
Abstract
Objective:
This study aims to determine sex differences in poststroke hypertriglyceridemia (serum triglyceride levels ⩾ 200 mg/dl) and high stroke severity in ischemic stroke patients.
Method:
Our study analyzed data from 392 males and 373 females with hypertriglyceridemia. Stroke severity on admission was measured using the National Institute of Health Stroke Scale (NIHSS) with a value ⩽7 indicating a more favorable post-stroke prognosis while a score of >7 indicates poorer post-stroke outcomes. Logistic regression models adjusted for demographic and risk factors. The adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for each clinical risk factor were used to predict the increasing odds of an association of a specific clinical baseline risk factor with the male or female AIS with hypertriglyceridemia.
Results:
In the adjusted analysis, male patients with hypertriglyceridemia, diastolic blood pressure (OR = 1.100, 95% CI, 1.034-1.171, P = .002), and Ischemic stroke mortality (OR = 6.474, 95% CI, 3.262-12.847, P < .001) were significantly associated with increased stroke severity. In female patients with hypertriglyceridemia, age (OR = 0.920, 95% CI, 0.866-0.978, P = .008) was associated with reduced stroke severity, while ischemic stroke mortality score (OR = 37.477, 95% CI, 9.636-145.756, P < .001) was associated with increased stroke severity.
Conclusion
Increased ischemic stroke mortality risk score was associated with increased severity in both male and female AIS patients with hypertriglyceridemia. Our findings provide information about sex differences in specific risk factors that can be managed to improve the care of male and female ischemic stroke patients with hypertriglyceridemia.
Introduction
Hypertriglyceridemia which is characterized by abnormally high plasma TG levels is caused by defective triglyceride (TG) metabolism. 1 The National Cholesterol Education Program guidelines 2 stratify the concentrations of fasting TGs into 4 levels: TGs levels of <150 mg/dl as normal, 150 to 199 mg/dl mild, 200 to 499 mg/dl as high, and levels of ⩾500 mg/dl as very high. 3 Elevated triglyceride levels (200-499 mg/dl)or hypertriglyceridemia often results from a blend of acquired factors, including being overweight, physical inactivity, smoking, excessive alcohol consumption, and a high intake of carbohydrates, coupled with genetic influences.4,5
Several studies have investigated the relationship between hypertriglyceridemia and acute ischemic stroke (AIS).8 -11 Findings indicate that serum triglyceride level is an important predictor of early prognosis in patients with AIS. 6 In a study using a random-effects model, there was a significant association between hypertriglyceridemia and an increased risk of small-vessel occlusion, a subtype of ischemic stroke. 7 The initial neurological severity was less severe in patients with hypertriglyceridemic waist phenotype. 8 In a prospective study, hypertriglyceridemia was associated with an increased risk of ischemic stroke in both males and females, particularly among female AIS patients. 9 High triglycerides seem to exert a worse effect on females than males regarding the risk of ischemic stroke. 5 However, the relationship between hypertriglyceridemia, stroke severity, and specific risk factors in male and female ischemic stroke patients is not fully understood.
Studies have shown that ischemic stroke patients, especially females, generally experience poor functional outcomes compared to males. 10 However, when treated with an intravenous tissue-type plasminogen activator (IVtPA) no significant difference in outcomes was reported. 11 Conversely, males tend to present with improved outcomes with IVtPA treatment than females. 12 Such sex differences in stroke outcomes have been attributed to several factors such as age, 13 comorbidities,14,15 pre-stroke functional status,16,17 and stroke severity. 15 While several studies have shown that females have increased severity of stroke compared to males 18 further investigation is needed to determine whether the observed sex differences are observable in ischemic stroke patients with hypertriglyceridemia and varying levels of stroke severity.
The importance of using a stroke severity measure such as the National Institutes of Health Stroke Scale (NIHSS) in statistical models for outcome prediction has been established.19,20 Initially, NIHSS was designed for research purposes to evaluate baseline data from patients in acute stroke clinical trials, it is now widely used in clinical settings to evaluate stroke severity, determine appropriate treatment, and predict patient outcomes. 21 Stratified NIHSS scores offer valuable insights into the severity of stroke and the patient’s neurological status after an AIS.17,22 Values of NIHSS scores >7 at 6 hours from stroke onset produced a positive predictive value of more than 75% for a worse neurologic function, 23 and a score of ⩽7 was associated with better functional neurological outcomes.24,25 Findings indicate that stratified NIHSS scores provide measures of the severity of stroke and the neurologic status of the patient.20,26
While hypertriglyceridemia may heighten the risk and severity of ischemic stroke by promoting atherosclerosis and thrombosis and increasing blood viscosity, it may exert some protective effects in post-stroke patients via unclear mechanisms. 5 Given this discrepancy in the role of hypertriglyceridemia among AIS patients, it is plausible that other factors may influence stroke severity in both male and female AIS populations with hypertriglyceridemia. This raises the possibility that even if elevated TG or hypertriglyceridemia is controlled in AIS patients, stroke severity could still manifest in male and female patients due to other clinical risk factors. Therefore, specific baseline clinical determinants may differentially contribute to sex differences in stroke severity in AIS patients with hypertriglyceridemia. We tested this hypothesis by identifying specific demographic and clinical determinants that could contribute to sex differences in AIS patients with fasting elevated triglycerides. This study aims to investigate sex differences in stroke severity in a population of patients with hypertriglyceridemia, defined by a serum triglyceride level of 200mg/dL and above. Findings from this study could inform clinical decision-making and treatment strategies targeted at factors contributing to sex differences and stroke severity in stroke patients with hypertriglyceridemia.
Materials and Methods
Study population
This retrospective study analyzed information from patients diagnosed with acute ischemic stroke (AIS) and hypertriglyceridemia at a regional stroke center of Prisma Health between January 2010 and January 2016. Data included in this study are from patients admitted to the stroke unit, diagnosed clinically, and confirmed by brain imaging based on World Health Organization (WHO) criteria for diagnosis of stroke were included. 27 Stroke severity on admission was measured using the National Institute of Health Stroke Scale (NIHSS). A score of ⩽7 on this scale indicated a more favorable post-stroke prognosis while a score of >7 indicated a less favorable post-stroke outcome. Patients with hemorrhagic stroke were not included in this study. Criteria for inclusion in this study include AIS in addition to hypertriglyceridemia, measured by a triglyceride level greater than or equal to 200 mg/dl. 28 The study also collected additional data to identify stroke risk factors including demographics such as age, race, sex, and medical history including atrial fibrillation/atrial flutter, coronary artery disease, carotid stenosis, diabetes mellitus, dyslipidemia, heart failure, hypertension, obesity, BMI, previous stroke or TIA, family history of stroke, and peripheral vascular disease. Information on medications taken before admission was documented including the use of antiplatelets, anticoagulants, antihypertensives, cholesterol-reducers, diabetic medications, or no medications. We collected data on the use of IV Tissue Plasminogen Activator (IVTPA) categorized by whether it was initiated in the hospital, outside the hospital, or antithrombic initiation by the end of the hospital stay. Data on ambulatory status before stroke, during admission, and discharge were also extracted and recorded as the ability to ambulate independently, with assistance, or unable to ambulate. Patients without available ambulatory data were labeled as either “No Data (ND)” or “Missing.” Laboratory values and vital signs on admission were recorded including cholesterol (HDL, LDL, lipids), serum glucose, creatinine, INR, heart rate, and blood pressure. Data on the overall ischemic stroke mortality rate was also extracted. Our study was approved by the PRISMA Health institutional review board of the Institutional Committee for Ethics. The study ensured complete anonymity of individual patients, and specific informed consent from patients was not obtained due to this anonymity. The investigators who performed the data analyses were unaware of the identities of those involved. This information was only available to the coordinating center of the PRISMA Health Upstate stroke register.
Statistical data analysis
The student-t-test was utilized to evaluate differences in continuous variables while the Pearson Chi-square test was used to assess differences in proportions. We verified the normal distribution of our data using the Kolomogorov-Smirnov test and this was further validated using a Lilliefors test for enhanced precision. The statistical significance level was set at a P value of <.05. To further stratify male and female hypertriglyceridemia groups into patients with NIHSS ⩽ 7 or NIHSS > 7, a univariate analysis was conducted. Subsequently, binary logistic regional models were constructed using identified predictors from the univariate analysis with a probability value of <.3, which allowed for the identification of independent predictors of NIHSS scores for male and female AIS patients with hypertriglyceridemia. This approach reduced discrepancies from non-comparable parameters. Binary logistic regional models were used to compute odds ratios (ORs) and corresponding 95% confidence intervals (CIs) to evaluate the significance of each variable by predicting the probability of being associated with male or female AIS patients with hypertriglyceridemia.
For the analysis, each AIS patient with hypertriglyceridemia irrespective of sex, was compared to determine the association with increased or reduced stroke severity based on baseline characteristics and risk factors. In the multivariate analyses, we assessed the influence of demographic and clinical risk factors or comorbidities, and stroke severity on sex differences among AIS with hypertriglyceridemia. Potential interactions between risk factors, as well as stroke severity, were controlled by adding interaction terms to the regression model.
We used the backward selection method because it allowed for simultaneous consideration of all variables. This method retained all variables in each regression model by an automatic procedure particularly when risk factors interacted with one another, to control for multicollinearity. Moreover, it facilitated determining the level of importance of each predictor variable by evaluating the effects once other predictor variables were statistically eliminated.
In the binary regression model, the dependent variable was stroke severity, stratified by an NIHSS score of ⩽ or >7, while the independent variables comprised the demographic and clinical risk factors. We analyzed, (i) male and female AIS-hypertriglyceridemia groups, (ii) male AIS- AIS-hypertriglyceridemia group, and (iii) female AIS-hypertriglyceridemia groups were analyzed separately. Odds ratios and 95% confidence intervals were calculated with a P-value significance of P < .05 to predict variables associated with higher or lower stroke severity and thus, more, or less favorable post-stroke outcomes.
To assess the fitness of the logistic regression model and ensure the absence of collinearity and adequate sampling, we utilized the Hosmer-Lemeshow goodness-of-fit statistic and odds ratios (ORs). The outcome measures of odds ratios and 95% confidence intervals (95% CIs) were determined for each model by considering a significance level of P < .05. The sensitivity, and accuracy of the logistic regression models were determined by the overall correct classification percentage and area under the Receiver Operating Curve (ROC). All statistical analyses were performed with Statistical Package for Social Sciences version 29.0 for Windows (SPSS, Chicago, IL).
Results
A total of 765 patients with acute ischemic stroke (AIS) with elevated triglyceride levels ⩾200 were identified (Table 1). Of this, 392 were males while 373 were females. In comparison to females, male patients were more likely to be younger, and present with coronary artery disease (CAD) or a history of myocardial infarction. They were less likely to present with hypertension and more likely to independently ambulate before admission. Males presented with higher total cholesterol, diastolic blood pressure, and lower HDL and LDL when compared to females. Additionally, males were less likely to independently ambulate after discharge.
Clinical characteristics of male and female acute ischemic stroke patients with triglyceride level ⩾ 200.

Pearson chi-square test.
T-Test.
P-value < .05.
Table 2 presents the clinical and demographic characteristics associated with stroke severity for male and female patients stratified by NIHSS scores. Males AIS patients with elevated triglyceride levels ⩾ 200 and NIHSS > 7 were less likely to have a family history of stroke or heart failure and less likely to ambulate Independently on admission, and before stroke. They were also less likely to receive IVTPA at the hospital and antithrombic therapy by the end of the hospital stay. Males were more likely to present with a history of elevated heart rate, a higher estimated mortality rate for ischemic stroke, and were less likely to ambulate Independently. On the other hand, females with AIS and elevated triglyceride levels ⩾ 200 and NIHSS > 7 were more likely to present with atrial fibrillation or ambulate independently on admission, or before stroke. They were also less likely to receive IVTPA initiated at the hospital, and antithrombic therapy by the end of hospital stay. They were more likely to present with elevated blood glucose levels, and an increased heart rate as well as a higher estimated mortality rate for ischemic stroke. Similar to males, females were less likely to ambulate on their own after discharge.
Clinical characteristics of male and female acute ischemic stroke patients with Triglyceride level ⩾ 200 stratified by NIHSS > 7 or NIHSS ⩽ 7.

Pearson chi-square test.
T-Test.
P-value < .05.
For the adjusted analysis of the entire AIS population with elevated triglycerides or hypertriglyceridemia( Figure 1), CAD (2.473, 95% CI, 1.592-3.841, P < .001) and diastolic blood pressure (OR = 1.031, 95% CI, 1.019-1.043, P < .001) were associated with males, while age (OR = 0.976, 95% CI, 0.960-0.992, P = .003), inability to ambulate independently before stroke (OR = 0.58, 95% CI, 0.007-0.476, P = .008), rtPA received outside the hospital (OR = 0.501, 95% CI, 0.253-0.993, P = .048), HDL (OR = 0.949, 95% CI, 0.930-0.969, P = .048), /BMI (OR = 0.971, 95% CI, 0.943-1.000, P = .047), and increased heart rate (OR = 0.980, 95% CI, 0.968-0.993, P = .002) were associated with females. The logistic regression model demonstrated strong predictive power. The AUROC is 0.771 (95% CI, 0.687-0.913, P < .001).
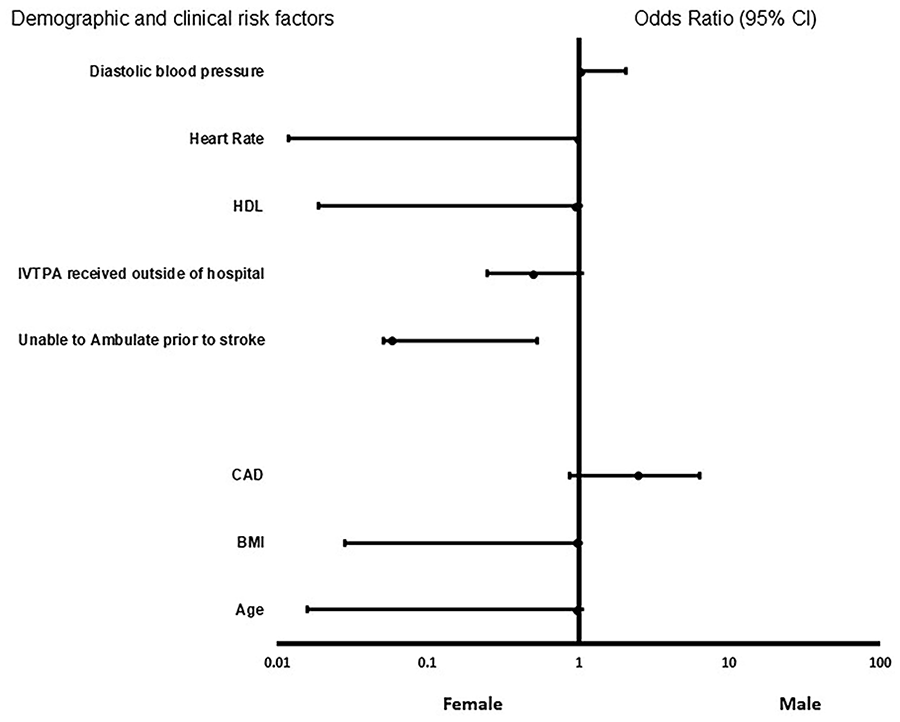
Forest plot representation of clinical and demographic factors for male or female ischemic stroke patients in the whole stroke population with elevated triglyceride levels ⩾ 200 mg/dl. Odd ratio below 1 denotes factors that are associated with females while odd ratio above 1 denotes factors that are associated with males. *Indicates statistical significance (P < .05) with a 95% confidence interval.
For the adjusted analysis for male ischemic stroke patients with a triglyceride level above 200 mg/dl and NIHSS ⩽7 or NIHSS > 7( Figure 2), systolic blood pressure (OR = 0.943, 95% CI, 0.908-0.978, P = .002), was associated with reduced stroke severity, while diastolic blood pressure (OR = 1.100, 95% CI,1.034-1.171, P = .002), and ischemic stroke mortality (OR = 6.474, 95% CI,3.262-12.847, P < .001) were associated with stroke severity. The model demonstrated a strong predictive power, and the AUROC is 0.752 (95% CI, 0.678-0.845, P < .001). For female patients (Figure 3), age (OR = 0.920, 95% CI, 0.866-0.978, P = .008), was associated with reduced stroke severity, IVtPA initiated in the hospital (OR = 4.541, 95% CI, 0.893-23.091, P = .06), and increased ischemic stroke mortality risk score (OR = 37.477, 95% CI, 9.636-14.756, P < .001), were associated with increased severity. The regression model was strong and the AUROC is 0.760 (95% CI, 0.701-0.8021, P < .001).

Forest plot representation of clinical and demographic factors for male ischemic stroke patients with elevated triglyceride level ⩾ 200 mg/dl. Odd ratio below 1 denotes factors that are associated with a NIHSS score ⩽ 7 while odd ratio above 1 denotes factors that are associated with a NIHSS score > 7. *Indicates statistical significance (P < .05) with a 95% confidence interval.

Forest Plot representation of clinical and demographic factors for female ischemic stroke patients with elevated triglyceride level ⩾ 200 mg/dl Odd ratio below 1 denotes factors that are associated with an NIHSS score ⩽ 7 while an odd ratio above 1 denotes factors that are associated with a NIHSS score > 7. *Indicates statistical significance (P < .05) with a 95% confidence interval.
Discussion
While hypertriglyceridemia has been reported to be associated with an increased risk of ischemic stroke in both male and female patients, 9 the relationship between hypertriglyceridemia, stroke severity, and specific risk factors that contribute to sex differences in ischemic stroke is not very clear. We investigated this issue in the current study. In the entire stroke population with hypertriglyceridemia, irrespective of stroke severity, CAD and diastolic blood pressure were associated with males, while age, inability to ambulate independently before the onset of stroke, BMI, IVTPA treatment outside the hospital, HDL, and elevated heart rate were associated with females. In the male ischemic stroke patients with hypertriglyceridemia, systolic blood pressure was associated with reduced stroke severity, while diastolic blood pressure and ischemic stroke were associated with increased stroke severity. For females, age was associated with reduced stroke severity, while increased ischemic stroke mortality risk score was associated with increased severity. The effect of diastolic blood pressure was significant and higher in males when compared with females, but when stratified by stroke severity, diastolic blood pressure was not significantly different in male and female patients with increased or reduced stroke severity in the univariate analysis.
In the adjusted analysis for the whole stroke population, diastolic blood pressure was associated with male patients, and this effect was sustained for male AIS with hypertriglyceridemia as well as with increased stroke severity. On the other hand, systolic blood pressure was associated with reduced stroke severity in male patients. High blood pressure also known as hypertension is categorized into 2 levels according to the American Heart Association guidelines, the first level is elevated blood pressure (BP), characterized by systolic pressure (SBP) ranging from 120 to 29 mm Hg and diastolic pressure (DBP) below 80 mm Hg, The second level involves an SBP of 130 to 139 mm Hg and a DBP of 80 to 89 mm Hg. 29 When diagnosed, over 3-quarters of patients with AIS present with elevated BP. 20 Among this group, half already have a history of hypertension. Several studies strongly associate a DBP exceeding 80 mm Hg with hypertension. 30 While clinical studies revealed a connection between hypertension and an increased risk of AIS, the link between BP upon admission for AIS and the severity of the stroke remains a topic of debate.31,32 More importantly, in the context of this study, there are limited and conflicting data on whether SBP or DBP at admission is a more accurate predictor of stroke severity. While some studies have shown that neither SBP nor DBP predicted stroke severity, 33 others suggest that onlySBP 34 or DBP35,36 was associated with worse neurologic outcomes. Our current study indicates that among male AIS patients with hypertriglyceridemia, higher diastolic blood pressure was associated with increased stroke severity, whereas higher systolic blood pressure was associated with reduced stroke severity. In our study, the systolic BP for males with increased stroke severity was 152.58 ± 27.640 while the diastolic BP associated with reduced stroke severity was 86.25 ± 16.462. We did not separately analyze risk factors contributing to stroke severity in AIS patients with elevated systolic 86.25 ± 16.462 mm Hg and those with elevated DBP 152.58 ± 27.640 mm Hg. Although the independent effect of SYS and DBP on stroke severity can be estimated by adjusting for differences in comorbid conditions, 37 it is challenging to reliably adjust for variations in stroke severities due to the effect of SYS or DBP mainly because the severity associated with individual risk factors is difficult to be analyzed quantitatively. Moreover, it is difficult to adequately control the severity of stroke associated with the specific effect of each risk factor. Therefore, our results do not align with the possibility that elevated systolic blood pressure as a risk factor results in less severe outcomes than elevated DBP in AIS patients with hypertriglyceridemia. 38 Consequently, future studies should investigate the relationship between diastolic and systolic BPs in the acute phase of stroke as well as its association with stroke severity and related sex differences. Additionally, these studies should clarify how elevated DBP or systolic either alone or in combination with other risk factors such as hypertriglyceridemia are associated with higher stroke severity in male AIS patients with hypertriglyceridemia.
We observed that in female AIS patients with hypertriglyceridemia, age was associated with reduced stroke severity. Many studies have investigated stroke severity in females. For example, the International Stroke Trial study found higher case fatality rates for females at 14 days and 6 months following a stroke. However, when accounting for variations in age and comorbidities between the sexes, the higher fatality in females was negated at 6 months post-stroke. 39 Baseline disparities in age, comorbidities, severity, and pre-stroke disability in male and female patients have been identified as significant contributors to the increased mortality observed in females. 40 Nevertheless, even with these factors considered, females consistently show poorer functional outcomes after stroke. 41 Throughout most of the life span, males tend to have a higher incidence of stroke than females. However, beyond the age of 85 years, the incidence of stroke is higher among females. In our current study, we observed that female AIS patients with an average age of 62.48 ± 13.743 and higher HDL of 38.15 ± 10.109 compared with females with hypertriglyceridemia were more likely to present with reduced stroke severity. High-density lipoproteins (HDL) are a type of lipoproteins that carry cholesterol in the blood, and females tend to present with a higher HDL level than males. 42 While some studies have reported that some lipid levels may not be stable after stroke, high-density lipoprotein levels are more stable after stroke than total cholesterol levels 43 and have a protective effect for ischemic stroke among elderly patients. 43 Our data reveal that hypertriglyceridemic female AIS patients of the average age of 62 years with higher HDL were associated with reduced stroke severity. Therefore, increased HDL-C levels may contribute to reduced stroke severity among hypertriglyceridemic female AIS patients in our current study. Our data add to the evidence relating age, HDL, and hypertriglyceridemia to stroke and support HDL as an important modifiable stroke risk factor for future studies on sex differences in stroke severity.
Female patients with IVTPA initiated at the hospital were more likely to be associated with increased stroke severity. IVTPA is a proven intervention for acute ischemic stroke patients, with an evidence-based recommendation from the American Heart Association/American Stroke Association (AHA/ASA).44,45 The benefit of IVTPA in acute ischemic stroke is strongly time-dependent. The more aggressive use of IVtPA in patients with relative contraindications, who were severely symptomatic (NIHSS > 10), with IVtPA, has been investigated. 46 The value of IVtPA in such severely symptomatic patients with large vessel occlusion reveals good outcomes.47 -49 Findings indicate that the efficacy of IVtPA treatment in patients with severe symptoms depends on the presence of a major anterior circulation artery occlusion that is detectable by CTA. 47 It is possible that our female patients with severe stroke were treated with IVtPA due to major anterior circulation occlusions. Our finding is supported by other studies that in patients presenting with severe stroke symptoms caused by major anterior circulation artery occlusions, IVtPA improves outcomes.47,50
We observed that ischemic stroke mortality was associated with increased stroke severity in both male and female patients with hypertriglyceridemia. Several risk factors are known to increase mid and long-term mortality of ischemic stroke patients. For example, age, pre-stroke functional status (mRS score > 0), stroke severity (NIHSS), diabetes mellitus, prior heart disease, posterior circulation stroke syndrome (compared with anterior circulation stroke syndromes), and nonlacunar stroke have all been reported to contribute to increased ischemic stroke mortality. Furthermore, there are variations in mortality prediction factors between males and females. 51 For example, a systematic review of 98 studies revealed that stroke severity and mortality were higher in females compared to males. 52 Our finding is supported by another study, 53 that identified stroke severity (measured by the NIH scores) as the primary independent factor linked to in-hospital mortality among ischemic stroke patients. Our data also add to the evidence that hypertriglyceridemia which contributes to AIS risk and higher stroke severity could contribute to sex differences in ischemic stroke mortality.
Conclusion
A significant number of studies have investigated the relationship between hypertriglyceridemia and ischemic stroke.5,54,55 Findings reveal an increased risk of ischemic stroke in both male and female patients. In this study, we investigated the role of hypertriglyceridemia as an important risk factor in stroke severity that could contribute to understanding sex differences in ischemic stroke with varying levels of stroke severity. In our results, we found that, among male AIS with hypertriglyceridemia, diastolic blood pressure was associated with increased stroke severity, whereas systolic blood pressure was associated with reduced stroke severity. In addition, age was associated with reduced stroke severity in female patients. Ischemic stroke mortality risk score was associated with severity in both male and female AIS patients with hypertriglyceridemia. These findings reveal sex differences and suggest the need to develop management strategies targeting male and female AIS patients with increased severity to enhance their eligibility for rtPA therapy. Further prospective research is needed to evaluate the specific role that TGs play in stroke severity and sex differences in patients with stroke, which may be important for clinical care and secondary prevention of stroke.
Limitations
This study has strengths as well as multiple limitations. We used data from a hospital-based stroke database and the use of multivariate statistical analyses provided important results. Hence, a major strength of our study is the utilization of prospectively collected data in a large stroke center from consecutively admitted ischemic stroke patients that closely resemble real-world clinical practices within a controlled stroke unit system. This unit was led by experienced stroke neurologists, and this improves the consistency of clinical evaluations and promotes sample homogeneity among acute ischemic stroke patients. Nevertheless, the results of our study may not be broadly applicable to the general population of ischemic stroke patients given our focus only on patients who were admitted to a dedicated acute stroke unit, patients with notably poor clinical baseline status or multimorbidity might have been previously admitted to a general or palliative care ward rendering our findings less generalized. The stroke unit setting allows a rapid and comprehensive stroke work-up and makes the variables used easily available, which may not be the case in other settings. On the other hand, stroke unit treatment is regarded as the gold standard of acute stroke care and has been consistently associated with lower mortality rates, irrespective of the patient’s age or clinical characteristics.56,57 In this context, our study has additional value given that access to organized stroke unit care will hopefully become more widely available shortly. Likewise analyzed patients cannot be considered as fully representative of stroke patients overall but constitute those patients that were felt to still benefit from stroke unit treatment.
In this study, we used fasting triglycerides levels which may be a more sensitive screening tool than non-fasting triglycerides for detecting disease risk or severity Combing with data from non-fasting triglycerides in future studies will provide a comparative analysis and a strong predictor of severity comparable to fasting triglycerides and possible sex differences. Moreover, we do not have data on disease status or treatment status for hypertriglyceridemia and this is an important limitation. However, despite this limitation, this study shows a sex-related difference in specific risk factors that can be managed to improve eligibility for thrombolytic therapy in ischemic stroke patients with hypertriglyceridemia. This highlights sex disparities and possible lower-intensity hypertriglyceridemia management among female patients. Greater mortality in male patients has been reported 36 and this study points to similarities among males and females in increased stroke mortality for AIS patients with hypertriglyceridemia.
Footnotes
Acknowledgements
We thank the stroke unit for helping in the data collection.
Abbreviations
Adjusted OR-: Adjusted odd ratio; atrial fibrillation: A fib, HRT: Hormone Therapy; BMI: Body mass index; CHF: Congestive heart failure; CI: Confidence interval; IRB: Institutional Review Board. INR: International normalized ratio; LDL-C: Low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; rtPA: Recombinant tissue plasminogen; TC: Total cholesterol; TG: Triglyceride, AIS: Acute ischemic stroke; NIHSS: National Institute of Health Stroke Scale; MRI: Magnetic Resonance Imaging; CT: Computer Tomography; MCA: middle cerebral artery; CAD: coronary artery disease; HRT: hormone replacement therapy; TIA: transient ischemic attack; PVD: Peripheral vascular disease; ROC: Receiver Operating Curve; INR: International Normalized Ratio; HRV: heart rate variability; TP: total power; VLF; LF: low frequency; HF: high-frequency domains.
Author Contribution
CIN, SIN, AINOC, NK, and TIN designed the concept, experiment, and data analysis. CBS and KK critically revised the drafts and interpreted the results. All authors read and approved the last version of this manuscript. All authors have provided the corresponding author with permission to be named in the manuscript and approved the submission of this manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
This study was funded by NIH R25 grant ( Grant #; 5R25AG067934-04).
Availability of Data and Materials
The retrospective datasets are available by request from the corresponding author of this manuscript respectively.
Ethical Approval
This study was approved by PRISMA Health Upstate SC, the institutional review board of the Health institutional committee for Ethics.