
Abstract
Background:
Fabry disease is rare and multisystemic, necessitating a disease-specific quality of life scale to assess changes in quality of life. We developed the Adult Fabry Disease Quality of Life scale to measure the quality of life of adult patients with Fabry disease.
Objectives:
To confirm the reliability of the Adult Fabry Disease Quality of Life scale using the test–retest method and calculate the minimal important change.
Design:
This study was based on two questionnaire surveys conducted at approximately 2-week intervals in November and December 2024 in Japan.
Methods:
Twenty-eight participants completed questionnaires consisting of background information, the Adult Fabry Disease Quality of Life scale, and the Short Form-8. In the second survey, an anchor question with a 7-point Likert scale was added to assess changes in general health. The intraclass correlation coefficient for reliability and Cronbach’s alpha coefficient for internal consistency were calculated. For minimal important changes, the average value of the smallest change group for the anchor question was calculated.
Results:
The intraclass correlation coefficients for each factor and the total score on the Adult Fabry Disease Quality of Life scale were 0.892–0.946. Cronbach’s alpha coefficient was 0.948 for the first survey and 0.956 for the second. In response to the anchor question, three participants (13.0%) felt a little worse, and three (13.0%) felt a little better. Those who felt a little worse and those who felt a little better showed improvements in quality of life of 3.7 and 5.3 points, respectively.
Conclusion:
The Adult Fabry Disease Quality of Life scale is highly reproducible at 2-week intervals. Defining the minimum important change was not possible, which is important when used as an outcome. Future studies should establish it using the anchor method.
Trial Registration:
This prospective study was registered with the UMIN-CTR on September 1, 2024 (No. UMIN000055144).
Plain language summary
We created a questionnaire to measure the quality of life of adult patients with Fabry disease. To use this questionnaire in the future, its reliability must be verified. In this survey, the same patients were asked to complete two questionnaires at 2-week intervals. Twenty-eight patients with Fabry disease participated in this study. The results of the two surveys were almost identical, indicating that the questionnaire was reliable. Minimal changes in scores on the scale used to assess patients who subjectively reported that their overall condition had improved or worsened varied and could not be evaluated. Overall, the questionnaire that we created was reliable and can be used for future research. Next, the degree to which the questionnaire scores minimal change when the quality of life changes needs to be investigated.
Keywords
Background
Fabry disease is an X-linked disorder caused by pathogenic variants in GLA. Deficiency of the lysosomal enzyme α-galactosidase A (α-Gal A) leads to progressive accumulation of glycosphingolipids (e.g., globotriaosylceramide), resulting in multisystem manifestations. 1 As a rare disease, the estimated number of patients with Fabry disease in Japan is approximately 1600, or 1 in 80,000, 2 but the results of newborn screening are 1 in 11,854, 3 indicating a wide range of results. Fabry disease includes classic and non-classic (late-onset) phenotypes, and similar heterogeneity has been reported in female patients. 4 Classic patients present with the characteristic neuropathic pain, abdominal symptoms, and hypohidrosis from childhood. 1 Non-classic phenotype patients mainly develop symptoms such as heart, kidney, and circulatory problems during adulthood. Approved treatments include regular hospital visits for intravenous enzyme replacement therapy (ERT) and pharmacological chaperone therapy for patients whose genetic variant types match.1,5
Patients with Fabry disease present with a variety of symptoms depending on their age and disease phenotype, which affect their quality of life (QOL). The QOL of patients with Fabry disease is lower than that of the general population. 6 In addition, the QOL of patients with the classic phenotype is lower than that of patients with non-classic phenotypes. 7 During the COVID-19 pandemic, social restrictions reduced the physical and mental QOL of patients with Fabry disease. 8 General QOL scales, such as the EQ-5D and SF-36, have been used to survey QOL in these patients. A systematic review conducted on the QOL of patients with Fabry disease included 54 papers, most of which used general QOL scales rather than those specific to Fabry disease. 6 However, because Fabry disease is rare and presents with several symptoms throughout the body, a disease-specific QOL scale that can be used to examine changes in QOL in detail must be developed. 6 The only patient-reported outcome measure specific to Fabry disease was the Fabry-specific pediatric health and pain questionnaire. 9 However, this scale was designed for pediatric patients and struggled to comprehensively capture the QOL of adult patients who develop cardiac, renal, or cerebrovascular symptoms. Therefore, we developed the Adult Fabry Disease QOL scale (AFQOL), a disease-specific scale for measuring the QOL of adult patients with Fabry disease. 10 The AFQOL, developed based on interviews with patients, measures subjective evaluations in terms of work, interpersonal relationships, and symptoms (Figure 1).
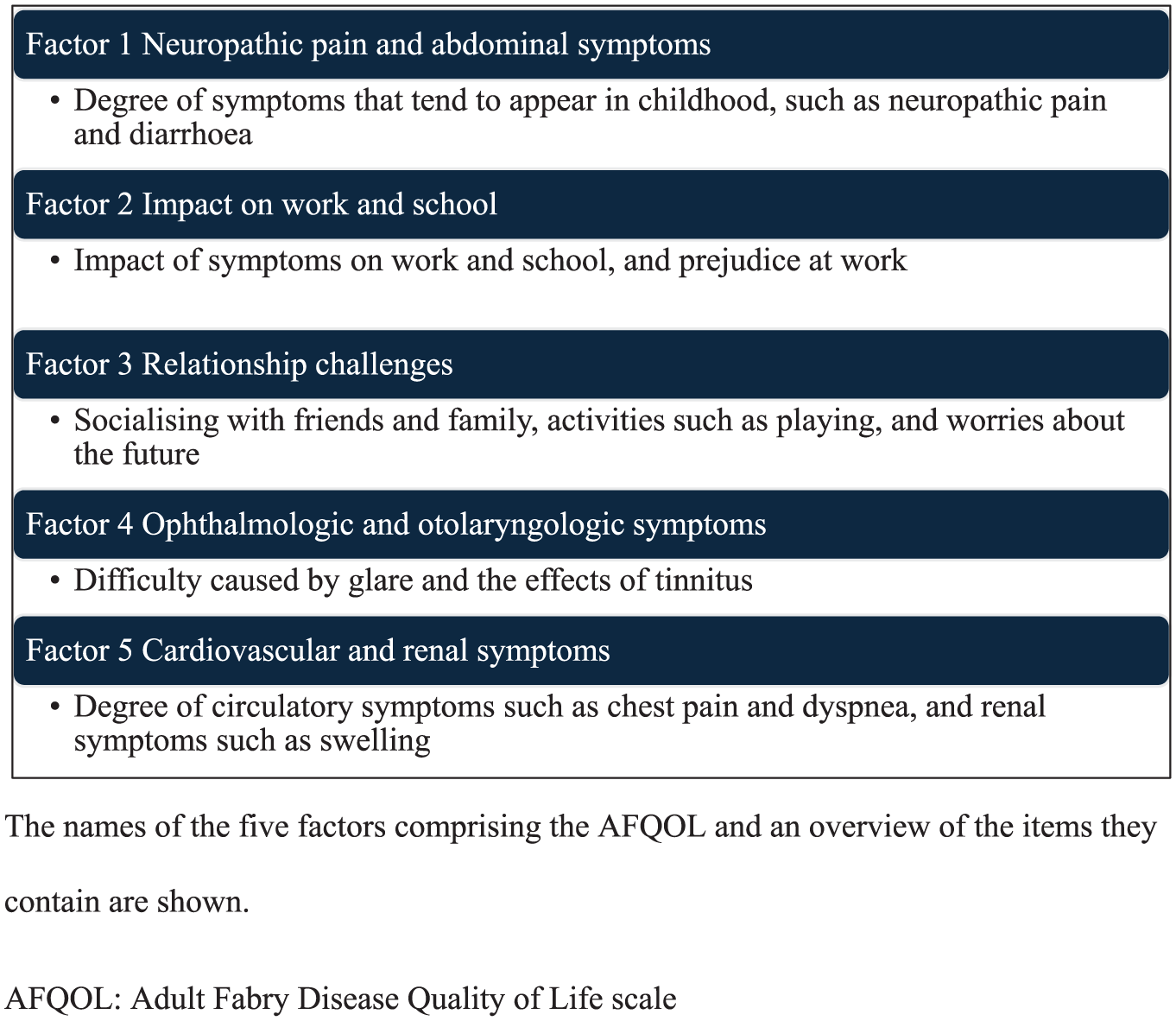
Factor structure of AFQOL.
The validity, reliability, and responsiveness of patient-reported outcome measures (PROM) must be verified. 11 AFQOL is useful in assessing patients with Fabry disease; however, its reliability has not been verified. Issues include test–retest reliability and validation of the minimal important change (MIC), 12 although the content validity and internal consistency of the AFQOL have been confirmed. 9 Therefore, we attempted to verify the reliability of the AFQOL using data from a longitudinal survey currently being conducted on patients with Fabry disease. This study aimed to confirm the reliability of the AFQOL using the test–retest method and calculate the MIC for the AFQOL. Confirmation of the reliability of the AFQOL will enable its use as a secondary outcome measure in future studies and clinical trials.
Methods
Design
We conducted a test–retest study using two online surveys administered approximately 2 weeks apart (November–December 2024) within a larger longitudinal cohort. This survey was part of a longitudinal study investigating the relationship between the disease-specific QOL of patients with Fabry disease and seasonal fluctuations in temperature. 13 This study aims to verify the reliability and preliminary validity evidence of the scale. The longitudinal study objectives, temperature changes, and QOL will be published in a separate paper.
This study was based on two questionnaire surveys conducted at approximately 2-week intervals in November and December 2024 in Japan. The reason for determining this 2-week interval was that aligning it with the ERT interval for Fabry disease was considered to facilitate future acceptability.
This manuscript was also prepared in accordance with the STROBE guidelines. 14
Participants
This study included patients aged ⩾ 18 years who had been diagnosed with Fabry disease. Patients hospitalized for acute conditions at the time of recruitment, or those unable to self-report questionnaire responses because of cognitive impairment or intellectual disability, were excluded.
We consulted with a statistics expert during the planning phase. Given that Fabry disease is a rare disorder, making participant recruitment difficult, and that limited data exist regarding the mean and standard deviation of the AFQOL, we did not determine the sample size based on conventional power analysis. Instead, we aimed to collect as many samples as possible to gain further insight.
Participants were recruited through the Japan Registration System for Metabolic and Inherited Diseases, the patient registry of the Japanese Society for Inherited Metabolic Diseases, and lysosomal disease specialists. Patients who had been diagnosed with Fabry disease were provided with an explanatory document, and those who wished to participate were registered using a questionnaire form on the website. Written informed consent was obtained from all participants included in the study. Twenty-eight participants wished to participate in this longitudinal study.
Data collection
For this survey, we sent the first and second questionnaire forms to the participants’ email addresses and asked them to complete the questionnaire online. We gave the participants 1 week to respond to the questionnaire after sending it out; if they did not respond within that week, we sent them another email to prevent them from dropping out.
In the first survey, questions about participants’ background information, AFQOL, and Short Form-8 (SF-8) scores were investigated. Background information included sex, age, place of residence, disease category, age at diagnosis, method of diagnosis, treatment, outside temperature, and use of air conditioning. Regarding the expression type in female patients, it was assumed that many had been diagnosed with the heterozygous type in Japan and were unaware of whether they were classical or non-classical. Therefore, the questionnaire options used were heterozygous. The second survey included questions on the outside temperature, air conditioning, AFQOL, and anchor items for measuring MIC.12,15 The anchor item was a 7-point Likert scale that asked about changes in general health over the period since the first survey, with the following answers: “worst ever,” “much worse,” “a little worse,” “no change,” “a little better,” “much better,” and “best ever.”
AFQOL
We developed the AFQOL as a disease-specific QOL scale for adults with Fabry disease. 10 The AFQOL consists of 39 items and 5 factors: “neuropathic pain and abdominal symptoms (10 items),” “impact on work and school (6 items),” “relationship challenges (11 items),” “ophthalmologic and otolaryngologic symptoms (5 items),” and “cardiovascular and renal symptoms (7 items).” Each item was rated on a 5-point Likert-type scale (always, often, sometimes, seldom, and never): 4 = “always” and 0 = “never.” Higher total and factor scores indicated lower QOL.
SF-8
The SF-8 is a general QOL scale consisting of eight items, although a Japanese version has been developed.16,17 The scores are standardized for each component, with an average of 50 points; a higher score indicates a higher QOL.
Statistical analysis
Descriptive statistics were used to analyze the data. Cronbach’s alpha coefficients were calculated for the internal consistency of each factor and the total AFQOL score. To assess test–retest reliability, intraclass correlation coefficients (ICC) were calculated for each factor and the total AFQOL score in the first and second surveys. The ICC (A,1), a two-way mixed-effect analysis of variance model with interaction for absolute agreement between single scores, was used in this study. 18 The mean change in AFQOL scores between the first and second surveys was calculated for participants with the smallest change (-1 or 1) in anchor items. Spearman’s ρ was used to measure the correlation between score changes and responses to the anchor questions. For the first survey, AFQOL, background information, and SF-8 were analyzed using Spearman’s correlation coefficient and an unpaired t-test.
Statistical analyses were performed using SPSS (version 29.0; IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05.
Results
Registrant information
We received 28 responses for the first survey and 23 for the second survey. Most participants lived in Osaka (seven participants) or Tokyo (seven participants), and the rest were distributed from Hokkaido to Kumamoto. The descriptive statistics are presented in Table 1. Of the 28 participants, 15 were women. The mean age of participants was 47.3 years, ranging from 23 to 68 years. The disease type was self-reported by patients, with five responding that it was “unknown.” All 15 female patients were considered heterozygous, while 12 of the male patients reported having the classic form, and 1 was “unknown.” The most common method for definitive diagnosis was genetic testing (12 patients, 42.9%), followed by enzyme activity testing (7 patients, 25.0%). Others listed included “combining family history with genetic testing,” “symptoms such as burning pain,” “kidney biopsy,” and “unknown.” Regarding treatments that participants had previously received, 82.1% had received ERT and 17.9% had received pharmacological chaperone therapy. In addition, they had experience with pain relief (35.7%) and cardiovascular medications (25.0%).
Characteristics of participants and scale scores (n = 28).

ERT, Enzyme replacement therapy; SD, Standard deviation.
Descriptive statistics for scales
The AFQOL results of the first and second surveys are presented in Table 2. The average total AFQOL score for the first survey was 57.0 points, and that for the second survey was 53.3 points (Figure 2). The SF-8 was answered during the first survey, with an average physical component score of 48.5 and an average mental component score of 46.9.
Factors and total score for scales.

MCS, Mental component summary; PCS, Physical component summary; SD, Standard deviation.

Distributions of AFQOL total score.
When comparing the AFQOL total score by sex, men (64.8 points) had a lower QOL than women (50.3 points). Cronbach’s alpha coefficient, which indicates the internal consistency of the scale, was 0.948 for the first survey and 0.956 for the second. The results of the correlation between the factors and the correlation between AFQOL and SF-8 are shown in Table S1.
Comparison of surveys
The anchor item asked about changes in conditions from the first to the second survey. Three participants (13.0%) answered that they felt a little worse, 16 (69.6%) felt no change, three (13.0%) felt a little better, and one (3.6%) felt much better.
The change in AFQOL scores was calculated from the first to the second time using the following formula:
Score change = results of first survey–results of second survey
A large change indicates an improvement in QOL. The mean change was less than 1 point for each factor (0.8 for factor 1, 0.8 for factor 2, 0.2 for factor 3, −0.4 for factor 4, and 0.0 for factor 5) and 1.5 points for the total score.
The ICC for each factor and the total score ranged from 0.892 to 0.946 (Table 3). To calculate the MIC, we checked the change in AFQOL for the three participants who felt a little worse and those who felt a little better on the anchor item (Table 4). The general condition worsened slightly; however, the AFQOL improved slightly. The mean change in AFQOL for participants who answered “a little better” was an improvement of 5.3 points. The correlation coefficient between the change in scores in this survey and responses to the anchor question was ρ = 0.032 (p = 0.886).
Intra-class correlation coefficient (A, 1) for AFQOL (n = 23).

AFQOL, Adult Fabry Disease Quality of Life scale; CI, Confidence interval; ICC, Intraclass correlation.
Change in general condition and change in AFQOL.

AFQOL, Adult Fabry Disease Quality of Life scale; SD, Standard deviation.
Discussion
This study confirmed the reliability of the AFQOL using the test–retest method. For all factors and total scores, the lower limit of the 95% confidence interval for ICC was greater than 0.75, indicating that the AFQOL is reproducible. 19 There are several formulas for calculating the ICC, depending on the model and the way the numerical values are handled; however, in this study, ICC (A,1) was used in accordance with the guidelines to confirm the reliability of the PROM test–retest. 18 Although there are several PROMs developed for patients with Fabry disease,20–22 only the symptom severity scale developed by Hamed et al. 23 has been reported to have good test–retest reliability. As a result, it is possible to compare the subjective evaluations of adult patients with Fabry disease at multiple points in time using the AFQOL. ERT is the primary treatment for Fabry disease. 1 Several enzyme preparations can be used by patients with Fabry disease, who need to visit the hospital every 2 weeks for intravenous administration. 5 The fact that the AFQOL showed reliability at approximately 2-week intervals demonstrated the reliability of the scale using ERT timing and increased AFQOL feasibility.
The internal consistency of the factors and the total scores of the AFQOL were very high. During the scale development stage, items with high item-item correlation and low item-total correlation were excluded. 10 In this survey, unlike in the development stage, the items in the questionnaire were grouped by factor, which improved internal consistency.
In this survey, we collected data from both male and female patients. Considering the severity of symptoms, it is reasonable to assume that the QOL of classic males is lower than that of heterozygous females. A systematic review reported that male patients with the classic phenotype have a lower QOL and face more challenges than female patients. 24 This suggests that the AFQOL can detect sex-related differences in QOL and may be responsive to clinically meaningful change.
Defining the MIC for AFQOL was not possible. Lack of correlation between score changes and anchor questions further supports this fact.
Fabry disease is rare; thus, collecting data from a large number of participants is difficult. 2 No scale can present the MICs for PROM in Fabry disease.9,20–22 Although the MIC may be indicated by distribution or standard deviation, confirming that this is appropriate for PROM, which is a subjective evaluation by the patient, is difficult. 12 To identify the MIC for the AFQOL, it may be necessary to accumulate and integrate results from future studies using the anchor-based approach. Although this study attempted to define MIC using a 2-week interval aligned with ERT, this was not successful, likely because such a short interval was insufficient to capture meaningful changes in symptoms and daily functioning. Defining an appropriate MIC will therefore require longer-term follow-up, such as through patient registries, and the accumulation of AFQOL data assessed at longer intervals (e.g., 4 or 8 weeks). In the present study, the responsiveness of the scale could not be established. Future research should further examine construct validity and responsiveness by increasing the sample size and incorporating additional psychological measures.
Limitation
This study had some limitations. First, the number of participants was small; therefore, caution should be exercised when interpreting results. Therefore, it may be difficult to interpret the findings of this study as representative of the overall QOL of all patients in Japan. Furthermore, robust calculation of QOL by disease type or treatment experience is challenging and requires caution in interpretation. This limitation is partly attributable to the absence of a priori the absence of sample size calculation; therefore, future studies should aim to include a statistically justified sample size. Second, the distribution of the AFQOL is similar to the data used in the development of the scale and is thought to reflect the situation of patients with Fabry disease in Japan. 10 However, only three cases were used to calculate the MIC; therefore, the individual effect was strong. It is necessary to continue accumulating knowledge about MIC through future surveys. Furthermore, this study did not collect information on the specifics of treatments, such as ERT. QOL at the time of response may fluctuate depending on factors such as the timing immediately after ERT treatment or the frequency of analgesic use. Future studies should evaluate the impact of these factors on AFQOL scores and treatment outcomes.
Conclusion
In this study, disease-specific QOL of patients with Fabry disease was investigated using a newly developed scale. The high correlation between the two time points and internal consistency indicate that the AFQOL is a highly reproducible scale. However, clearly defining the MIC, which is important when using it as an outcome, was not possible. Because the change in AFQOL scores showed no meaningful correlation with the anchor rating (ρ = 0.032), anchor-based estimation of MIC was not supported in this dataset. In future surveys, it will be necessary to accumulate findings using the anchor method and use them to calculate the MIC.
Supplemental Material
sj-docx-1-trd-10.1177_26330040261433034 – Supplemental material for Reliability assessment using the test–retest method and minimal important changes in the Adult Fabry Disease Quality of Life Scale
Supplemental material, sj-docx-1-trd-10.1177_26330040261433034 for Reliability assessment using the test–retest method and minimal important changes in the Adult Fabry Disease Quality of Life Scale by Yuta Koto, Masami Tanaka, Mitsuyo Ishiura, HyeSook Kim, Atsushi Ohashi, Nozomi Hadano, Aya Narita and Norio Sakai in Therapeutic Advances in Rare Disease
Footnotes
Acknowledgements
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.