizations and their staff to the assigned implementation strategy condition, but the project’s ATTC strategy staff and quality raters were blinded to implementation strategy condition assignment. In addition, it was not possible to blind HIV organizations, their staff, or client participants to clinical intervention condition assignment, but the project’s research staff who conducted the follow-up assessments were blinded to all condition assignments.
Statistical methods
Statistical analyses were conducted using an intention-to-treat approach. Staff-level outcomes were approximately normal, and within-site variation was close to zero. A series of multilevel adjusted analyses was conducted, each of which controlled for project cohort and was weighted through a propensity score weight derived by regressing implementation strategy condition assignment on staff characteristics. The interaction between the implementation strategy condition assignment and each hypothesized moderator was examined first, with main effects examined as appropriate.
Client-level outcomes had strong floor effects (0 of 28 days) and/or strong ceiling effects (28 of 28 days), which led to bimodal u-shaped, j-shaped, or inverted j-shaped distributions. Given these non-normal distributions, linear regression analyses were not appropriate. Rather, these types of distributions are appropriately addressed using zero-and-one inflated beta regression after data are transformed to a proportion scale (0 to 1). This model is a mixture model with three parts: a prediction of the probability of the ceiling effect vs. other values (the ceiling effect), a prediction of the mean for values in between, but not including, the floor and ceiling effect (non-ceiling/non-floor effect), and a prediction of the probability of the floor effect vs. other values (the floor effect). We fit three-level multilevel models to account for the nesting of client participants within MIBI staff and MIBI staff within HIV organizations using the R package (Liu & Kong, 2015). Each model was adjusted for the baseline value of the respective outcome measure, client characteristics (i.e., age, White, male, heterosexual, transgender, married, high school or higher, alcohol as primary substance, and engagement in HIV care), project cohort, randomization to ATTC + ISF condition, randomization to UC + MIBI condition, and the cross-level interaction between ATTC + ISF condition and UC + MIBI condition.
Results
Participant flow and recruitment
HIV organizations were recruited in three cohorts, each lasting 20 months from the randomization of HIV organizations to the final data collection. The first cohort, in the central United States, occurred from January 2015 through August 2016 and resulted in the recruitment of 14 HIV organizations, 28 MIBI staff, and 191 client participants. The second cohort, in the western United States, occurred from January 2016 through August 2017 and resulted in the recruitment of 11 HIV organizations, 22 MIBI staff, and 300 client participants. The third cohort, in the eastern United States, occurred from January 2017 through August 2018 and resulted in the recruitment of 14 HIV organizations, 28 MIBI staff, and 333 clients. Figure 2 details the flow of HIV organizations, MIBI staff, and client participants through the project’s preparation, implementation, and sustainment phases. Although similar numbers of staff were recruited across conditions, about twice as many clients were screened, enrolled, and randomized within the ATTC + ISF condition.

Participant flow.
Baseline characteristics
Table 4 presents baseline characteristics for MIBI staff participants for the overall sample (N = 78) and each condition (ATTC = 38; ATTC + ISF = 40). Overall, MIBI staff participants were 25–34 years of age (46%), female (71%), Caucasian/White (62%), a graduate degree or higher (50%), 12 months or less tenure with current HIV organization (35%), and intermediate motivational interviewing experience or higher (53%).
Staff characteristics at baseline.

Note. ATTC = Addiction Technology Transfer Center; ISF = implementation and sustainment facilitation; MI = motivational interviewing; SD = standard deviation.
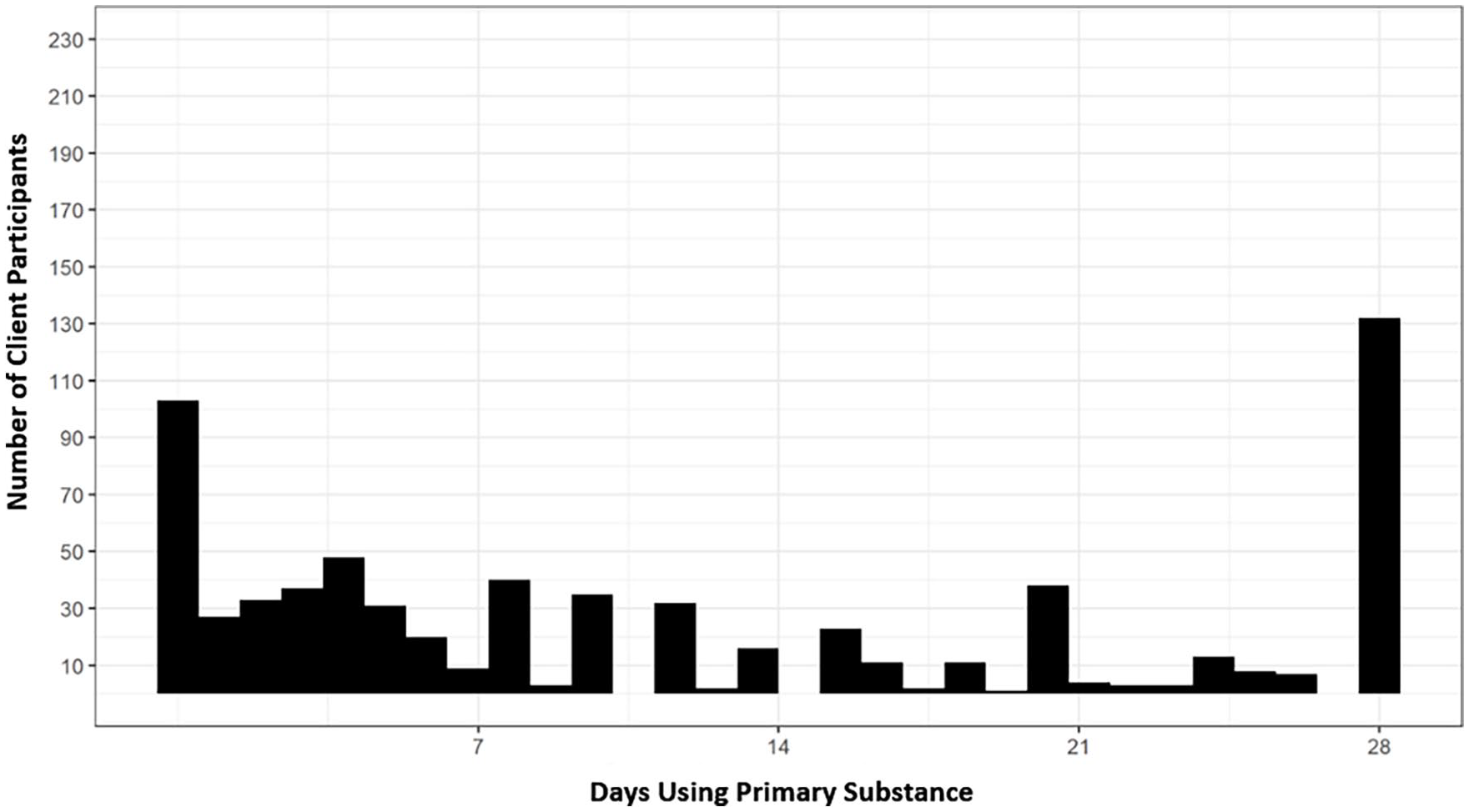
Table 5 presents the baseline characteristics for client participants for the overall sample (N = 824) and each condition (ATTC and UC = 134; ATTC and UC + MIBI = 130; ATTC + ISF and UC = 281; ATTC + ISF and UC + MIBI = 279). Overall, clients were male (76%), African American/Black (54%), heterosexual (42%), a high school graduate or higher (70%), and engaged in HIV care (95%). Primary substance use for the overall sample was alcohol (37%), cannabis (23%), cocaine/crack (18%), methamphetamine (17%), heroin (2%), and other (3%). On average, client participants reported using their primary substance 16 days during the past 28 days (57% of days). However, 222 (27%) of client participants reported using their primary substance daily during the past 28 days (see Figure 3).
Client characteristics at baseline.

Note. ATTC = Addiction Technology Transfer Center; UC = usual care; MIBI = motivational interviewing-based brief intervention; ISF = implementation and sustainment facilitation; SD = standard deviation; SUD = substance use disorder.

Baseline distribution for client’s days of primary substance use.
Implementation strategy dose
Regarding the ATTC strategy, the average dose (measured in hours) per MIBI staff was 23.85 hr (SD = 1.62) for the ATTC condition and 25.02 hr (SD = 1.63) for the ATTC + ISF condition. Regarding the ISF strategy, the average dose (also measured in hours) was 9.29 hr (SD = 2.83) for MIBI staff and 4.83 hr (SD = 3.09) for leadership staff.
Outcomes
Table 6 summarizes results of analyses focused on testing the extent to which the ISF strategy had an impact on the staff-level outcomes. Consistent with our hypotheses, results of each moderator analysis are presented first, with a main effect analysis reported as appropriate.
Moderator-first analyses of the impact of the ISF strategy on time-to-proficiency, implementation effectiveness, and level-of-sustainment.

Note. ISF = implementation and sustainment facilitation; ICC = intracluster correlation; CI = confidence interval; SE = standard error; MI = motivational interviewing; ATTC = Addiction Technology Transfer Center.
For time-to-proficiency, none of the hypothesized moderators were found to be significant. Furthermore, the ISF strategy was not found to have a significant main effect on decreasing time-to-proficiency, β = −.02, 95% confidence interval (CI) = [−0.41, 0.37]. On average, time-to-proficiency was 12.35 days (SD = 3.18) for MIBI staff in the ATTC condition and 11.44 days (SD = 4.87) for MIBI staff in the ATTC + ISF condition.
For implementation effectiveness, none of the hypothesized moderators were found to be significant. However, the ISF strategy was found to have a significant main effect on increasing implementation effectiveness, β = .65, 95% CI = [0.25, 1.05], p < .01. On average, the sum number of MIBIs implemented during the implementation phase (the consistency dimension of staff-level implementation effectiveness) was 3.32 (SD = 4.13) for MIBI staff in the ATTC condition and 6.93 (SD = 5.49) for MIBI staff in the ATTC + ISF condition. On average, the sum quality score of MIBIs (the quality dimension of staff-level implementation effectiveness) was 560 (SD = 780) for MIBI staff in the ATTC condition and 1,324 (SD = 1,054) for MIBI staff in the ATTC + ISF condition.
For level-of-sustainment, none of the six hypothesized moderators were found to be significant, and there was not a significant main effect for the ISF strategy, β = .09, 95% CI = [−0.42, 0.60]. On average, the number of MIBIs implemented during the sustainment phase was 3.42 (SD = 6.31) for MIBI staff in the ATTC condition and 3.18 (SD = 8.33) for MIBI staff in the ATTC + ISF condition.
Table 7 summarizes results of analyses focused on testing the extent to which the ISF strategy had an impact on the effectiveness of the MIBI to improve client outcomes. Consistent with our hypotheses, the cross-level interactions between implementation condition and clinical intervention condition are presented first, with the other key terms presented below.
Cross-level interactions examining the impact of the ISF strategy on the intervention effectiveness of the MIBI.

Note. • indicates variable removed to allow model to converge. Ceiling effects were excluded for outcomes without a ceiling effect. Times engaging in risk behavior have no theoretical ceiling. Past 28 days substance use treatment does have an actual ceiling at 28, but it was so infrequently observed in the data that a ceiling effect did not result. ISF = implementation and sustainment facilitation; MIBI = motivational interviewing-based brief intervention; ICC = intracluster correlation; OR = odds ratio; CI = confidence interval; UC = usual care; ATTC = Addiction Technology Transfer Center.
For days of primary substance use (see Figure 4 for the distribution at follow-up), the ISF strategy had a significant impact on the effectiveness of the MIBI, at least in terms of significantly decreasing the odds, (odds ratio [OR] = 0.11, 95% CI = [0.08, 0.15], p = .01) of clients using their primary substance daily during the 28-day follow-up period. To help interpret the size of this effect, an OR of 0.11 is equivalent to an OR of 9.09 (1/0.11 = 9.09), which is considered a large effect (Chen et al., 2010). The ISF strategy increased the odds (OR = 1.51) of clients being completely abstinent from their primary substance at follow-up, but this small effect was not statistically significant. Complementing the results shown in Table 7, Figure 5 helps visualize the cross-level interaction between implementation condition and intervention condition on days of primary substance use.
Follow-up distribution for client’s days of primary substance use.

The impact of the ISF strategy on intervention effectiveness.
The ISF strategy was not found to have a significant impact on the effectiveness of the MIBI for the other client outcome measures. However, there were significant effects for the ATTC + ISF strategy on clients’ endorsement of problems related to their primary substance (problem recognition), which is important, yet distinct from the effectiveness of the MIBI (intervention effectiveness). Specifically, the ATTC + ISF strategy increased the odds of client participants endorsing that their primary substance was associated with each of the 11 DSM-5 symptoms (ceiling effect; OR = 6.68, 95% CI = [5.39, 8.28], p = .01) and the number of the 11 DSM-5 symptoms endorsed for client participants without a ceiling/floor effect (OR = 1.36, 95% CI = [1.09, 1.68], p = .01).
Discussion
We used a cluster-randomized, type 2 hybrid trial to simultaneously test the impact of the ISF strategy (as an adjunct to the ATTC strategy) on (1) the integration of a MIBI for SUDs within HIV organizations across the United States and (2) the effectiveness of the MIBI (as an adjunct to UC within HIV organizations). Contributing to the growing literature on the effectiveness of facilitation-based strategies (Chinman et al., 2015, 2017; Jones et al., 2015; Kilbourne et al., 2014, 2015; Kirchner et al., 2014; Lessard et al., 2015; Liddy et al., 2015; Seers et al., 2018) and the effectiveness of MIBIs for SUD within HIV service settings (Aharonovich et al., 2012, 2017; Haldane et al., 2018; Hasin et al., 2014; Kahler et al., 2018; Scott-Sheldon et al., 2017; Wray et al., 2016), we found at least two findings of significance. First, we found evidence that the ISF strategy had a significant impact on improving the consistency and quality of MIBI implementation during the implementation phase (implementation effectiveness). Second, we found evidence that the ISF strategy had a significant impact on improving the effectiveness of the MIBI (intervention effectiveness). However, our main findings also included null results. Indeed, we did not find support for our hypotheses that staff-level measures of the inner setting domain (implementation readiness, implementation climate, leadership engagement, and tension-for-change) and characteristics of individuals domain (motivational interviewing experience and personal recovery status), two of the key CFIR domains (Damschroder et al., 2009), moderated the impact of the ISF strategy. Although these measures were not found to moderate the impact of the ISF strategy, we posit it remains possible one or more of these measures may mediate (i.e., help explain) the impact of the ISF strategy on implementation effectiveness, which has been explicitly hypothesized. As such, subsequent mediational analyses are warranted. In addition, we did not find support for our hypotheses that the ISF strategy would significantly decrease time-to-proficiency and significantly increase the level-of-sustainment. Organized in chronological order along the EPIS continuum (Aarons et al., 2011), below we discuss the limitations, generalizability, and implications of our findings (Campbell et al., 2012; Pinnock et al., 2017).
In terms of time-to-proficiency, we did not find evidence supporting our hypotheses. However, we believe that the potential for the ISF strategy to decrease time-to-proficiency was limited by requiring MIBI staff to demonstrate proficiency before they were allowed to help implement/test the project’s MIBI for SUDs and/or instructing MIBI staff to demonstrate MIBI proficiency sometime before the beginning of the project’s implementation phase, rather than as soon as possible. As such, our findings may or may not generalize to contexts in which there is a stronger justification for staff demonstrating MIBI proficiency as soon as possible (e.g., fee-for-service contexts). In terms of implications, this finding advances knowledge regarding the preparation of staff to implement a MIBI for SUDs and highlights the need for research experimentally testing the extent to which strategies minimize the time to complete key activities (Saldana et al., 2012) and the extent to which the impact of these strategies is significantly moderated by constructs hypothesized to be important (Damschroder et al., 2009).
Consistent with our time-to-proficiency finding, we did not find evidence to support our moderation-focused hypotheses regarding the impact of the ISF strategy on implementation effectiveness. We did, however, find evidence that the ISF strategy significantly improved the average level of implementation effectiveness achieved by MIBI staff. An early indicator of the impact of the ISF strategy on this outcome was the finding that about twice as many clients were screened, enrolled, and randomized within the ATTC + ISF condition (see Figure 1). A potential limitation of this finding is that MIBI staff were asked to limit the number of MIBIs implemented to three per month. This was done to help increase the likelihood that the monthly performance feedback and group consultation provided as part of the ATTC strategy could have an impact on MIBI quality, which is important given implementation effectiveness is defined as the both the consistency (i.e., the number of MIBIs implemented) and quality (i.e., the adherence and competence to the MIBI protocol) of implementation (Garner, Zehner, et al., 2017; Klein et al., 2001; Klein & Sorra, 1996). Although we believe this approach was well-justified, our findings may not generalize to less controlled contexts or contexts in which the quality component of implementation effectiveness is not using the Independent Tape Rater Scale to measure MIBI quality. Nonetheless, a key implication of this finding is that the ISF strategy was a promising adjunct to the ATTC strategy, at least for improving the implementation of our project’s MIBI for SUDs within HIV organizations. Thus, it is recommended that intermediary/purveyor organizations seeking to improve the integration of a MIBI for SUD within HIV organizations, such as the AIDS Education and Training Center network, consider use of the ATTC + ISF strategy for such efforts.
Consistent with prior research highlighting that variation in implementation influences program outcomes (Durlak & DuPre, 2008; Garner et al., 2016), we found that in addition to significantly improving implementation effectiveness, the ISF strategy significantly improved the intervention effectiveness. Notwithstanding the importance of this finding, it is important to note that the ISF strategy’s impact on the effectiveness of the project’s MIBI for SUDs was limited to a single client outcome, days of primary substance use. Unfortunately, less than optimal recruitment and randomization of client participants, which has recently been highlighted as a key potential drawback of type 2 hybrid trials (Landes et al., 2019), limited our power to detect statistically significantly differences in the study’s other client outcome measures. Other noteworthy limitations are that the days of primary substance use and the other client outcome measures were based on client self-report and limited to a 4-week follow-up period. To the best of our knowledge, we are the first to have experimentally tested the impact of an implementation strategy on intervention effectiveness (i.e., the cross-level impact of an implementation strategy on the relative effectiveness of the experimental clinical intervention compared to the control clinical intervention), which is distinct from our prior implementation research that tested the impact of an implementation strategy on client outcomes (i.e., the direct impact of the implementation strategy to improve client outcomes relative to the control implementation strategy; Garner et al., 2012). Thus, the generalizability of our findings may need to be limited to contexts similar to our current study. The key implication of this finding is that future efforts to improve the integration of MIBIs for SUDs within HIV organizations, both implementation research and implementation practice, should consider the use of the ATTC + ISF strategy. Finally, Foy et al. (2015) noted, “If studies evaluating the effects of implementation intervention are to be of relevance to policy and practice, they should have endpoints related to evidence-based processes of care, patient outcomes, or population outcomes.” Thus, another implication of our finding is the need for more type 2 hybrid trials that enable tests of impact on intervention effectiveness, which is arguably one of the most relevant endpoints of all.
Although the level-of-sustainment is not possible without some level of implementation effectiveness occurring first, the level-of-sustainment is another endpoint of significant relevance (Chambers et al., 2013; Proctor et al., 2015; Stirman et al., 2012). Thus, it is significant to note that we did not find support for our hypotheses related to the level-of-sustainment, and the average level-of-sustainment was not only similar between conditions but was also relatively low (only three MIBIs during the 6-month sustainment period). The key limitation associated with this finding is that level-of-sustainment was based on self-report from MIBI staff. It does not appear that self-report led to MIBI staff overestimating their level-of-sustainment. Our level-of-sustainment finding was also limited by not being able to measure the extent to which MIBIs were implemented with quality. Conservatively, the generalizability of our findings should be limited to efforts to testing the impact of the ISF strategy as an adjunct to the ATTC strategy or the level-of-sustainment of a MIBI for SUDs within HIV organizations. However, we believe our findings generalize more broadly to research that has advanced knowledge regarding sustainment (Hunter et al., 2015, 2017). Arguably, sustainment is one of the most important outcomes to identify the effective strategies for, especially given that the lack of sustainment minimizes the return-on-investments for resources expended during prior phases along the EPIS continuum (exploration phase, preparation phase, and implementation phase) (Aarons et al., 2011). Thus, a key implication is that future research is needed to test strategies that can significantly improve both the relative effectiveness of the ATTC + ISF strategy on the level-of-sustainment and the extent to which the ATTC + ISF strategy improves the absolute level-of-sustainment.
In conclusion, although the ATTC strategy was found to be sufficient for the preparation of HIV organization staff to implement a MIBI for SUDs, the ISF strategy was found to be an effective adjunct to the ATTC strategy in terms of both implementation effectiveness and intervention effectiveness. Based on these findings, future implementation research and practice focused on integrating a MIBI for SUD within HIV organizations should consider using the ATTC + ISF strategy. However, given the ISF strategy did not have a significant impact on the level-of-sustainment, which was similarly low in both implementation conditions, we also conclude that future efforts should seek to enhance the ATTC + ISF strategy through strategies focused on improving the level-of-sustainment during the sustainment phase.
Supplemental Material
Supplemental_File_1_-_FINAL – Supplemental material for The implementation and sustainment facilitation strategy improved implementation effectiveness and intervention effectiveness: Results from a cluster-randomized, type 2 hybrid trial
Supplemental material, Supplemental_File_1_-_FINAL for The implementation and sustainment facilitation strategy improved implementation effectiveness and intervention effectiveness: Results from a cluster-randomized, type 2 hybrid trial by Bryan R Garner, Heather J Gotham, Michael Chaple, Steve Martino, James H Ford II, Mathew R Roosa, Kathryn J Speck, Denna Vandersloot, Michael Bradshaw, Elizabeth L Ball, Alyssa K Toro, Christopher Griggs and Stephen J Tueller in Implementation Research and Practice
Supplemental Material
Supplemental_File_2_-_FINAL – Supplemental material for The implementation and sustainment facilitation strategy improved implementation effectiveness and intervention effectiveness: Results from a cluster-randomized, type 2 hybrid trial
Supplemental material, Supplemental_File_2_-_FINAL for The implementation and sustainment facilitation strategy improved implementation effectiveness and intervention effectiveness: Results from a cluster-randomized, type 2 hybrid trial by Bryan R Garner, Heather J Gotham, Michael Chaple, Steve Martino, James H Ford II, Mathew R Roosa, Kathryn J Speck, Denna Vandersloot, Michael Bradshaw, Elizabeth L Ball, Alyssa K Toro, Christopher Griggs and Stephen J Tueller in Implementation Research and Practice
Footnotes
Authors’ note
This project would not have been possible without both the participation and collaboration of the project’s 39 organizations and their dedicated staff, as well as the participation of the organization’s client participants. In addition, this project would not have been possible without the assistance of the following: Tracy Karvinen, Traci Rieckmann, Matthew Orndorff, David Kaiser, Mark Zehner, and Marianne Kluckmann.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute On Drug Abuse of the National Institutes of Health under Award Number R01DA038146.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.