
Abstract
Background:
Clinical studies have begun to evaluate therapeutic approaches to address the widespread neurodevelopmental and mental health challenges associated with a group of genetic syndromes known as “RASopathies.” However, the perspectives of patients and families regarding the relevance and accessibility of such treatment approaches have not been studied.
Objectives:
To assess the mental healthcare needs and treatment experiences encountered by individuals with RASopathies and caregivers.
Design:
Directed content analysis of focus group and interview transcripts.
Methods:
We qualitatively analyzed data from four virtual focus groups comprised of caregivers (n = 21) of youth with RASopathies and a series of individual interviews with young adults (n = 11) with RASopathies. Perspectives on primary neurodevelopmental and mental health concerns, treatment history, and care accessibility were explored using a directed content analysis framework.
Results:
Consistent with prior research, participants reported that attention/executive functioning, mood, and social concerns were common; anxiety was a particularly frequent comorbidity. Mental health concerns varied across settings and frequently interfaced with physical health symptoms. Barriers to care included poor accessibility of services, adverse medication effects, and a lack of provider experience or knowledge. Addressing neurodevelopmental and mental health symptoms effectively often necessitates family resilience and advocacy on the part of patients and their caregivers. Emergent themes uncovered needs for provider training pertaining to rare diseases, trauma-informed care, and improved community awareness regarding RASopathies.
Conclusion:
This study identified a set of actionable items to inform research, care delivery, and advocacy that reflect the expressed needs and lived experiences of participants representing both caregivers and patients with RASopathies.
Plain language summary
New treatments are being developed and tested to address neurodevelopmental and mental health challenges of people with RASopathies, yet there is a lack of research exploring the patient experience when accessing existing treatments and perceived barriers to care. Our team conducted and analyzed a series of focus groups and interviews with caregivers and young adults with RASopathies. We asked about mental health concerns, treatment history, care accessibility, and ideas for treatment approaches to better meet their needs. Results identified a wide variety of mental health conditions and treatment strategies, with anxiety being a particularly frequent area of concern. Mental health conditions frequently interfaced with physical symptoms. Caregivers and individuals with RASopathies frequently struggled to access care, had adverse medication effects, or encountered providers with a lack of experience or knowledge of RASopathies. Advocacy from patients and their families was often needed to successfully address neurodevelopmental and mental health symptoms. Several themes emerged from these conversations, including needs for provider training in rare diseases, trauma-informed care, and improved community awareness regarding RASopathies. This study identified a set of actionable items to inform research, care delivery and advocacy that was informed by the perspectives of both caregivers and patients with RASopathies.
Keywords
Introduction
While rare diseases are frequently understudied and lacking in adequate treatment options, the neurodevelopmental and mental health conditions that accompany them are a particular area of unmet need.1–3 The RASopathies are a group of complex rare disorders caused by gene variants that disrupt signaling through the Ras/mitogen-activated protein kinase (RAS/MAPK) pathway. 4 This dysregulated signaling can impact numerous processes involved in brain development, leading to effects on learning, attention, social skills, emotion regulation, and behavior.5,6 A range of physical health manifestations is also observed, including craniofacial features, cardiac disease, gastrointestinal issues, dermatologic findings, and increased risk for malignancies. The collective incidence of RASopathies is approximately 1:1000 to 1:2500 births. 7 Neurofibromatosis type 1 (NF1), Noonan syndrome (NS), cardiofaciocutaneous (CFC) syndrome, and Costello syndrome (CS) are the most well-known of these conditions.
Neurodevelopmental complications are observed in all RASopathies, but the prevalence and constellation of specific symptoms vary within and across diagnostic groups. Intellectual disability is considerably more common among individuals with gene variants that affect downstream components of the RAS/MAPK pathway (e.g., those causing CS and CFC), than those that affect transducers upstream of RAS (e.g., those causing NF1 or NS). 8 In NF1 and NS, overall intellectual functioning is often age-appropriate, but effects on specific aspects of learning, attention, or processing are widely observed.9,10 All RASopathies are associated with an increased risk for social challenges and symptoms of autism spectrum disorder (ASD),11,12 with the highest rates of autism traits (e.g., repetitive behaviors, differences in social communication) observed in CFC.13,14 A higher frequency of internalizing (e.g., anxiety, mood disturbance) and externalizing (e.g., impulsivity, aggression) behaviors has also been reported across all RASopathies.15–18 Anxiety in particular has been noted as a prevalent comorbidity among individuals with CS.19,20
Despite evidence of widespread neurodevelopmental and mental healthcare needs experienced by individuals with RASopathies, few resources have been dedicated to the development and evaluation of interventions to address these concerns. A small number of studies have investigated pharmacological therapies, primarily in patients with NF1. Stimulant medications have shown efficacy in treating social challenges, aggressive behaviors, and symptoms of attention deficit hyperactivity disorder (ADHD) in NF1.21,22 Other psychiatric medications, including antidepressants and antipsychotics, have been reported on in observational studies of NF1 and CS; however, their effectiveness remains unclear, with some reports of adverse reactions.20,23 RAS-targeted therapies such as MEK inhibitors, which aim to address the RAS/MAPK pathway directly, have demonstrated efficacy in reducing physical symptoms (e.g., tumors, cardiomyopathy), but their utility in addressing cognitive and behavioral concerns has not been well-established.24–26 Similarly, despite basic research showing that antiseizure drugs (e.g., lamotrigine) and statin drugs can improve learning and memory function in animal models of NF and NS, clinical trials with humans have not produced strong evidence of efficacy.27–33 In terms of psychotherapeutic approaches for RASopathies, trials of a telehealth group social skills intervention, social cognitive training, mind-body therapy, acceptance and commitment therapy, and a working memory training program have all yielded preliminary evidence of feasibility and/or efficacy to improve aspects of cognitive function or behavioral health.34–39
As established and emerging therapies to address neurodevelopmental and mental health conditions in RASopathies are investigated, it will be critical to focus resources on interventions that have high relevance and accessibility within patient communities. Identifying which care needs are perceived as most pressing for patients and their families, which treatments are routinely utilized by individuals with RASopathies, and the degree to which families consider these treatments accessible is of fundamental importance. 40 Additionally, research aimed at identifying caregiver challenges remains limited despite evidence of elevated parenting stress and unmet needs across RASopathies.41–43 Studies reporting higher stress levels among caregivers of children with RASopathies who have greater emotional and behavioral difficulties suggest that intensified focus on interventions to alleviate these difficulties could improve quality of life for family members.41,44,45 To advance treatment development and delivery, we engaged both patients and caregivers in focus groups and interviews to elicit their perspectives surrounding neurodevelopmental and mental healthcare services. We focused on the period between childhood and early adulthood, a key developmental window during which symptoms are most likely to emerge and caregiving demands are often substantial. 46 Our study team then qualitatively analyzed the interview transcripts to address the following research questions:
What types of neurodevelopmental or mental health concerns were individuals with RASopathies experiencing?
What treatments and supports were families utilizing to address those concerns?
What were the primary barriers and facilitators to treatment for mental health concerns?
What themes emerged regarding the experience of mental health symptoms and treatment?
Method
Participant recruitment and enrollment
Study participants were recruited through multiple channels, including a database of prior participants in research studies by our team, email listservs, and social media postings by patient advocacy groups (CFC International, Costello Syndrome Family Network, Children’s Tumor Foundation, NF Midwest, NF Network, Noonan Syndrome Foundation, RASopathies Network). Participants were included if they were English-speaking and identified themselves either as a caregiver of a child or young adult (aged 3–25 years) with a RASopathy, or as a young adult (aged 18–28 years) with a RASopathy. (Note. We defined the term caregiver to encompass any adult who supports decision-making and functional participation in educational, health care, daily living, and/or community settings for at least one individual with a RASopathy, such as a parent or guardian.) Exclusionary criteria were: lack of English language fluency; not being within the age ranges noted above; or lacking either a diagnosis of NF1, NS, CFC, or CS or a child with one of these diagnoses. Individuals with RASopathies who were unable to understand and appreciate the study information provided, as per assessment with the University of California, San Diego Brief Assessment of Capacity to Consent, 47 were also excluded. Participation was limited to one individual per family.
Prior to data collection, an informed consent process was conducted via private videoconferencing meetings using e-consent documentation. Twenty-one caregivers consented to participate in 1 of 4 focus groups, each dedicated to one of the major RASopathy syndromes. Additionally, 11 young adults with a RASopathy consented to participate in private semi-structured interviews. The study duration was from May 2023 to April 2024. Table 1 displays aggregated demographics of individuals with RASopathies reported on in these focus groups and interviews. Participant numbers are provided to accompany illustrative quotes in text and tables, but these quotes are not connected to specific attributes to maintain participant privacy.
Demographics and diagnostic features of individuals with RASopathies reported on in caregiver focus groups and young adult interviews. RASopathy diagnosis is denoted by the presenting clinical syndrome and gene affected.

CFC, Cardiofaciocutaneous syndrome; CS, Costello syndrome; NS, Noonan syndrome; NF1, neurofibromatosis type 1.
Data collection
Transcripts for thematic coding were obtained from each of four virtual caregiver focus groups led by a postdoctoral researcher and a post-graduate research assistant (each lasting approximately 75 min) and 11 semi-structured individual interviews led by a post-graduate research assistant (each lasting approximately 25 min). Participants in both groups were asked the same open-ended questions regarding primary neurodevelopmental or mental health concerns (if any), treatment history related to such concerns, experiences obtaining care, and perspectives regarding potential future treatments or support that might be helpful. Focus groups and interviews were recorded and transcribed by the University’s HIPAA-compliant videoconferencing platform. All video recordings were reviewed by a research assistant to ensure accuracy of the transcriptions, and the corresponding transcripts were de-identified prior to analysis.
Data analysis
We conducted a directed content analysis 48 using a hybrid deductive–inductive coding approach. Initially, raw data from focus group and interview transcripts were coded using a deductive codebook informed by existing literature and clinical experience with RASopathies. During this process, several data segments did not align with the predefined codes. These unmatched statements were grouped inductively based on conceptual similarity and discussed among the research team. From these groupings, new codes were defined and organized into broader categories. While qualitative methods primarily guided the coding and interpretation of participants’ experiences, our content analysis also incorporated visualizations and descriptive summaries of code frequencies to enrich the qualitative findings. To address Research Question 4, inductively derived codes were synthesized to develop overarching themes that captured the most salient patterns in the data. The saturation of themes was determined by the absence of new codes emerging in the iterative coding process, consistent with explanations of data saturation in scholarly literature. 49 When new data (i.e., additional transcripts) yielded no additional codes/themes and instead repeated what was in previous data, focus group and interview data were considered saturated. The data analysis procedure and code formulation process are visualized in Figure 1.

Data analysis process reflects a directed content analysis framework for coding focus group and interview transcripts.
Codebook development
The initial deductive codebook was collaboratively developed by a faculty researcher, a postdoctoral researcher, and two graduate student research assistants (herein referred to as researchers). Codes were selected based on empirical research on neurodevelopmental and mental health concerns across RASopathy conditions13,16,19,50,51 as well as extensive prior communication and experience with families affected by RASopathies across clinical, research, and community settings. Codes were operationally defined, and the initial codebook was input into NVivo 1.71.
Focus group coding
After initial familiarization with the transcripts and deductive codebook, two researchers independently conducted descriptive coding of each transcript. Next, the researchers met for consensus review to evaluate consistency regarding the number of mentions across all focus group transcripts for each code and the mapping of quotes/content to each code. They discussed iterative changes or additions to the codebook needed to reflect emerging concepts and themes. The same process was followed for each consecutive transcript. The coding categories were then refined and reorganized, and the focus group codebook was reviewed and finalized.
Interview coding
Minor terminology modifications were made to the focus group codebook to enable accurate coding for interview transcripts (e.g., referring to “individuals” rather than “caregivers”). Under the supervision of a graduate student, research assistants independently coded each transcript. Consensus review of transcripts was completed to inform necessary modifications to the codebook. 48 The researchers concluded that saturation had been reached when no new coding categories were added to the final transcripts. 49 The finalized interview codebook was reviewed and approved by the research team (see Table 1, Supplemental Materials).
Data validation and triangulation
To increase the rigor of the study, the team collected data via multiple sources (i.e., caregiver focus groups and patient interviews) and across the four major RASopathies. The investigators also engaged in peer debriefing prior to and in critical stages of analysis, such as after the initial focus group coding, after completion of all four focus groups, at multiple points during coding of interviews, and throughout manuscript preparation. To align with recommended standards for qualitative patient-centered research, reflexivity was incorporated into the research process through each researcher’s self-reflections about how their own positionality and characteristics could have influence on the results of this study.52,53 The author Positionality Statement is available in the Supplementary Materials. The reporting in this study conforms to the COREQ statement. 54
Results
Research question 1: What types of neurodevelopmental or mental health concerns were individuals with RASopathies experiencing?
Areas of concern described by patients and caregivers were classified across 10 domains (Figure 2). Notably, 4 of 5 domains discussed by the highest proportion of individuals were the same across the caregiver and young adult cohorts: anxiety; attention and executive function; mood (depressed mood or mood dysregulation); and social concerns. Anger and conduct concerns were described as the fifth most-frequently mentioned issue among caregivers, whereas sleep was the fifth most-frequently mentioned among young adults with RASopathies. Supplementary Table 1 provides specific information regarding the number of participants endorsing and the total number of mentions across transcripts for each domain.

Neurodevelopmental and mental health concerns mentioned by study participants.
We also coded subcategories of concerns. Note that for each fraction, the numerator represents the number of mentions within a subcategory (e.g., a specific type of anxiety) and the denominator represents the number of mentions within a larger category (e.g., anxiety). For most mentions by caregivers (38/59) and young adults (41/65) pertaining to Anxiety, comments were general (e.g., “I’ve experienced anxiety” (YA04)) and were not linked to a specific anxiety subtype. Regarding Attention & Executive Functioning, comments were typically about ADHD or problems paying attention (36/47 for caregivers, 27/30 for young adults). One caregiver explained, “I have been noticing he cannot focus on anything, like playing with a particular toy or swinging or any activity for say, definitely for 10 minutes at a stretch, but the school reports that his attention span is more like 3 minutes” (CG10). In the Mood Concerns category, caregivers most often shared observations related to mood changes or dysregulation (26/41). One parent described, “we’ve had outbursts, where he just will start shutting down and won’t communicate to anybody” (CG01). Mentions by the young adults in the Mood Concerns category typically involved specific mentions of depression (31/33). Regarding Social Concerns, most mentions by caregivers were related to relationships or social skills (30/34). One caregiver expressed concern about the lack of involvement of peers in her child’s life, questioning “where are her friends from school coming over for birthday parties or going to the park or watching a movie?” (CG19). Social Concerns among young adults typically centered around experiences of being the victim of bullying (8/10). One participant shared, “I was diagnosed with a brain tumor, and that same year I was getting bullied to the extreme at school. . .it was a horrible year for me” (YA04).
Research question 2: What treatments and supports were families utilizing to address those concerns?
Figure 3 depicts the primary groupings of interventions that families used to address neurodevelopmental or mental healthcare needs and associated subcategories. Data regarding the frequencies of participant mentions for each of these treatment/support modalities is available in Supplemental Table 2. The Therapy and Medication codes were mentioned by most participants. Therapy subcategories included developmental therapies (e.g., speech/language therapy, occupational therapy), outpatient behavioral or mental health therapies (e.g., applied behavior analysis, cognitive behavioral therapy), inpatient mental health therapies, and undefined therapies. In terms of medications, individuals from both cohorts reported use of medications addressing ADHD (n = 6), sleep (n = 6), mood/anxiety/behavior (n = 6), seizures/pain/migraines (n = 6), as well as dietary supplements (n = 5).

Treatments or supports for neurodevelopmental and mental health concerns utilized by individuals with RASopathies as reported in caregiver focus groups and young adult interviews.
School supports were more commonly mentioned by caregivers (14 caregivers with 32 total mentions) versus young adults (3 young adults with 8 total mentions). Special education instruction, such as the presence of Individualized Education Programs, was discussed along with classroom accommodations, including structured break times and the use of sensory objects. Further school supports included small class sizes, homeschooling, and staff support (e.g., advocacy of staff members, effective collaboration with staff members, and teachers who were understanding of RASopathies symptoms). Family-based interventions were also mentioned more frequently by caregivers (16 caregivers with 32 total mentions) than by young adults (2 young adults with 2 total mentions). These supports included strategies for communication and for providing the necessary structure to tasks and activities. Regarding community groups/supports, engagement in extracurricular activities and social groups was most frequently endorsed. Individual coping strategies were mentioned by 4 young adults (8 mentions) but not by any caregivers. Examples of coping strategies included physical activity, sleep tracking, having a structured schedule, task reframing, and dietary changes.
Research question 3: What were the primary barriers and facilitators to treatment for mental health concerns?
Study participants discussed barriers (i.e., factors that prevented or made it more difficult to access or continue treatment) and facilitators to care (factors that supported initiating or maintaining access to services) (Figure 4). The top 5 barriers to treatment for caregivers, in order from most mentioned to least, included: scheduling (e.g., waitlist, unavailable providers); insurance coverage; medication barriers; distance to services; and time commitment. In comparison, the top 5 barriers reported by young adults were medication barriers; lack of alliance or alignment with provider; provider lack of expertise; scheduling; and government or community systems. Two barriers common to both data sets were related to scheduling and adverse medication effects. Both young adults and caregivers struggled to find appointments with providers due to waitlists and other delays. While medication was described as helpful for many participants, some individuals reported that medication side effects were a barrier to continuing treatments. One young adult shared, “[The medication] just made all my mental stuff 10 times worse . . . I was too scared to do medication for like 5 years” (YA10).

Barriers and facilitators to care endorsed by young adults and caregivers. Responses were categorized under four domains. Accessibility factors were defined as those related to a participant’s ability to initiate or continue treatment; individual/family factors referred to the patient or family’s knowledge, resources, attitudes, or experiences that could influence treatment; provider factors were specific to the qualities or experiences of clinicians working with the patient; and systemic barriers and facilitators were those related to institutions of power such as governments or school districts, as well as the impact of larger world events.
Caregivers often cited accessibility as a considerable barrier to care. One caregiver mentioned: “I want to do so many things for him, but I just don’t have the time with my job” (CG06). Family financial resources also prevented access to services, with a caregiver noting “sometimes you have to go outside my insurance, and to get somebody who really can help, a real good fit . . . it can be expensive” (CG01). Young adults focused more on challenges related to alliance with providers. One young adult noted “therapy. . .it really just kind of solidified my distrust in adults . . . it’s definitely made it so I was just kind of struggling alone quietly” (YA09). Another voiced frustration over the lack of knowledge about RASopathies among providers: “Finding providers that understand my conditions is difficult . . . they don’t understand my condition at all. And that makes it very frustrating to get the care that I need. Not just in mental health care, every kind of care.” (YA01). Caregivers also endorsed barriers related to a lack of alliance with providers or encountering inexperienced providers, but to a lesser extent than young adults. Both groups identified diagnostic labels as barriers. More specifically, they described not being able to access services due to rigid diagnostic criteria for a mental health condition. One caregiver stated, “He’s like just in all these little corners, you know, not quite in a category to receive services” (CG06).
In terms of facilitators of care, several differences were apparent between caregivers and young adults. Caregivers highlighted advocacy and family resilience (defined as: how families derive meaning from their experiences to cope with challenges 55 ) as important facilitators, whereas young adults placed greater emphasis on provider fit. Family resilience was mentioned by seven caregivers (11 total mentions), but not by any young adults. One caregiver noted, “It’s mostly. . .taking things as they come and finding out the path once I have to walk down [it]” (CG14). Although not mentioned by young adults, caregivers also frequently cited job flexibility and service modality options as facilitators. Both groups, however, underscored the significance of advocacy. Advocacy referred to instances where individuals sought improvements in services by requesting changes in the quality, focus, or availability of services. For example, one participant shared, “I pushed pretty hard to get handwriting support for the dysgraphia” (CG17). Another caregiver experienced relief after finally being approved to start sessions with a behavior therapist to receive parent training, stating, “it’s something I’ve always wanted. I wished it was available. It wasn’t. But so I just kind of had to beg for it.” (CG13)
Research question 4: What themes emerged regarding the experience of mental health treatments?
Research question 4 focused on key themes that arose when study participants shared about their mental healthcare experiences. Four themes were identified across the caregiver and young adult samples: complex constellation of symptoms; shifting neurodevelopmental and behavioral concerns; being different & lack of community knowledge about RASopathies; and suggested treatments or supports to improve care (Table 2).
Key themes identified through content analysis of focus group and interview transcripts.
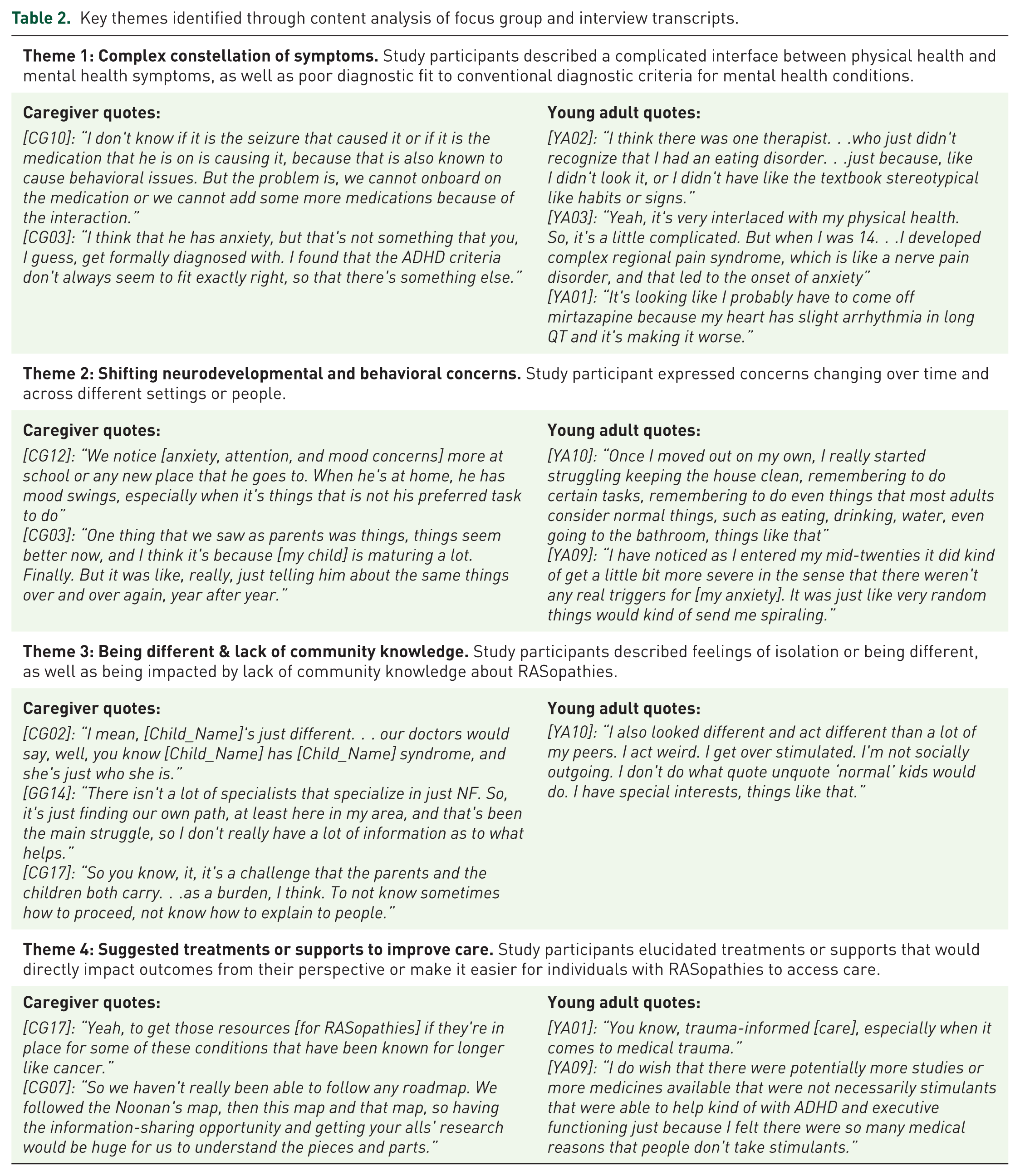
Theme 1: Complex constellation of symptoms
The complicated interface of physical and mental health symptoms surfaced as a theme for both caregivers and young adults. Participants frequently described how physical symptoms (e.g., pain, increased histamine, challenges swallowing, tumors, joint disorders) led to or exacerbated mental health symptoms such as depression, anxiety, or trauma. One caregiver shared about the influence of epilepsy on mental health: “I saw my son was a very happy kid. Then seizure struck him. . .we have been seizure-free for 4 and a half years, but ever since that seizure, we have seen a huge change in his behavior” (CG10). Two young adults mentioned that physical health conditions (e.g., cardiac conditions) increased anxiety; at the same time, some individuals had to stop taking medications for their mental health concerns because of adverse impacts on their medical condition (e.g., tachycardia). Medications for physical health conditions were also described to have unintended mental health effects. One caregiver mentioned that a medication prescribed for plexiform neurofibromas caused adverse effects (e.g., rash, hair loss) that led to worsening anxiety and depression for their child.
The complex constellation of symptoms experienced by individuals with RASopathies also contributed to delayed diagnosis or misdiagnosis. In some cases, diagnostic delays were attributed to the provider(s)’ lack of experience. In other cases, delays or misdiagnoses may have been related to the individual’s symptoms not fitting within conventional diagnostic categories. A particular source of diagnostic uncertainty mentioned by both caregivers and young adults was the considerable overlap in symptoms of ADHD and autism. One young adult emphasized that mental health is “not one-size” (YA02) and that mental health conditions do not present the same way across people.
Theme 2: Shifting neurodevelopmental and behavioral concerns
A second theme expressed by participants was changing symptom presentation across time, setting, or person. Some participants described an evolution of neurodevelopmental and behavioral concerns at different ages. For example, a child’s night terrors at age 4 evolved into broader anxiety later in development. Another child exhibited changes in sensory responsiveness over time, shifting from a pattern of avoiding stimulation toward one of seeking it. Multiple young adults described attention challenges as a dominant theme in the school-age period, whereas depression and anxiety became increasingly apparent in adolescence or later. Some caregivers reported that maturation-related changes, such as puberty, negatively impacted their child’s mental health or behavior, whereas others expressed that maturity brought increased self-management and coping skills for their children. Changes also occurred in terms of symptom severity. For several young adults, mental health symptoms worsened as they reached adulthood, with newly emerging triggers or symptoms (e.g., shaking hands, fast heartbeat).
Symptoms often varied across settings. Several caregivers described anxiety or behavior concerns as particularly apparent in new settings or settings associated with negative experiences (e.g., doctor’s office). Many participants mentioned the school environment as an important reference point. Caregivers often reported observing more concerns in the school than home setting, where “there are not as many expectations” (CG07) or caregivers feel they have more control. Caregivers reported a variety of challenges in the school setting, such as anxiety, attention difficulties, and externalizing behaviors, sometimes in response to sensory needs, culture, differences in learning, or requests from staff to complete non-preferred tasks. They also reported having struggled to communicate with school staff to foster understanding of their child’s needs and to keep “a common language between home and school” (CG19). Young adults expressed similar themes, including difficulties learning in a traditional setting as well as negative experiences in school (e.g., expulsions). Finally, transitioning from high school to college or a career was reported to be difficult, often related to reduced structure compared to the school years.
Behavioral concerns, particularly regarding anxiety and mood, also differed depending on the individual’s preference for or familiarity with the person with whom they were interacting. Caregivers described mood and behavior changes when their child was interacting with a particular person (e.g., other family member, school paraprofessional), with one stating “He has preferred people that he likes to be around, even a para at school where he’s happy with, you get another para next to him and he’s agitated, angry” (CG12). Young adults with RASopathies noted that their own ability to cope decreased based on certain interpersonal interactions (e.g., receiving problematic advice from an acquaintance after disclosing symptoms) or increased in the presence of trusted individuals (e.g., receiving support from a parent).
Theme 3: Being different and lack of community knowledge about RASopathies
A third theme encapsulated feelings of difference and isolation, sometimes compounded by a lack of community understanding of their diagnosis. Caregivers expressed that their children “look different,” are “just different” or are “just who [they are],” but caregivers “don’t know how much [they think they’re] different” (CG01, CG02, CG04). One caregiver wondered how much their child should share with others about their diagnosis, expressing concerns that this could make them stand out. Other caregivers noted that their children visibly struggled to form friendships because they “didn’t quite fit in” (CG02). In contrast, some caregivers questioned the social construct of normalcy, concluding “there’s no such thing as being normal” (CG05) and that differences such as perceived immaturity in comparison to other children “really [don’t] matter” (RA17). In short, caregivers chose to make meaning of the perceived differences of their children with RASopathies in distinct ways that reflected varying thought processes about acceptance.
For young adults with RASopathies, the social impacts of their medical or mental health conditions were often a concern. Several participants mentioned experiencing feelings of isolation during their K-12 school years or perceiving that they didn’t fit in with peers. They reported awkwardness arising from missing school activities due to medical appointments or having a diagnosis that placed them outside of the perceived norm. One young adult shared, “I was experiencing ‘Hey, I’m different from everyone else that’s my age’ and that doesn’t feel great.” (YA11).
Caregivers, but not young adults, reported that the community’s lack of knowledge about RASopathies impacted the way individuals were perceived. They expressed feeling unsure at times how to explain their child’s RASopathy to others, especially when there were few outward manifestations of their condition. Caregivers noted that many in their community did not know about the existence of RASopathies, unlike other conditions, which have campaigns about them. They described difficulties transitioning children from interacting with family members who understood them to others in the broader community or at school. This shift could be particularly challenging in the school setting when staff did not know how to support their child’s neurodevelopmental needs due to a lack of experience with RASopathies. Caregivers shared a perceived need to advocate for their children both in terms of school supports and to raise awareness in the larger community.
Theme 4: Suggested treatments or supports to improve care
Future supports were defined broadly as suggested but not currently utilized treatments or assistance that could impact outcomes or potentially make it easier for individuals with RASopathies to access care. A key suggestion from study participants was to increase the training and professional development of clinicians. Caregivers recommended increased training pertaining to how neurodevelopmental concerns present in children with rare diseases like RASopathies. One caregiver contemplated questions that had arisen as she navigated providers: “Can’t you get us into mental health professionals who understand this condition? Can’t there be someone in the team in that hospital . . . that are specialists in this?” (CG17). Young adults mentioned the need for trauma-informed care, especially to address experiences of medical trauma: “A lot of people, like therapy-wise, don’t understand that just because I’m alive and well, doesn’t mean that all the things that have happened to me in my life weren’t difficult, and I still struggle with processing them now” (YA01). They also voiced the potential benefit of more provider training in working with individuals with complex medical and neurobehavioral needs, including individuals who are minimally verbal.
The need for future research to identify effective treatments was also frequently mentioned. For young adults, comments primarily centered on the need for improved pharmacological or biological treatment strategies for RASopathies (e.g., investigation of the utility of transcranial magnetic stimulation in treating ADHD). Caregivers saw a potential benefit for additional social supports, such as a peer group focused on skills development, but also expressed uncertainty about whether their children would be interested in joining a group. As such, caregivers emphasized the need for increasing the self-confidence and autonomy of children and teens with RASopathies to allow them to make their own choices about what would benefit them as they are developmentally able to do so. Additionally, they suggested that researchers could establish a database of resources about the effectiveness of different neurodevelopmental and mental health treatments for children with RASopathies. An integrated summary of critical needs to advance care and support of RASopathies families is provided in Table 3.
Crucial needs for advancing neurodevelopmental and mental health care in RASopathies.

Discussion
Mental health and behavioral challenges are known to contribute to reduced quality of life among individuals with RASopathies, as well as increased stress among their caregivers.45,56,57 The development of effective treatments to address these concerns has been identified as an urgent priority at recent international RASopathy symposia.58,59 The goal of the current study was to gain insight into how individuals with RASopathies and their caregivers view their symptoms, utilize available treatments, and perceive experiences related to mental health care. Congruent with other published research, both cohorts expressed that RASopathies are often accompanied by challenges related to attention/executive functioning, mood, and social function.15,45,58 Notably, anxiety also emerged as a frequently expressed mental health concern among study participants. Coupled with recent research identifying a heightened risk for anxiety among youth with RASopathies who were assessed with diagnostic interviews,17,60 the finding that anxiety was a topic of considerable discussion among study participants suggests that it could be a more significant comorbidity than previously understood and an area of clinical priority within the RASopathies patient community. Sleep problems and sensory needs were also key concerns mentioned by participants, despite fairly limited focused research on these topics.60,61
Participants described how their concerns were complex in their expression (shifting across time, setting, and person). This finding underscores the importance of monitoring symptom burden across relevant contexts (e.g., at home, in the classroom) when forming diagnostic impressions and assessing treatment response. Further, mental health concerns often interfere with participants’ physical health. These connections between mental and physical health burdens highlight the value of multidisciplinary perspectives in addressing RASopathy complications like chronic pain, sleep problems, and feeding difficulties.62–64 Results also suggest that “diagnostic overshadowing” may occur in RASopathies, whereby mental health or behavior problems are overlooked in the face of more apparent physical health symptoms. This conceptualization aligns with multiple studies reporting that neurodevelopmental conditions like ADHD and ASD are diagnosed less frequently among youth with RASopathies than would be expected based on assessments administered for research.12,13,65 Importantly, several young adults in the current study voiced frustration at not having their mental health concerns recognized or taken seriously, alluding to the importance of including behavioral health experts within multidisciplinary care teams.
Another common concern of study participants involved a lack of understanding and acceptance from those surrounding them (e.g., educators, community members). These results signal a need for support measures focused on increasing education about RASopathies and fostering inclusivity and belonging. Relatedly, participants frequently described providers’ lack of experience or knowledge as a barrier to care, an experience identified in previous research assessing perspectives of families affected by Noonan syndrome. 57 Unfortunately, these trends are not unique to RASopathies but instead are reflected in the larger rare disease community.66,67 Our findings underscore the importance of robust advocacy and family support organizations, awareness campaigns, and increased training and education for healthcare professionals (further elaboration of these needs is provided in Table 3). Research demonstrating that attending RASopathies family support conferences is associated with reduced stress among parents 42 further supports the conclusion that disease-related education and family connections can enhance well-being. The impact of such conferences and gatherings on the experiences of youth with RASopathies should be further explored.
In terms of the current treatment landscape described by study participants, a wide variety of approaches to address neurodevelopmental concerns were shared, including both standard pharmacological and therapy-based treatments as well as family and individual coping strategies. Although assessing the utility of these currently available treatments was beyond the scope of the current study, the significant variability that participants described in their treatment experiences (e.g., perceived efficacy, accessibility, and occurrence of adverse effects) confirms the need for tailored approaches. Relatedly, recognition of how patient selection and differences in symptom burden within and across each RASopathy may impact the results and efficacy of clinical trials is a critical consideration for investigators.68,69
Our study also highlights the need for removing barriers to treatments and making them accessible across a range of geographical regions and income levels, as well as across a spectrum of disability. Notably, several young adults in our study voiced the experience that mental health concerns emerged or intensified during the time of transition to adulthood. This finding parallels studies reporting high levels of concern among caregivers of individuals with RASopathies when contemplating their child’s future, the long-term impact of their condition, and whether social services will be available to meet their care needs.44,45,70 To mitigate stress during this vulnerable time, roadmaps and programming to ensure a planned and purposeful healthcare transition when transferring from child- to adult-centered care systems would be of great value. 71
Several differences between young adult and caregiver perspectives were identified. For example, whereas caregivers often describe concerns regarding developmental delays, anger or conduct problems, and autistic symptoms, these concerns were rarely reported by young adults. This discrepancy could be due in part to differences in the age range represented, or to the fact that young adults with RASopathies with more pervasive neurodevelopmental and behavioral challenges may have been less able or willing to participate in our study. As has been described in previous studies, this finding could also indicate a tendency for youth with RASopathies to underreport these symptoms or, conversely, for caregivers to overreport them.18,72
Another difference in the perspectives expressed was that caregivers often mentioned the importance of family support, whereas young adults tended to emphasize individual coping strategies. Emerging research provides evidence in favor of both family-based and individual skill-building approaches to enhance patient functioning. In terms of family-based approaches, a recent pilot of a psychologist-led acceptance and commitment therapy program for parents of children with RASopathies achieved high feasibility, strong engagement, and positive participant feedback. 73 A similar study focusing on parent management training for parents of children with NS found that after engaging in the intervention, mothers reported a decrease in parent-child dysfunctional interactions, along with an overall decrease in parenting stress. 45 Complementing these interventions designed for caregivers, supports to enhance individual coping among youth with RASopathies are also critically important. Providing tools and strategies around socialization, emotion regulation, chronic pain management, and coping with medical procedures could prove to be especially beneficial.38,57,74 Further, the varying perspectives of caregivers and young adults suggest that fostering communication among family members about their respective concerns, perceptions, and goals could be valuable in identifying effective support strategies.
Limitations
This study contained several limitations. First, the amount of time each participant spoke varied, leading to a greater representation of the views of some focus group and interview participants. Further, the structure of the focus group and interview questions, which requested information about a range of concerns (such as anxiety, mood, and attention), necessitated follow-up prompts to encourage participants to elaborate on their responses. There was also a tendency for focus group participants to agree, potentially due to conformity and biases regarding social acceptability. While the dependability of data was likely minimally affected by these limitations (which are common in qualitative research), additional structure, balanced speaking time protocols, and opportunities to provide anonymous responses could enhance future studies. Interview data eliciting perspectives of young adults with CS were not available for analysis. Although enrollment was attempted with multiple participants, the videoconferencing format was challenging due to the need for verbal communication and ensuing anxiety. Future studies could design interview structures that better adapt to the needs of individuals with CS and CFC, such as having the interviewer be a familiar person, offering alternative response modalities, and limiting the use of open-ended questions. 75
Symptom overlap across specific mental health diagnoses occasionally made it difficult to assign the most appropriate code to every utterance (for instance, depressed or unstable mood and anger were coded separately, even though they can intersect). This limitation underscores the need for more focused studies on how mental health conditions manifest in RASopathies. Regarding perspectives on currently available treatments for individuals with RASopathies, conclusions about the potential efficacy of such treatments were not possible within this qualitative study. Both retrospective and prospective controlled studies using patient-reported outcomes could enhance knowledge regarding promising treatment avenues. We did not collect information from the participating caregivers regarding their own health history and whether they were diagnosed with a RASopathy; it is possible that caregivers who have a RASopathy themselves could have distinct perspectives as compared with those with children carrying de novo variants. Finally, interpretations regarding cross-syndrome differences were challenging due to small sample sizes for each individual diagnosis; future studies using survey-based methodologies or multinational recruitment could potentially reach larger cohorts.
Conclusion
This study identified a set of actionable items to inform research and practice that reflect the expressed needs and lived experiences of both patients with RASopathies and their caregivers (Table 3). Our results illuminate the barriers and facilitators that families frequently encounter, offering insights that can drive improvements in care access and elevate care standards. The findings also gesture toward critical future research directions. As the importance of patient-centered outcomes research is increasingly recognized, strong partnerships with patient communities will enhance the relevance and impact of treatment research in RASopathies and other underrepresented conditions.
Supplemental Material
sj-docx-1-trd-10.1177_26330040261427019 – Supplemental material for Patient and caregiver perspectives on neurodevelopmental and mental health care for RASopathies
Supplemental material, sj-docx-1-trd-10.1177_26330040261427019 for Patient and caregiver perspectives on neurodevelopmental and mental health care for RASopathies by Evelyn M. Elizondo, Anne M. Floyd, Allison M. H. Foy, Dante J. Rogers, Betül Çakır-Dilek, Megan Manternach, Jessica Simacek, Rebekah L. Hudock and Elizabeth I. Pierpont in Therapeutic Advances in Rare Disease
Supplemental Material
sj-docx-2-trd-10.1177_26330040261427019 – Supplemental material for Patient and caregiver perspectives on neurodevelopmental and mental health care for RASopathies
Supplemental material, sj-docx-2-trd-10.1177_26330040261427019 for Patient and caregiver perspectives on neurodevelopmental and mental health care for RASopathies by Evelyn M. Elizondo, Anne M. Floyd, Allison M. H. Foy, Dante J. Rogers, Betül Çakır-Dilek, Megan Manternach, Jessica Simacek, Rebekah L. Hudock and Elizabeth I. Pierpont in Therapeutic Advances in Rare Disease
Footnotes
Acknowledgements
We are greatly appreciative of RASopathy patient advocacy groups for their assistance with recruitment and wish to thank the individuals with RASopathies and caregivers who generously contributed to this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.