
Abstract
Background:
Gaucher’s disease (GD), a rare lysosomal storage disorder, primarily affects haematopoietic tissue. Emerging evidence suggests that GD also has an impact on gynaecological well-being, with documented pregnancy-related complications. However, substantial evidence is still lacking, indicating the need for better surveillance of GD-associated gynaecological complications.
Objectives:
To assess the frequency of gynaecological ailments, pregnancies and pregnancy-related complications and outcomes in women diagnosed with GD in Central and Southeastern Europe.
Design:
An online questionnaire was developed to gather data on gynaecological and reproductive health among female patients aged 18 years or older from five countries (Croatia, Slovenia, Serbia, Northern Macedonia, Bosnia and Herzegovina). The questionnaire was translated to native language of participating countries and distributed by the Croatian Gaucher Association. The study was conducted from December 2021 to March 2022.
Methods:
The variables assessed were treatment type, age at diagnosis, reproductive history, frequency of haematological disorders, infertility issues and pregnancy outcomes, as well as comparison of these variables between treated and untreated patients. Descriptive statistics were employed to calculate proportions, and mean values were computed for continuous variables. Fisher’s exact test was used to compare categorical variables.
Results:
The study involved 26 participants. At the time of the study, four of the participants were undergoing substrate reduction therapy (SRT), and the remainder were receiving enzyme replacement therapy (ERT). Patients who received treatment during pregnancy reported a higher frequency of pregnancy-associated bleeding (71.3% vs 22.2%, p = 0.030). In total, there were 25 pregnancies and 20 births reported, while 11 (42.3%) respondents did not have children. All women conceived naturally, yet three reported difficulties with conception. Women who reported bleeding during pregnancy were more likely to experience issues with conception (p = 0.036) and bleeding during childbirth (p = 0.018). However, no significant difference was observed in relation to bleeding prior to pregnancy (p = 0.529).
Conclusion:
GD does not hinder pregnancy or motherhood, nor does it affect fertility, although it does require proper medical oversight and care. ERT alone may not be sufficient to prevent bleeding events, and detailed studies concerning coagulation might be necessary in pregnant women with GD.
Plain language summary
The study aimed to investigate the impact of Gaucher’s disease (GD), a rare genetic disorder, on gynecological health and pregnancy outcomes. It involved 26 patients diagnosed with GD from five European countries. The study examined the incidence of gynecological complaints and pregnancy-related complications, including irregular bleeding, spontaneous abortions and peripartal complications. While a higher proportion of patients experienced irregularities in their menstrual cycles, only a few faced difficulties in conceiving. Among pregnant participants, conception difficulties were associated with bleeding during pregnancy and childbirth. Interestingly, patients undergoing treatment reported bleeding during pregnancy more frequently compared to untreated patients. Despite these challenges, most participants conceived naturally, with relatively few complications during pregnancy and childbirth. However, some individuals who were not pregnant expressed concerns about pregnancy due to their disease. Overall, the research provides important insights into managing pregnancy in GD patients, indicating favorable pregnancy outcomes in most cases. Nonetheless, the relatively small sample size and lack of genetic information limit the ability to draw unequivocal conclusions. Therefore, careful monitoring and medical care should be ensured.
Introduction
Due to the small number of patients and atypical clinical manifestations, rare diseases, including Gaucher’s disease (GD) represent a challenge in everyday clinical practice. Gynaecological and reproductive health in the context of GD and other accumulation diseases is often controversial, without definite guidelines and evidence-based conclusions mainly due to insufficient number of studies conducted.
As a genetic disorder affecting glucocerebrosidase enzyme (GCase), disease severity is mainly attributable to its residual activity correlating with accumulation of glucoceramide in tissue macrophages and monocytes. Therefore, three types of the disease can be distinguished.1,2 Type 1, or the chronic non-neuronopathic type, is the most common form of the disease and affects about 92% of patients. It is usually diagnosed around the age of 20, since the residual activity of the enzyme is the highest. Type 1 is usually manifested as growth retardation, asthenia and/or delayed puberty, while other common findings include hepatosplenomegaly which is seen in more than 90% of patients (often as the only sign of the disease), haemorrhagic diathesis along with thrombocytopenia, as well as bone deformities and pathological fractures deriving from macrophage infiltration of bone tissue. Anaemia is present in 20%–50% of cases and is usually moderate, whilst leukopenia is rare. 1 Type 2, the acute neuronopathic form, affects 1% of diagnosed individuals. It is the rarest type, often diagnosed during infancy. Clinical features include organomegaly, muscle rigidity, convulsions and subsequent brain stem damage. If left untreated, the disease progresses and leads to death by 2 years of age. 3 Subacute neuronopathic type, often referred to as type 3, makes up to 7% of patients with GD and is characterized by progressive encephalopathy with oculomotor apraxia, epilepsy and ataxia along with the signs of type 1 disease, occurring mostly in childhood.3,4
In individuals with GD, reproductive health is often affected as well. Pubertal delay may be observed along with menorrhagia, while the duration of menstruation is typically not affected. 5 Although pubertal delay and menstrual cycle dysregulation occur in individuals with GD, the disease is not considered to cause infertility, nor has it been linked to premature delivery or congenital disabilities. 5 Worsening of thrombocytopenia and anaemia are common complications during pregnancy, while in the postpartum period, an increased risk of haemorrhage has been observed. Treatment with enzyme replacement therapy (ERT) reduces the risk of these complications and is highly encouraged during pregnancy. 6
Bleeding tendency is frequently observed in patients diagnosed with GD, and is partly caused by thrombocytopenia due to massive splenomegaly. However, higher risk of bleeding observed in the setting of normal or slightly low platelet count suggests that coagulopathy and abnormal platelet function are additional factors for haemorrhagic diathesis in these patients. 7 Hollak et al. reported parameters of coagulation in 30 type 1 GD patients (of which 14 were splenectomized) before and after treatment with ERT. After 6 and 12 months of treatment, activated partial thromboplastin time (aPTT) significantly decreased in all patients (especially in the nonsplenectomized group), whereas prothrombin time (PT) remained unchanged. Factor V, protein C and platelet count increased in the non-splenectomized group after 12 months. 8 However, other studies did not find differences in platelet count or adhesion between treated and untreated patients, nor did they observe normalization of coagulation parameters. 9 This suggests a complex interplay between coagulation factors and platelet function in haemostasis.
The surveillance of symptoms and complaints arising from rare diseases is essential for better disease management among affected individuals. In the Republic of Croatia and the neighbouring countries of southeast Europe, problems in surveillance are especially prominent, due to insufficient financial and human resources. Therefore, our study aims to clarify and determine the real impact of the disease on pregnancy, its outcomes, and the overall reproductive well-being of women.
Materials and methods
This study included women aged 18 and older who were diagnosed with GD from the Republic of Croatia, the Republic of Slovenia, the Republic of Serbia, Bosnia and Herzegovina and the Republic of North Macedonia. A total of 26 participants from Central and Southeastern Europe were enrolled in this study. We collected data from all women over the age of 18 who were diagnosed with GD from the specified countries. All participants were presented with informed consent, and all of them agreed to participate in the study. The questionnaire was used with the permission of the author of the previous research with similar topic and expanded to suit the current study’s specific objectives. 10 Patients in Croatia were identified and contacted through the Hospital Information System of the University Hospital Center Zagreb, where they receive treatment and do follow-ups. Patients from other countries were contacted through the Croatian Gaucher Association.
This study is a descriptive research study with the aim to evaluate the frequency of irregular menstrual bleeding, dysmenorrhea, conception issues and haematopoietic abnormalities potentially affecting pregnancy and labour (i.e. anaemia and thrombocytopenia), as well as intrapartum and peripartum complications (including spontaneous abortion, premature birth, postpartum complications and bleeding complications), the psychological impact of GD on pregnancy and motherhood, and the influence of therapy during and after pregnancy. We employed a 49-item questionnaire (provided as Supplemental File) which was translated into the native language of participating countries to ensure it was understandable to the respondents.
Statistical analysis
Descriptive statistical methods were employed for both continuous and categorical variables. Given the small sample size and low observation count (N < 50), Fisher’s exact test was utilized for comparisons. To assess the power of our study findings, a post-hoc power analysis was performed using Cohen’s w, calculated for significant p-values of Fisher’s exact test. The association between problems with conceiving and bleeding during pregnancy had a power of 0.69, with Cohen’s w of 0.62. Post-hoc power analysis revealed higher test power when comparing bleeding during childbirth and conceiving problems (0.81, with Cohen’s w of 0.71). Statistical analysis was performed using the R programming language v.4.1.1. The significance level was set at p < 0.05.
Ethics
The study adhered to the principles of the Declaration of Helsinki and received approval from the institutional ethics committee of the University of Zagreb Medical School and University Hospital Centre Zagreb (registration number 380-59-1/1/6-22-111/113). The informed consent was enclosed at the introductory section of the questionnaire and was obtained from all participants prior to the study.
Results
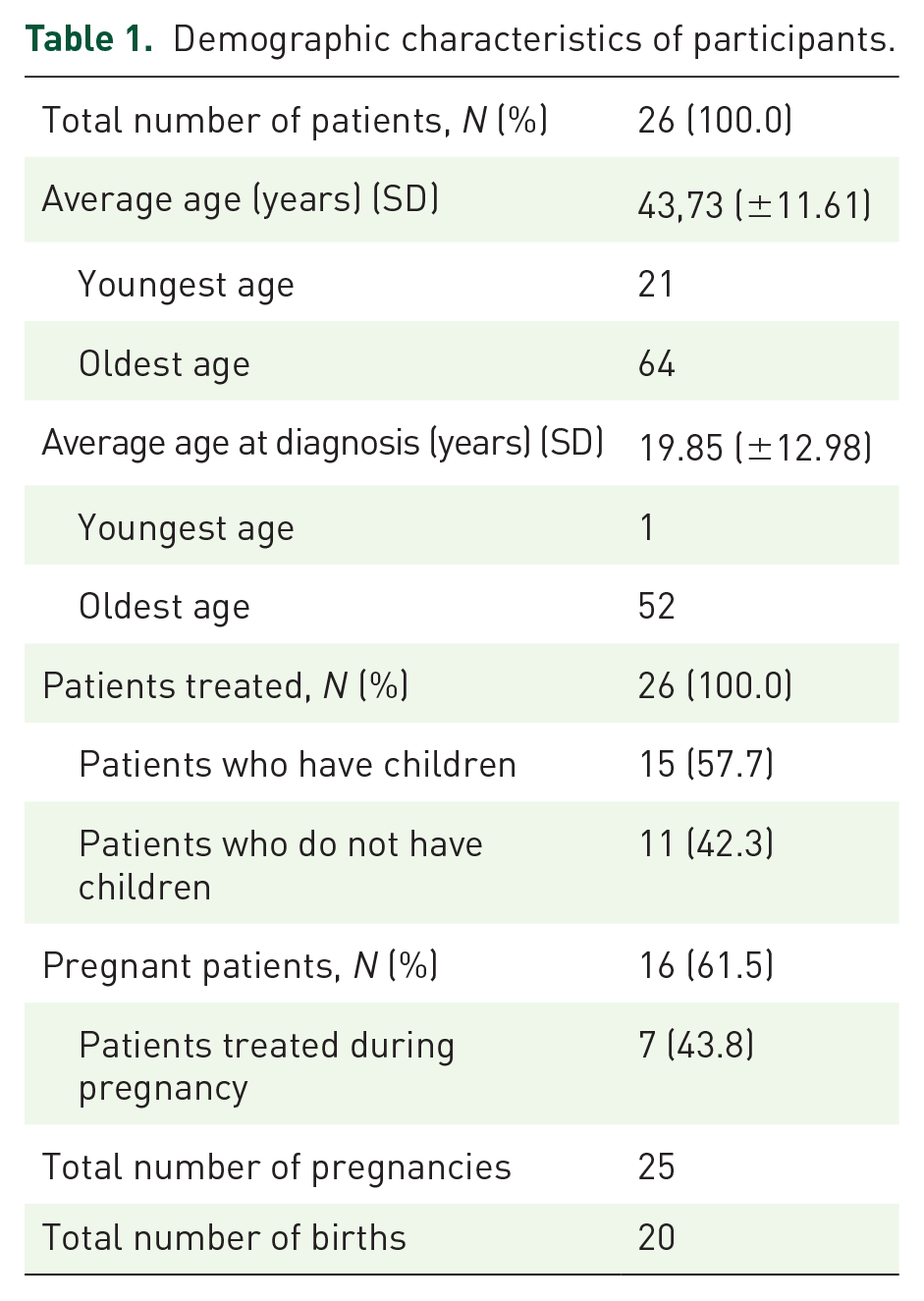
The study involved a total of 26 participants, with 11 (42.3%) from the Republic of Croatia, 6 (23.1%) from the Republic of Serbia, 6 (23.1%) from the Republic of Slovenia, 2 (7.7%) from Bosnia and Herzegovina and 1 (3.9%) from the Republic of North Macedonia. All participants were undergoing treatment at the time of the study, with 4 out of 26 (15.4%) receiving substrate reduction therapy (SRT) and the remaining individuals receiving ERT. However, during pregnancy, only 7 out of 16 (43.8%) participants were receiving treatment. The age of the participants ranged from 21 to 64 years, with an average age of 43.7. The mean age at diagnosis was 19.9 years. Demographic details are outlined in Table 1.
Demographic characteristics of participants.
The lowest reported age of menarche was 12 years, while the highest was 17 years, with an average age of 13.9 years. Among the respondents, 20 were in the childbearing age group, while the rest were in menopause. The average age of menopause was 46.5 years. Among group of women of reproductive age, 19 out of 20 (95.0%) had regular menstrual cycles on monthly basis, although 10 out of 20 (50.0%) experienced irregularities in menstrual bleeding, including longer duration and/or higher intensity, as well as bleeding occurring outside the expected menstrual period (Table 2).
Data related to respondents of childbearing age (N = 20).

Among the 26 respondents, 11 (42.3%) had no children, 10 (38.5%) had 1 child, 4 (15.4%) had 2 children and only 1 respondent (3.9%) had 3 children. A total of 25 pregnancies and 20 births were reported. A total of 16 out of 26 participants (61.5%) had been pregnant, and 15 out of 26 (57.7%) had given birth. The average age at childbirth was 26.5 years. A single twin pregnancy was reported. Three participants had discrepancies between the number of pregnancies and the number of children: one had three pregnancies but only one child, another had four pregnancies and two children, while the third had one pregnancy but no children.
Among pregnant women, 3 out of 16 (18.8%) reported difficulties with conceiving, and 2 out of 16 (12.5%) reported attempting to conceive for longer than 2 years, but ultimately succeeding. In contrast, among non-pregnant women, only 1 out of 10 (10.0%) reported attempting to conceive for over 2 years. All women conceived naturally without assisted reproductive techniques (ART). During pregnancy, 6 out of 16 (37.5%) women reported vaginal bleeding, and 2 out of 16 (12.5%) experienced spontaneous or medically indicated abortions. Notably, these women had multiple abortions each, resulting in a total of 4 abortions out of 25 pregnancies (16.0%). These abortions were evenly distributed between the first and second trimesters. Moreover, one patient, who had no children, had undergone abortion on own request. Therefore, there were five abortions in total.
Out of 26 participants, 8 (30.8%) were anaemic, and 5 out of 16 (31.3%) experienced aggravation of anaemia during pregnancy. Among pregnant women, 12 (75.0%) reported pre-existing issues with bleeding cessation and/or thrombocytopenia, with 4 out of 12 (33.3%) experiencing exacerbation of thrombocytopenia during pregnancy. One participant was uncertain about bleeding during pregnancy and was excluded from analysis. Out of the remaining, 5 (33.3%) reported bleeding problems during childbirth, with 3 out of 15 (20.0%) requiring erythrocyte transfusion and 4 out of 15 (26.7%) needing platelet transfusion. Out of the 20 deliveries, 4 (20.0%) erythrocyte transfusions and 5 (25.0%) thrombocyte transfusions were required after deliveries.
In addition to transfusion requirements, several other complications were reported. One woman experienced postpartum vaginal bleeding lasting for 3 months without requiring transfusions. A breech foetal position was observed in one pregnancy, which cannot be clearly linked to GD. Although three premature births were reported, two occurred in women with twin pregnancy, making a direct link to GD less certain. Among the three premature newborns, two had length less than 45 cm and weighed under 2500 g. Furthermore, one newborn weighed less than 2500 g, but had normal length. Two newborns exhibited low thrombocyte counts at birth. No deaths were reported. A single delivery occurred after the 42nd week of pregnancy. Additionally, 6 out of 20 (30.0%) deliveries were performed via caesarean section. Pregnancy-related data are presented in Table 3.
Data related to respondents who were pregnant.

N = 15.
When comparing treated and untreated subjects, no significant differences were found in the need for transfusions or the exacerbation of anaemia or thrombocytopenia during pregnancy. Intrapartum bleeding did not differ significantly either (p = 0.596). Surprisingly, treated patients reported bleeding during pregnancy more often when compared to untreated patients (71.4% vs 22.2%, p = 0.030).
Furthermore, among those receiving ERT, 5 (23.8%) were anaemic, 16 did not have anaemia, whereas one patient did not know if she was anaemic. Among those treated with SRT, three out of four (75.0%) were anaemic. Although anaemia was less likely to occur among patients treated with ERT, we did not find it to be significantly different (p = 0.081). Moreover, we did not observe any differences between menorrhagia among those receiving ERT and SRT (p = 0.474).
Among fertile women, no differences were noted in bleeding during pregnancy (p = 1.000), intrapartum bleeding (p = 1.000), incidence of anaemia (p = 0.546) or thrombocytopenia (p = 0.491) in relation to dysmenorrhea. Women in menopause were excluded from this analysis due to potential recall bias regarding menstrual complaints.
Subsequently, we wanted to assess if bleeding, anaemia or low thrombocyte count were linked to difficulties conceiving. Among pregnant women, three who reported difficulties conceiving also experienced issues with vaginal bleeding during pregnancy and childbirth. Notably, all three suffered from anaemia and thrombocytopenia before becoming pregnant. Accordingly, bleeding during pregnancy (p = 0.036) and bleeding during childbirth (p = 0.018) were linked to conceiving problems. Interestingly, no significant differences were found regarding bleeding before pregnancy (p = 0.529). Anaemia (p = 0.063) and thrombocytopenia (p = 0.529) were not associated with difficulties conceiving.
Lastly, among the women who did not have children, 4 out of 10 (40.0%) attributed their failure to achieve pregnancy, childbirth and motherhood to the fear induced by the diagnosis of GD.
Discussion
Gynaecological well-being is still a controversial topic among women suffering GD, despite advances in therapy and pregnancy care. While most studies report adverse gynaecologic and obstetric outcomes in a smaller percentage, more severe complications, such as antepartum bone crisis, have also been noted, suggesting that the disease burden may be underestimated. 11 Estimation of disease symptoms is further complicated by the fact that some women are not being diagnosed before pregnancy. In our study, four women (25.0%) were not diagnosed during their pregnancy, but rather later in life clearly implying that GD was not a setback for motherhood. Among those, two had difficulties stopping the bleeding even before being pregnant, while two had worsening of anaemia during pregnancy and one had postpartum bleeding requiring erythrocyte transfusions. Granovski-Grisaru et al. reported a similar percentage (27.7%) of women being diagnosed during their first pregnancy, which could be the consequence of disease aggravation during pregnancy. 6
Although diagnostic and therapeutic approaches evolved, GD still remains a diagnostic challenge, among both pregnant and non-pregnant individuals, mainly due to the wide range of symptomatology, ranging from asymptomatic disease to more severe manifestations. Reported median time from symptoms onset to diagnosis varies and greatly depends on disease type. The oldest age at diagnosis in our sample was 52, and the youngest was only 1 year, with the average age being 19.85 years. A significant age range at the time of diagnosis probably speaks in favour of the broad symptomatology of GD. In a smaller cohort of 86 patients, time to diagnosis was 2 years, ranging from half a year to 26 years. Moreover, no significant difference in establishing diagnosis was observed after introducing specialist care. 12 Comparing the mean age at diagnosis of GD with other available multinational and national registries, the sample of this study shows a lower mean age at diagnosis. According to the French registry of patients with GD, the average age at diagnosis is 22 years. 13 However, for individuals affected with type 1 GD, the diagnosis is often established in middle age, usually in the fifth decade. 14 As reported by International Collaboration Gaucher Group (ICGG), which consists predominantly of patients from the United States and Israel, reported mean age at diagnosis is 27.2 ± 19.7 years for the N370S homozygous genotype. The age at diagnosis for the homozygous L444P genotype was significantly lower, 2.3 ± 3.2 years. 15 The Gaucher Outcome Survey, which included 1209 patients, indicates a dependence between the age at diagnosis and the disease type, whereby the oldest average age at diagnosis (40.4 years) is observed in people suffering from GD type 1, and the youngest in those suffering from GD type 2 (2.5 months), or type 3 (3.2 years). 16 The same reason could likely explain the youngest and the oldest age as well as the wide range of ages at diagnosis in our sample. However, our conclusions are presumptive since we did not have insight into the genetic background of the participants’ disease.
Impact of GD on menstrual history has not been thoroughly explored, but evidence suggesting alterations in menstrual bleeding exists in the literature. Overall, menorrhagia occurs more frequently among GD affected women. 10 In a small study of seven Jewish women, three of them reported menorrhagia, while one had a short period of amenorrhea. However, two of the patients reporting menorrhagia conceived successfully. 17 Among menstruating patients in the study by Granovsky-Grisaru, heavy menstrual bleeding was noted among 22 out of 52 (42.3%) patients. Moreover, heavy bleeding was more frequent among those exhibiting mild and moderate disease severity (10 in each group, compared to 2 among women with severe disease). 11 In our sample, among menstruating participants (20 in total), half of them experienced menorrhagia, while only one participant reported not having regular menstrual bleeding.
According to Croatian Scientific and Statistical Yearbook 2023, published by Croatian Institute for Public Health (CIPH), among 516,580 healthy women included in primary gynaecological healthcare outside the Croatian Health Insurance Fund network, 0.54% were diagnosed with menstrual bleeding disorders, while 0.12% experienced other forms of abnormal bleeding of the reproductive tract indicating significant disparities among healthy women and women diagnosed with GD. 18 Unfortunately, as far as we know, there are no available statistics on the incidence of abnormal uterine bleeding for neighbouring countries. Therefore, future efforts should focus on comprehensive monitoring of gynaecological symptoms prevalence in both affected individuals and the general population to better assess symptoms prevalence, improve treatment and enhance quality of life.
Haematological disorders are frequently encountered in patients suffering from GD, the most common of which are anaemia and thrombocytopenia, and less often leukopenia. 19 Quantitative disorders have a far greater importance in clinical practice because their monitoring serves as a tool for determining treatment efficacy. 20 According to the IGCC registry, 36% of patients with type 1 GD have accompanying anaemia, while 40% and 45% have mild or moderate thrombocytopenia, respectively. 15 In our study sample, the proportion of anaemic patients is comparable (30.8%). Furthermore, among women who were pregnant, reported prevalence of anaemia and thrombocytopenia was 43.8% and 75.0%, respectively. Anaemia and thrombocytopenia arise from both GD-related and non-related mechanisms, including increased sequestration of erythrocyte in the spleen, impaired haematopoiesis and blood loss due to thrombocytopenia. 21 In our study, a similar percentage of women had worsening of pre-existing thrombocytopenia and anaemia during pregnancy (Table 3), although thrombocytopenia was more commonly observed. However, only five intrapartum and one postpartum haemorrhage occurred. Other studies report unequivocal results regarding haemorrhage prevalence. Elstein et al. report a higher number of bleeding events: among untreated groups three haemorrhages took place during the intrapartum, and 53 in the postpartum period. 22 In a similar study by Granovsky-Grisaru et al. the incidence of bleeding was comparable to ours, but only among those undergoing vaginal delivery (21.3%), while, among women undergoing caesarean delivery, the prevalence was higher (77.7%). Transfusions were more frequently needed among women who underwent caesarean section. 11
The treated participants from our sample exhibited bleeding episodes more frequently compared to those untreated, while there was no significant difference in the prevalence of anaemia and thrombocytopenia between these groups. It seems that the bleeding tendency is not solely dependent on the thrombocyte count, but might also be dependent on other underlying mechanisms. Indeed, research so far suggests that ERT alone might be insufficient to effectively manage bleeding tendency, as it might be related to platelet dysfunction and coagulation factors disorders as well, which are not improved with ERT.5 –7 Therefore, detailed coagulation studies and monitoring are warranted in patients, especially when planning and during pregnancy.
In our study, all pregnant participants conceived naturally. There was 25 pregnancies and 5 abortions (of which 4 medically indicated) in total, while, among the non-pregnant participants, one tried but did not succeed in conceiving for more than 2 years. According to CIPH, infertility was reported in 0.13% of healthy women included in primary gynaecological health care, indicating that infertility does not present significant burden in patients with GD.5,18 Among 15 women with GD interviewed in Greece, 4 of them conceived using ART. However, in the same study there were overall 41 pregnancies with 56.1% resulting in live births, while the proportion of performed abortions was much higher (26.8% spontaneous, and 14.6% elective and therapeutic abortions). 23 A high proportion of abortions was also noted in our sample, with 5 out of 25 pregnancies (20.0%) being terminated by abortion (either spontaneous or medically indicated), while, according to CIPH, a much lower percentage (0.05%) of abortions was reported in 2023 among women in general population, indicating the need for proper pregnancy surveillance. 18
Our observations regarding perinatal complications and preterm delivery are in line with the current findings suggesting that GD has a minimal impact on neonatal outcomes. 5
So far only several studies have sought to evaluate the safety and impact of therapy during pregnancy in the context of GD. Isolated cases of imiglucerase treatment and successful pregnancy outcomes have been described. 24 Our study unveiled a paradoxical finding that patients under treatment reported higher rates of bleeding. This observation could potentially be explained by the severity of symptoms and differences in disease genotypes within the treated patient group. Evidence supporting this hypothesis is the significant difference in the mean age at diagnosis between the treated and untreated patient groups. The treated patients had a mean age at diagnosis of 14.7, while their untreated counterparts had a mean age at diagnosis of 23.8. This discrepancy in age at diagnosis likely stems from more severe clinical presentation in the treated patient group, which could subsequently contribute to a heightened susceptibility to complications during pregnancy. This phenomenon was also noted in the study by Elstein et al., encompassing 66 pregnancies (23 treated and 43 untreated), among which postpartum bleeding was more prevalent among enzyme-treated patients. 22 Existing evidence still indicate that the continuation of ERT during pregnancy remains a suitable course of action for patients with GD, suggesting its overall safety and potential benefits. 25 Adequate safety profile was also reported among participants treated with eliglustat, with only one spontaneous abortion which occurred in a healthy female during the first phase of clinical trial. 26
We identified four patients receiving SRT at the time of the study. Among them, two did not receive therapy during pregnancy, one never became pregnant and only one patient received therapy during pregnancy. Based on the history taken, we could not determine with certainity whether she received ERT or SRT during her pregnancy. Therefore, making straightforward conclusions on safety profile and incidence of adverse outcomes of SRT in comparison to ERT is difficult.
A noteworthy observation was that 40% of patients in our sample expressed concerns regarding possible pregnancy outcomes in the setting of GD. Therefore, comprehensive counselling and educational initiatives to provide patients with accurate and informed perspectives on reproductive health and pregnancy management should be imperative in future care planning for patients with GD.
Study limitations
While the insights gained from this study are valuable, several limitations must be acknowledged. The main obstacle of this research is the small sample size. However, it should be emphasized that this study included all women over the age of 18 who were diagnosed with GD in the Republic of Croatia, the Republic of Slovenia, the Republic of Serbia, Bosnia and Herzegovina and the Republic of North Macedonia, which makes it the only such study with data on patients with GD for southeastern Europe. This study offers valuable insights into the potential risks of pregnancy and childbirth for women with GD. However, it cannot provide precise statistical data, as a much larger patient sample is needed. Incorporating qualitative research in future studies could greatly deepen the insights and strengthen the credibility of the findings, offering a more comprehensive understanding of the topic.
One of the main limitations of this study is the inability to perform a formal power analysis and justify the sample size. This is primarily due to the rarity of GD, which significantly limits the number of available patients. Given the low prevalence of GD, our sample size was determined by the total number of female patients diagnosed with GD rather than a predefined statistical calculation. While this approach ensures that all eligible patients were included, it may limit statistical power of our findings.
Even though a portion of the questions in our questionnaire was taken from a previously used questionnaire with the author's permission, some additional questions were included to meet the objectives of the current study. 10 However, these added questions were neither validated nor pilot-tested prior to use. This should be considered when interpreting the findings.
Moreover, the study’s retrospective design without direct access to medical records raise the potential for recall bias. However, we believe the bias to be minimal due to the high level of patient awareness regarding their medical condition. Since data regarding gynaecological health are not routinely collected from the general population, making a direct comparison of the incidence of certain gynaecological symptoms between the general population and women affected with GD was not possible, except for women residing in Croatia, where these data are routinely collected by CIPH. Furthermore, some of the questions (e.g. alteration of menstrual characteristics) were answered by the patients based on their own personal experience, since it is not possible to objectify such questions.
Nevertheless, the data collected in this study contribute to a deeper comprehension and raise awareness of the complexities surrounding gynaecological health in the setting of GD, which is important for guiding clinical decision-making.
Conclusion
GD does not have impact on fertility, although difficulties with conception have been present among women diagnosed with GD. Notably, difficulties with conception emerged as a significant factor linked to the occurrence of bleeding during pregnancy and childbirth. While infertility may not be an issue, higher rates of abortions observed among women with GD drive attention to a possible impact on gynaecological health. Interestingly, our findings revealed that the treated patients experienced bleeding during pregnancy more frequently than the untreated patients, possibly due to the more severe disease form in the treated group or due to coagulation abnormalities. These observations highlight the need for more detailed coagulation studies in patients regardless of treatment received, especially during pregnancy.
The substantial number of successful pregnancies achieved and the relatively low incidence of complications during labour and the postpartum period suggest that GD should not be considered a significant hindrance to either pregnancy or motherhood. However, this research highlights the importance of proactive medical supervision in ensuring safe and healthy pregnancies for patients with GD.
Supplemental Material
sj-docx-1-trd-10.1177_26330040251335665 – Supplemental material for Navigating gynaecological challenges in Gaucher’s disease: insights from five European countries
Supplemental material, sj-docx-1-trd-10.1177_26330040251335665 for Navigating gynaecological challenges in Gaucher’s disease: insights from five European countries by Ljubas Dominik, Krstulović Opara Anđela, Wagner Jasenka and Duraković Nadira in Therapeutic Advances in Rare Disease
Footnotes
Acknowledgements
We would like to express special thanks to the Croatian Gaucher Association for technical assistance during the study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.