
Abstract
The purpose of this study was to investigate changes in the palatal form in patients treated with and without premolar extractions. A total of 40 patients who had undergone orthodontic treatment (extraction and non-extraction) were divided into two groups coequally. Retrospective records were collected at pretreatment and at bracket removal. Stone casts were scanned by cone-beam tomography; linear and angular measurements on the three-dimensional model were then performed for both the sagittal direction and the transverse direction. Paired t-tests for dependent samples were used to compare results within the same group, and t-tests for independent samples were used to compare results between groups. A p value less than 0.05 was considered statistically significant. The sagittal palatal form increased in the non-extraction group, whereas it decreased in the extraction group. There was a decrement in the transversal palatal form in both groups. There were no differences or changes in molar or canine crown angulation in the non-extraction group. Conversely, distal tipping of the upper right first molar and distal tipping and lingual movement of both left and right upper canines were observed in the extraction group.
Keywords
Introduction
Orthodontic treatment aims to straighten up teeth, provide a proper occlusal relationship between teeth, and maintain healthy orofacial functions. Crowding of dental arches occurs as a result of arch size discrepancies, tooth size discrepancies, and sometimes transverse arch discrepancies. Such discrepancies, however, may negatively affect psychological well-being, as they can impair individuals’ appearance, speech, and stomatognathic system functions. 1 –3
Therefore, relieving crowded arches and correcting malocclusion are ways of providing pleasing aesthetics and proper occlusal stability. Several methods can be employed to relieve crowded arches and correct malocclusion. A permanent tooth/teeth can be extracted or the dental arches can be expanded to provide enough space for teeth to align properly; however, there has been a huge debate on whether to extract the teeth in question, and the debate is as old as the specialty of orthodontics. The decision on such a debate is influenced by many factors, such as the appearance of the patient’s smile, the patient’s bone support, the duration of the treatment, and the long-term stability of the orthodontic treatment. 4 –9
The oral cavity represents a functional unit, as stated by Engelhardt. It consists of five parts: the teeth, the periodontium, the temporomandibular joints, the salivary glands, and the musculature. The musculature consists of five parts, which are chewing, tongue, palatal, pharynx, and facial musculature. If the mouth’s functional harmony is satisfactory, then a stable situation is achievable because the single structure has mutual responses. These reciprocal effects are potent and can cause an orthodontic treatment process to be clearly successful over a long period of time, given only the stomatognathic system. Changes in teeth position and angulation should lead to changes in tongue posture, which results from the changes in palate shape, volume, and height. Moreover, the success of orthodontic therapy is evaluated in terms of the long-term stability of the orthodontic treatment results, which is achieved by maintaining proper teeth angulation, proper teeth occlusion, and a well-balanced stomatognathic system 10
A promising, yet less explored, method of altering the effective relation between the tooth material and the basal bone can be accomplished through the change in axial relation of the crown of the tooth in the mesiodistal direction. Andrews, 11 in 1972, emphasized the significance of crown angulation and inclination in the attainment of optimum occlusion. Andrews postulated that the degree of crown angulation—especially in the maxillary anterior crowns, owing to their trapezoidal morphology—determines the amount of mesiodistal space the crowns occupy within the arch; thus, it has potential space implications.
With the evolution and the development of imaging techniques delivered from capturing three-dimensional models of plaster casts using cone-beam tomography or digital laser scans, a more accurate and less time-consuming measurement can easily be obtained. 12 –14
This study aimed to evaluate the transversal and sagittal palatal form changes in crown angulation on three-dimensional models taken before and after treatment of patients with their first premolar extraction and without extraction. Thus, the study aimed to provide data that might prove valuable to clinicians deciding whether to extract teeth based on changes to the palate form that might occur, affecting the long-term stability of the orthodontic treatment.
Materials and methods
In this study, 40 patients were treated for the orthodontic treatment of decomposition. The patients were divided into two groups for the experiment: group (A) and group (B). Group (A) comprised 20 patients, who were treated with conventional methods and without extraction of premolars; group (B) comprised 20 patients, who were treated with conventional methods and with extraction of premolars.
The patients in each group were examined for sagittal, transversal, and molar angulation changes before and after orthodontic treatment.
The present study included 80 pre- and posttreatment maxillary plaster casts of 40 completed cases in the permanent dentition phase, managed with fixed mechanotherapy.
The maxillary casts were retreated from the archive of treated cases who underwent treatment as outpatient in the Department of Orthodontics at Near East University in the Turkish Republic of Northern Cyprus. From the archive, pre- and posttreatment maxillary casts of the same cases were taken and then duplicated as digital analogues using cone-beam computed tomography. NewTomCCD (3G) (Verona, Italy) was used to scan the casts.
Sagittal palatal form
To calculate the changes that occurred within the sagittal palatal form during the treatment of extraction and non-extraction cases, anatomical points were identified and adopted in the sagittal measurement, such as right and left maxillary tuberosity. A straight line was drawn up between maxillary tuberosity right and maxillary tuberosity left; the length of the distance between the right and left tuberosity was then calculated.
A new point was then identified, which is the midpoint between the right and left maxillary tuberosity. This point was considered the starting point for measuring the length of the sagittal palatal form toward all the medial lingual gingival borders of 12 + 13 + 14 + 15 + 16 + 22 + 23 + 24 + 25 + 26 and the incisive papilla, as depicted in Figure 1.

Illustration of sagittal and transverse linear measurements.
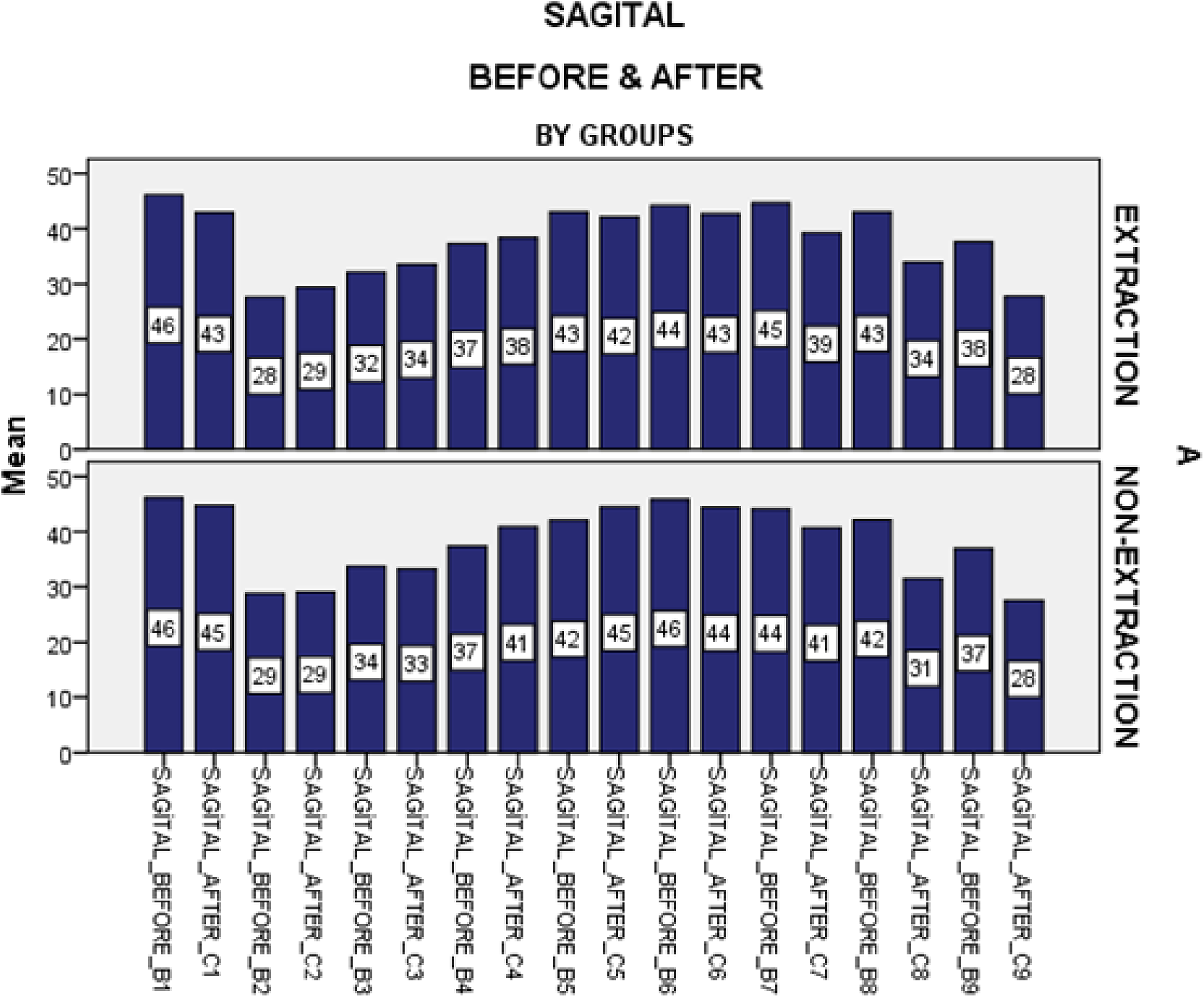
Sagittal dimension before and after, in extraction and non-extraction treatments.
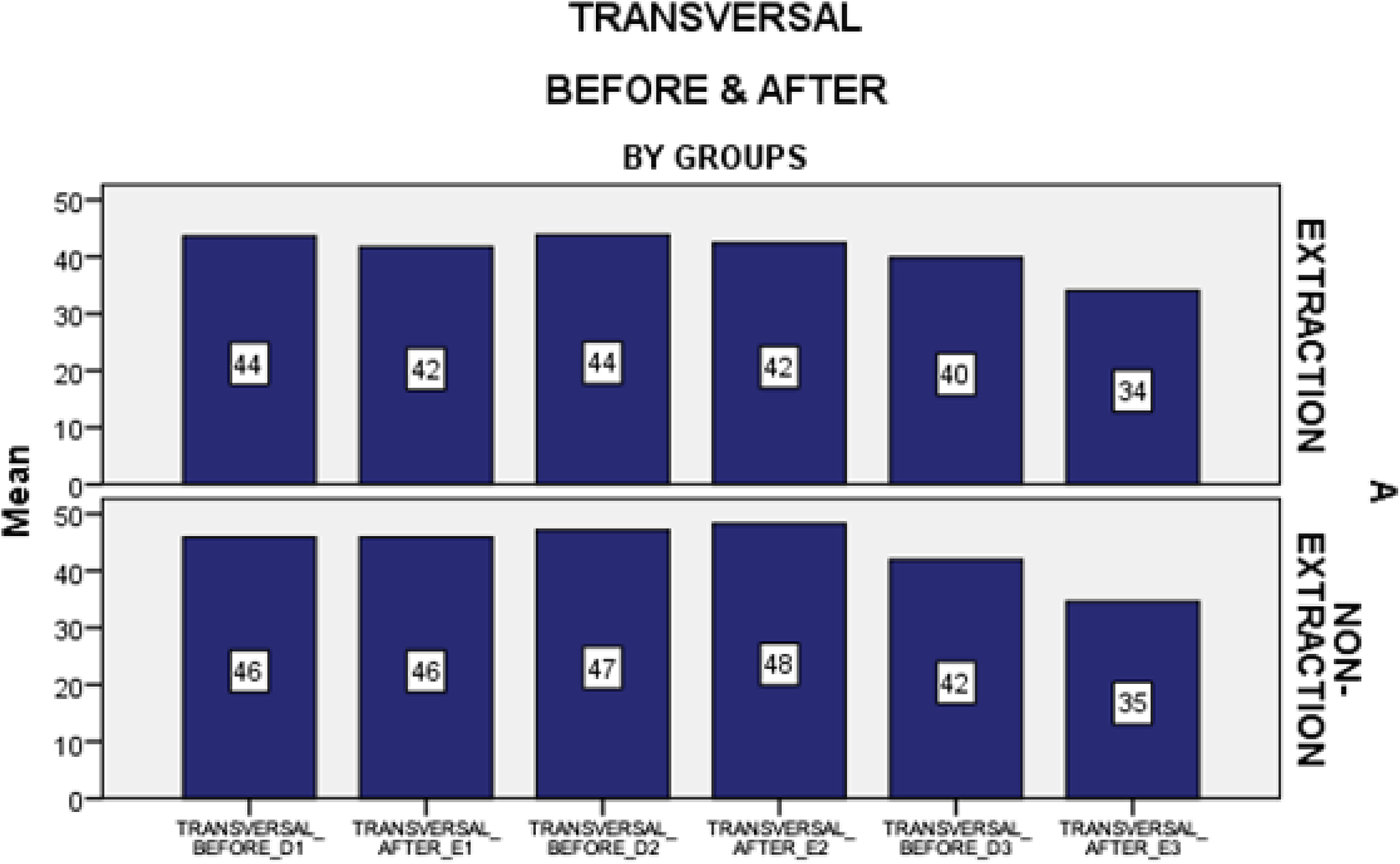
Transversal dimension before and after, in extraction and non-extraction treatments.

Molar angulation before and after, in extraction and non-extraction treatments.

Canine angulation before and after, in extraction and non-extraction treatments.
Transversal palatal form
To calculate the changes that occurred in the transversal palatal form during the treatment of extraction and non-extraction cases, four measurements were used (as shown in Figure 1): Distance between central groove of the maxillary right and left first molar. Distance between tip of the cusp of the second right and left premolar. Distance between tip of the cusp of the first right and left premolar. Distance between tip of the cusp of the right and left canine.
Measurements of crown angulation
In this study, the angulation of the maxillary right and left first molar and right and left canine in the buccolingual and mesiodistal direction was calculated. To calculate the buccolingual changes of angulation of the first molar and canines, two axes were adopted, and the angle between them was taken. The first axial was a line from the mesiobuccal cusp of the first molars to the medial buccal of the gingival border, and the same procedure was applied for the canines (buccal cusp of canine to the medial buccal of the gingival border).
The second axial was the line connecting three anatomical points: the first palatal ruga right, the first palatal ruga left, and the midway space between the first palatal ruga right and the first palatal ruga left. The angle between these two axes was taken to calculate the buccolingual angulation. To calculate the mesiodistal angulation changes of the first molars and canines, two axes were adopted, and the angle between them was taken. The first axial was a line from the mesiobuccal cusp of the first molars to the medial buccal of the gingival border, and the same procedure was applied for the canines (buccal cusp of canine to the medial buccal of the gingival border).
The second axial was the line connecting three anatomical points: the incisive papilla, the midway space between the first palatal ruga right and the first palatal ruga left, and the midway space between the second palatal ruga right and the second palatal ruga left. The angle between these two axes was taken to calculate the mesiodistal angulation.
Statistical analysis
The data obtained from this study were analyzed using IBM SPSS Statistics 22.0 (demo version) software. Since all the variables used in the study were quantitative (continuous) variables, they are presented as mean ± standard deviation (x ± ss). Due to the insufficient number of subjects (fewer than 50 subjects), the quantitative data were evaluated using the Shapiro–Wilk test. When comparing quantitative data between the groups, t-tests for independent samples were used. When the data did not comply with the regular distribution, the Mann–Whitney U test was used. Finally, when comparing quantitative data within the groups, t-tests for dependent samples were used. The level of error (α) was taken as 0.05, and p values (p ≤ 0.05) were considered statistically significant. All p values above this value (p > 0.05) were considered statistically insignificant.
Results
Evaluation of palatal form in the transversal and sagittal dimension before and after extraction in orthodontic cases
After the results had been collected and statistical operations conducted on them using the IBM SPSS Statistics 22.0 (demo version) program, the following results were obtained (Figure 4).
In order for the results to be comprehensible, the following symbols require explanation:
B1: Measurement of the distance between the incisive papilla and the midpoint of the right and left maxillary tuberosity (before extraction).
C1: Measurement of the distance between the incisive papilla and the midpoint of the right and left maxillary tuberosity (after extraction).
B2: Measurement of the distance between the right first molar lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C2: Measurement of the distance between the right first molar lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B3: Measurement of the distance between the right second premolar lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C3: Measurement of the distance between the right second premolar lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B4: Measurement of the distance between the right canine lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C4: Measurement of the distance between the right canine lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B5: Measurement of the distance between the right lateral lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C5: Measurement of the distance between the right lateral lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B6: Measurement of the distance between the left lateral lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C6: Measurement of the distance between the left lateral lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B7: Measurement of the distance between the left canine lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C7: Measurement of the distance between the left canine lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B8: Measurement of the distance between the left 2premolar lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C8: Measurement of the distance between the left 2premolar lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B9: Measurement of the distance between the left first molar lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C9: Measurement of the distance between the left first molar lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
D1: Distance between the central grove of the right and left maxillary first molar (before extraction).
E1: Distance between the central grove of the right and left maxillary first molar (after extraction).
D2: Distance between the tip of the cusp on the right and left second premolar (before extraction).
E2: Distance between the tip of the cusp on the right and left second premolar (after extraction).
D3: Distance between the tip of the cusp on the right and left canine (before extraction).
E3: Distance between the tip of the cusp on the right and left canine (after extraction).
From the results, it was noted that the sagittal dimension decreased in the extraction group after orthodontic treatment (Figure 2), especially in the following: The difference between sagittal before B1 and sagittal after C1 was statistically significant (p = 0.008). The difference between sagittal before B7 and sagittal after C7 was statistically significant (p = 0.0001). The difference between sagittal before B8 and sagittal after C8 was statistically significant (p = 0.0001). The difference between sagittal before B9 and sagittal after C9 was statistically significant (p = 0.0001). No other differences were significant (p > 0.05) (Table 1).
It was also noted that the transversal dimension decreased in the extraction group after orthodontic treatment (Figure 3), especially in the following: The difference between transversal before D1 and transversal after E1 was statistically significant (p = 0.001). The difference between transversal before D3 and transversal after E3 was statistically significant (p = 0.0001). No other differences were significant (p > 0.05) (Table 2).
Evaluation of palatal form in the transversal and sagittal dimensions before and after non-extraction in orthodontic cases
In order for the results to be comprehensible, the following symbols require explanation:
B1: Measurement of the distance between the incisive papilla and the midpoint of the right and left maxillary tuberosity (before extraction).
C1: Measurement of the distance between the incisive papilla and the midpoint of the right and left maxillary tuberosity (after extraction).
B2: Measurement of the distance between the right first molar lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C2: Measurement of the distance between the right first molar lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B3: Measurement of the distance between the right 2premolar lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C3: Measurement of the distance between the right 2premolar lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B4: Measurement of the distance between the right canine lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C4: Measurement of the distance between the right canine lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B5: Measurement of the distance between the right lateral lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C5: Measurement of the distance between the right lateral lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B6: Measurement of the distance between the left lateral lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C6: Measurement of the distance between the left lateral lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B7: Measurement of the distance between the left canine lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C7: Measurement of the distance between the left canine lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B8: Measurement of the distance between the left 2premolar lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C8: Measurement of the distance between the left 2premolar lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
B9: Measurement of the distance between the left first molar lingual border and the midpoint of the right and left maxillary tuberosity (before extraction).
C9: Measurement of the distance between the left first molar lingual border and the midpoint of the right and left maxillary tuberosity (after extraction).
D1: Distance between the central grove of the right and left maxillary first molar (before extraction).
E1: Distance between the central grove of the right and left maxillary first molar (after extraction).
D2: Distance between the tip of the cusp on the right and left second premolar (before extraction).
E2: Distance between the tip of the cusp on the right and left second premolar (after extraction).
D3: Distance between the tip of the cusp on the right and left canine (before extraction).
E3: Distance between the tip of the cusp on the right and left canine (after extraction).
As can be seen in the results, the sagittal dimension increased in the non-extraction group after orthodontic treatment, especially in b2c2–b4c4–b5c5, although it decreased in b1c1–b7c7–b8c8–b9c9. The difference between sagittal before B4 and sagittal after C4 was statistically significant (p = 0.0001). The difference between sagittal before B5 and sagittal after C5 was statistically significant (p = 0.003). The difference between sagittal before B7 and sagittal after C7 was statistically significant (p = 0.001). The difference between sagittal before B8 and sagittal after C8 was statistically significant (p = 0.0001). The difference between sagittal before B9 and sagittal after C9 was statistically significant (p = 0.0001). No other differences were significant (p > 0.05) (Table 3).
As can also be seen, the transversal dimension decreased in the non-extraction group after orthodontic treatment, especially in d1e1–d3e3, although it increased in d2e2. The difference between transversal before D3 and transversal after E3 was statistically significant (p = 0.0001) (Table 4).
Evaluation of upper first molar angulation before and after orthodontic treatment in extraction and non-extraction cases
After the results had been collected and the statistical operations conducted on them using IBM SPSS Statistics 22.0 (demo version) software, the following results were obtained (Figure 5).
In order for the results to be comprehensible, the following symbols require explanation:
F1: Mesiodistal angulation of the upper right first molar before extraction.
G1: Mesiodistal angulation of the upper right first molar after extraction.
F2: Mesiodistal angulation of the upper left first molar before extraction.
G2: Mesiodistal angulation of the upper left first molar after extraction.
F3: Buccolingual angulation of the upper right first molar before extraction.
G3: Buccolingual angulation of the upper right first molar after extraction.
F4: Buccolingual angulation of the upper left first molar before extraction.
G4: Buccolingual angulation of the upper left first molar after extraction.
The following can be seen from the results: The upper right first molar moved toward the distal direction in mesiodistal angulation in the extraction group. The upper left first molar moved toward the mesial direction in mesiodistal angulation in the extraction group. The upper right first molar moved toward the buccal direction in buccolingual angulation in the extraction group. The upper left first molar moved toward the lingual direction in buccolingual angulation in the extraction group (Table 5). The upper right first molar moved toward the distal direction in mesiodistal angulation in the non-extraction group. The upper left first molar moved toward the mesial direction in mesiodistal angulation in the non-extraction group. The upper right first molar moved toward the lingual direction in buccolingual angulation in the non-extraction group. The upper left first molar moved toward the lingual direction in buccolingual angulation in the non-extraction group (Table 6).
Evaluation of upper first canine angulation before and after orthodontic treatment in extraction and non-extraction cases
After the results had been collected and the statistical operations conducted on them using IBM SPSS Statistics 22.0 (demo version) software, the following results were obtained.
In order for the results to be comprehensible, the following symbols require explanation:
H1: Mesiodistal angulation of the upper right first canine before extraction.
I1: Mesiodistal angulation of the upper right first canine after extraction.
H2: Mesiodistal angulation of the upper left first canine before extraction.
I2: Mesiodistal angulation of the upper left first canine after extraction.
H3: Buccolingual angulation of the upper right first canine before extraction.
I3: Buccolingual angulation of the upper right first canine after extraction.
H4: Buccolingual angulation of the upper left first canine before extraction.
I4: Buccolingual angulation of the upper left first canine after extraction.
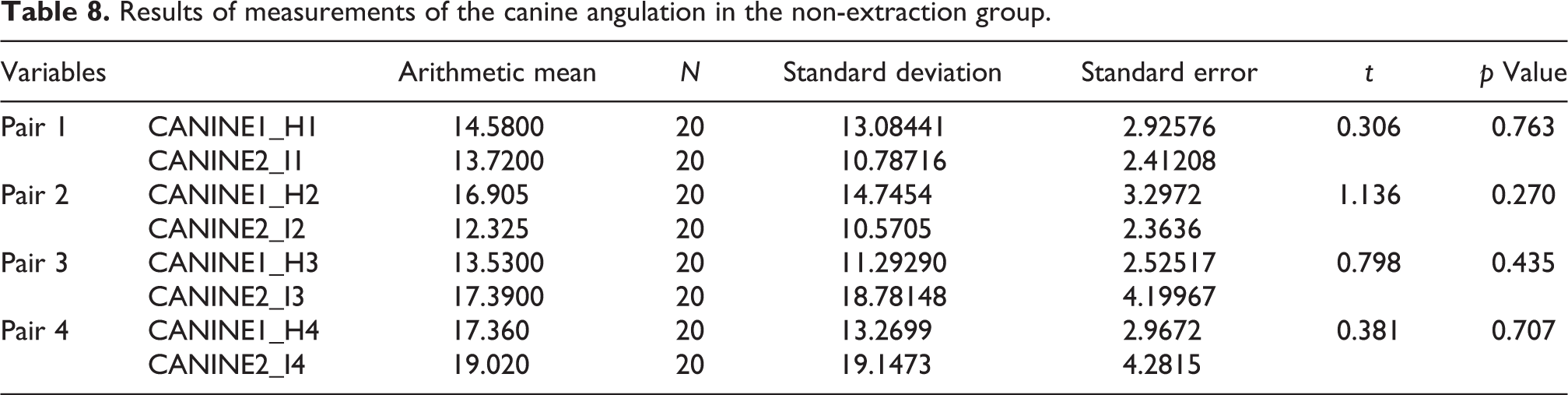
The following can be seen from the results: The upper right first canine moved toward the distal direction in mesiodistal angulation in the extraction group. The upper left first canine moved toward the distal direction in mesiodistal angulation in the extraction group. The upper right first canine moved toward the lingual direction in buccolingual angulation in the extraction group. The upper left first canine moved toward the lingual direction in buccolingual angulation in the extraction group (Table 7). The upper right first canine moved toward the mesial direction in mesiodistal angulation in the non-extraction group. The upper left first canine moved toward the mesial direction in mesiodistal angulation in the non-extraction group. The upper right first canine moved toward the buccal direction in buccolingual angulation in the non-extraction group. The upper left first canine moved toward the lingual direction in buccolingual angulation in the non-extraction group (Table 8).
Discussion and comparison of results
For dental clinicians, model analysis is considered an easy and simple technique. Compared to cephalometric analysis, model analysis has the advantage in measuring the crown angulation: Lateral cephalometric radiographs make it difficult to obtain such measurements due to the nature of superimposition on both sides. 15 In this study, all the patients were treated with an edgewise orthodontic appliance. Changes in the sagittal and transverse palatal forms were investigated. The patients who were treated with premolar extraction processes were compared accurately with the patients who were treated without premolar extraction processes. After the obtained results had been reviewed, it was concluded that there were several changes in the upper jaw after the orthodontic treatment, whether with or without the extraction of teeth. This indicates that orthodontic treatment in general induces many positive or negative changes in the teeth and jaws. In group B patients, who received orthodontic treatments with the extraction of their upper first premolars, a decrement in sagittal palatal form and transversal dimensions was noticed, and it was statistically significant (p ≤ 0.05). Such changes result from the retraction of the anterior teeth to fill the remaining space created by the extraction; they could also be attributable to the changes in the posture of the tongue, which is forced to be elevated more in an upward direction to accommodate the lost space anteriorly. In group A patients, who received orthodontic treatments without tooth extraction, it was observed that changes in the transverse direction increased in the premolar region, although this was statistically insignificant, and decreased in the molar region, which could be due to the nature of the archwires that were used in the treatment to constrict the arch form. The sagittal palatal form also decreased in the molar teeth and increased in the premolar region as a result of the changes in the arch form, correcting the articulation of the teeth, removing spaces between the teeth, and allowing the teeth to settle into their ideal locations; these were statistically significant changes within the non-extraction group. According to these findings, however, changes in the palatal height and volume are affected by the timing, duration, and the individual’s age, as growth has a huge impact on palatal height and volume. These results indicate that palatal volume might have decreased in the extraction group, as space loss has occurred anteriorly due to closure of the extraction space. Since growth can still affect palatal height and volume, this might become less significant. This can also be seen in a study that measured palatal volume and height in growing patients who received orthodontic treatment by either extraction or non-extraction: The palatal volume increased in the non-extraction group; meanwhile, a decrease in palatal volume was noticed in the extraction group, although this was followed by a slight increase due to growth factors. 16
The anterior tongue functioning space is theoretically decreased with retraction of the maxillary incisors. This leads to the assumption that reduced anterior space will create more pressure of tongue for the sagittal palatal form. It also explains why patients treated with a premolar extraction process exhibit the same relapse tendency in arch width as patients treated without a premolar extraction process. Moreover, there were no statistically significant changes in the non-extraction group related to the angulation of molars, and the canine results showed upper right molar crown angulation. Although distal tipping in the upper dental arch was clinically observed, it was not statistically significant and was caused by good alignment of the teeth and removal of the crowding so that the teeth can return to their normal positions. Molar left crown angulation decreased in the non-extraction group, indicating mesial tipping in the upper dental arch, but this was insignificant. The change in angulation of the right and left molars in the buccolingual direction decreased significantly in the non-extraction group, indicating lingual tipping in the upper dental arch; this explains the decrement in transversal palatal form. The change in right and left canine angulation decreased significantly in the non-extraction group, indicating mesial tipping in the upper dental arch, caused by good alignment of teeth and removal of the crowding. The change in angulation of the right canine in the buccolingual direction increased, indicating buccal tipping; meanwhile, the change in angulation of the left canine in the buccolingual direction decreased, indicating lingual tipping.
In group A patients, who were treated with the extraction of teeth, the results indicated that the angulation of upper molars occurred in the mesial direction in the left molar, due to the extraction of premolars, and moved mesially toward the point of closing the space of extraction. Distal tipping of the left and right canines, due to the extraction of premolars, and movement distally toward the point of closure of the space of extraction were also observed.
The change in angulation of the right molars in the buccolingual direction increased, indicating buccal tipping; meanwhile, the change in angulation of the left molars in the buccolingual direction decreased, indicating lingual tipping.
The change in angulation of the right and left canines in the buccolingual direction decreased significantly in the extraction group, indicating lingual tipping in the upper dental arch; this explains the decrease in transversal palatal form.
Conclusion
This study investigated the transverse and sagittal changes in the palatal form and angular changes in the molars and canines in patients treated with and without premolar extractions. The results were as follows: (1) In the extraction group, the sagittal and transverse palatal form decreased in the molar region. (2) In the non-extraction group, the sagittal and transverse palatal form increased sagittally in the premolar region; meanwhile, a decrement in the molar region was observed. (3) In the non-extraction group, a decrement in the transverse palatal form was observed. (4) Angular changes in the non-extraction group were not significant, while canine angulation in the extraction group indicated a distal and lingual tipping after retraction. (5) At the same time, molar angulation in the extraction group indicated distal crown tipping.
Results of measurements of the sagittal dimension in the extraction group.
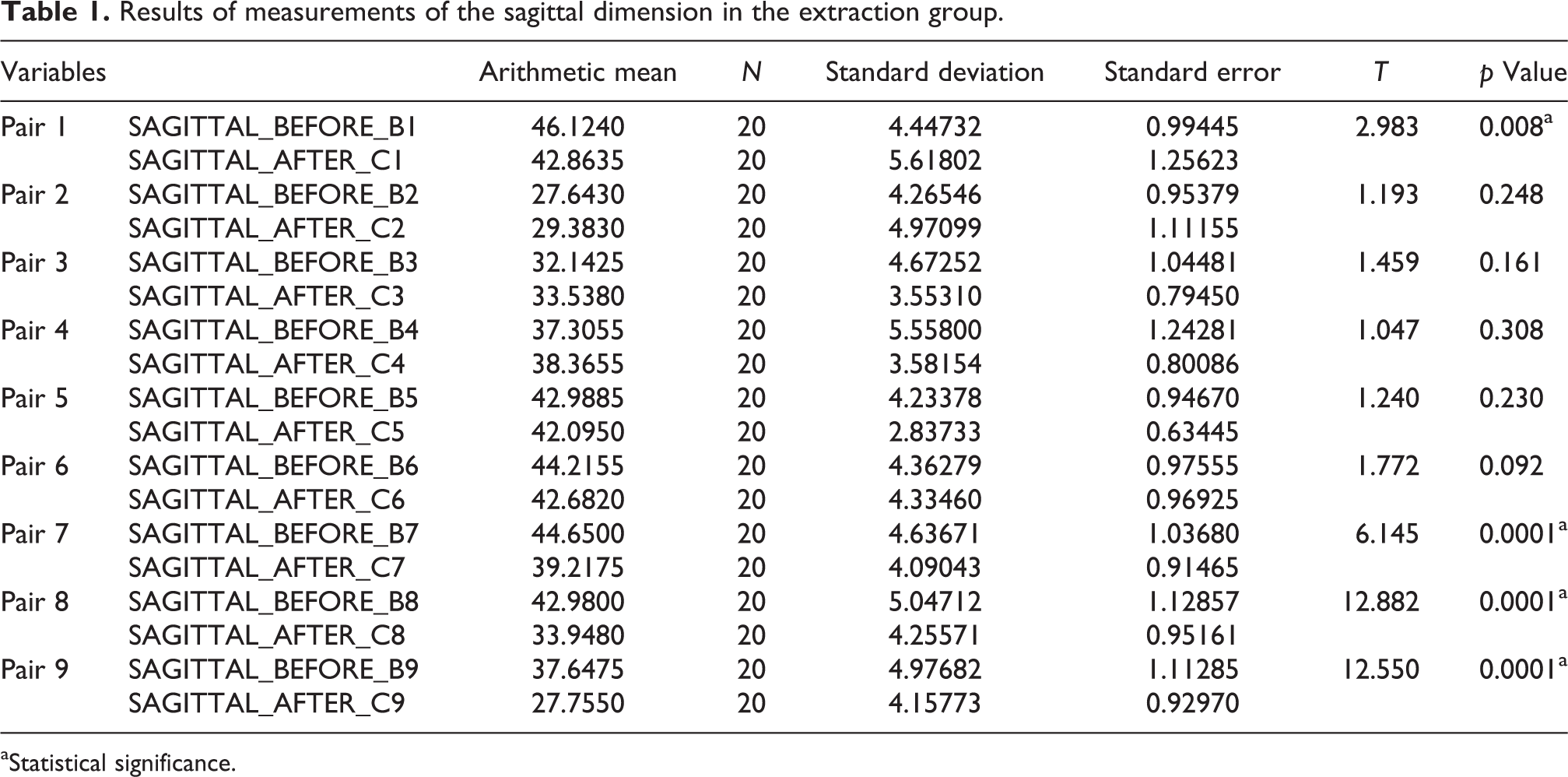
aStatistical significance.
Results of measurements of the transversal dimension in the extraction group.

aStatistical significance.
Results of measurements of the sagittal dimension in the non-extraction group.

aStatistical significance.
Results of measurements of the transversal dimension in the non-extraction group.
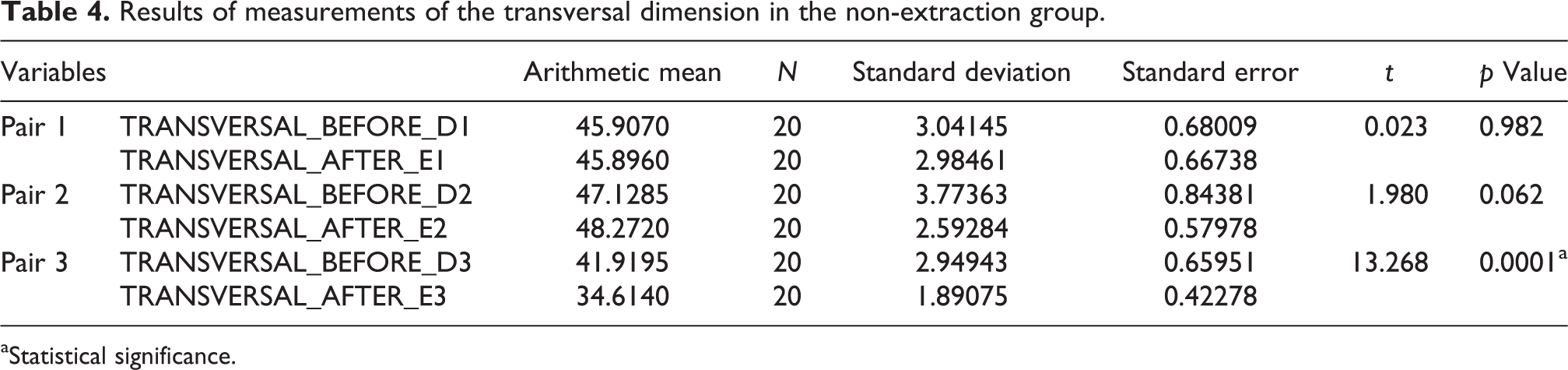
aStatistical significance.
Results of measurements of the molar angulation in the extraction group.

aStatistical significance.
Results of measurements of the molar angulation in the non-extraction group.

Results of measurements of the canine angulation in the extraction group.
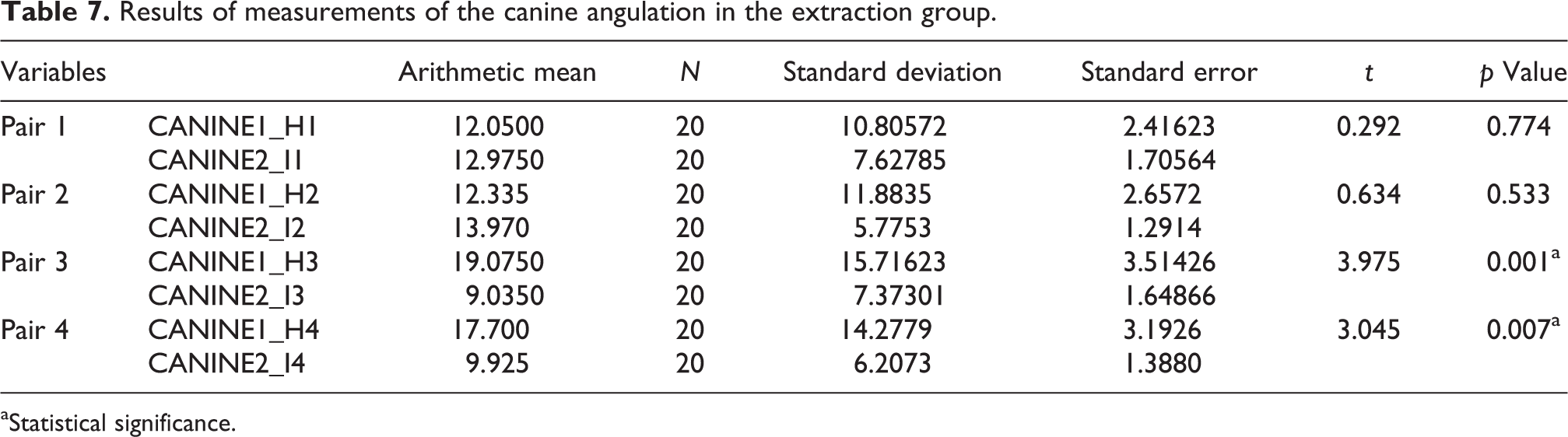
aStatistical significance.
Results of measurements of the canine angulation in the non-extraction group.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.