
Abstract

Introduction
For decades, the promise of gene therapy to ameliorate the impacts of life-limiting conditions by modifying or manipulating gene expression with a single administration has captured the public imagination in unprecedented ways. Despite historical setbacks, 1 a number of ex vivo and in vivo gene therapies are available for clinical use globally, with more than 2000 under investigation and on the road to market authorisation, predominantly targeting rare diseases. 2 In haemophilia, a once ambitious dream is finally a reality following recent regulatory approvals of three adeno-associated virus (AAV) vector-mediated gene therapies in the United States (US) and Europe: valoctocogene roxaparvovec (Roctavian®; Biomarin, San Rafael, CA, USA) for clotting factor (F)VIII (haemophilia A) 3 and etranacogene dezaparvovec (Hemgenix®; CSL Behring, Melbourne, Victoria, Australia) and fidanacogene elaparvovec (Beqvez/Durveqtix; Pfizer) for FIX (haemophilia B) which are also approved in Canada.4,5 Moreover, several other gene therapies for haemophilia based on the AAV platform and alternative gene delivery systems are in varying stages of clinical development. 6
From a United Kingdom (UK) standpoint, Hemgenix® is the first of these products to have received market authorization to date and subsequently recommended for use on the National Health Service (NHS) in England, 7 followed closely by Scotland. 8 Despite attaining licensure and entering clinic, the current consensus of first-generation AAV vector-mediated gene therapies for haemophilia (herein referred interchangeably with haemophilia gene therapy) among patient advocates, physicians and researchers alike is one of cautious consideration, noting the complexity of in vivo gene transfer and the necessity for risk mitigation strategies to ‘protect patients from potential harm’ (p. 3). 9 Anticipation of such caution has seen greater emphasis placed on the concept of shared decision-making (SDM) in supporting prospective candidates for haemophilia gene therapy to make well-informed choices based on the best available evidence, quality information and personal preferences. 10 Accordingly, in the context of implementing SDM, 11 the importance of language use and information framing when communicating the fundamental science underpinning gene therapy and its expected therapeutic effects to people living with haemophilia (PLwH) cannot be understated.12,13
Global efforts to enhance PLwH’s comprehension of gene therapy through education has been previously described, including several initiatives by patient advocacy organisations (PAGs) and resources directly branded and promoted by the pharmaceutical industry. 14 In addition, the World Federation of Hemophilia has released an inter-active, web-based SDM tool, featuring multimedia learning materials that address the key attributes and commonly asked patient questions and concerns about gene therapy. 15 Besides these regular channels of engagement, the news media constitutes an additional source of medical and scientific information that is playing an ever-increasing role in shaping patient and public awareness and attitudes towards certain disease states and biomedical innovation.16,17 However, it has been shown that the news media have a propensity to sensationalise their reportage and inflate patient expectations by emphasising the benefits whilst minimising discussions of risks and uncertainties,18,19 especially for genetics and genomic research. 20 Nonetheless, within the haemophilia literature, the news media has received surprisingly little attention as a mediator of knowledge and decision-making relating to novel treatments. We want to use this editorial to highlight the possible implications for PLwH of unchecked hype surrounding AAV vector-mediated gene therapy, drawing on our observations of reporting by popular news brands in the UK.
What is at stake?
In April 2023, soon after Hemgenix® was authorised by the UK’s Medicines and Healthcare Products Regulatory Agency, 21 the Mail Online 22 – one of the country’s biggest news brands with a monthly audience of over 18 million people 23 – posted the article, “Revolutionary gene therapy could cure thousands of haemophiliacs. . .” Upon further reading, it 22 refers to the possibility of a ‘permanent’ fix through sustained FIX levels without acknowledging the known and unknown risks, together with the limitations of AAV as a gene delivery vehicle, as has been described extensively within the literature (for a good summary see Pierce et al.). 24 This is by no means an isolated incident. Following the announcement that Hemgenix® would be made available for use on the NHS in England in June 2024, 7 the BBC 25 – generally highly regarded around the world for its science communication – ran a headline about an individual who had participated in the UK clinical trial and had by all intents been ‘cured [of his] haemophilia’. Much later in the article, it becomes clear that the individual was instead expressing a subjective ‘feeling’ of being ‘cured’, rather than scientific fact. The Telegraph, 26 who fall into the top 10 ranking of news websites in the UK, 23 published much the same story. This is not to downplay the encouraging therapeutic outcome and personal narrative of this one individual; similar ‘life-changing’ sentiments have been documented in PLwH who have undergone AAV vector-mediated gene therapy,27 –29 which should indeed be celebrated. Yet, the way the treatment has been presented as wholly ‘curative’ is potentially misleading. These inaccuracies and discrepancies are inconsistent with the scientific evidence, although it is conceivable that the news items featured above will have a greater purchase on public understandings of the therapeutic utility of haemophilia gene therapy.
From our experience, it is not uncommon for news media to make unsubstantiated claims of curative success about haemophilia gene therapy, together with overly positive patient anecdotes. Living with haemophilia ourselves, we can certainly attest to the apprehension that arises with such leading news stories; several well-wishing (mainly unaffected) friends and loved ones excitedly sharing links to the press coverage, only to be politely and cautiously reminded that it is not quite as simple and straightforward as is being portrayed. Baas et al. 30 have sought to address some of the controversy and ambiguity of the use of the term ‘cure’ pertaining to haemophilia gene therapy, suggesting that it ‘may create wrong expectations if it is not clear’ what is meant by it or ‘if [PLwH] attach a different meaning to the word than their physicians do’.
While AAV vector-mediated gene therapies for haemophilia A and B have normalized FVIII and FIX levels in some individuals, uncertainties in the long-term durability of clinical effect persist, particularly for FVIII where levels have slowly declined over time; reasons for which remain unknown. Crucially, should PLwH exhibit a suboptimal response or lose factor expression within a comparatively short period, the capacity to redose with the same AAV vector or opt for an alternative AAV serotype is limited due to host immunity and cross-reactivity, respectively. 24 Consequently, this currently restricts haemophilia gene therapy to a one-time opportunity, placing greater emphasis on SDM.9,12 –14,31 Moreover, only adult PLwH (⩾18 years of age) are eligible to receive gene therapy at present, many of whom will have pre-existing joint damage stemming from earlier bleeding that will not be restored post-administration and may continue to impact on quality of life. 31 The notion of gene therapy being unable to ‘fix the problems’ from the past and resultant disappointment has been reported to some degree among trial partcipants. 28 An additional aspect relates to the congenital nature of haemophilia; given AAV vectors are considered to be largely non-integrating into the host genome, 24 there is a low risk for germline transmission, 32 which is less problematic ethically, yet the underlying genetic defect will still be passed onto future generations. 31 Taken together, Baas et al. 30 consider it ‘desirable to refrain’ from using language such as ‘cure’ to help PLwH avoid potentially misguided interpretations of the risk–benefit profile of gene therapy, ‘especially . . . when stakeholders transcend the context in which they usually operate’; we would argue that this includes news media.
Whereas the outstanding questions relating to the clinical translation of AAV vector-mediated gene therapy for haemophilia are being raised by researchers, 24 it is highly unlikely that the nuances and distinctions of this treatment modality – at a technology platform level and versus existing alternatives – are being disseminated effectively into the wider public realm. According to Smedinga et al., 33 consumer interpretation of potentially misleading framings that make certain aspects of a drug or disease state more salient than others, ‘may trigger different emotional and behavioural responses’ with significant influence on subsequent decision-making. Considering the unique risk–benefit trade-off of haemophilia gene therapy, most notably its irreversible state (i.e., once administered, there is no going back!), 9 fostering safe, accurate and socially responsible communication around the technology is becoming ever more vital as these products are added to the therapeutic armamentarium and where PLwH’s rights, interests and autonomy to make evidence-informed choices are prioritised.12,30
Another reason to promote public vigilance to press coverage concerning haemophilia gene therapy and individuals’ options can be drawn from the work of Disability Studies scholars, 16 who have highlighted how representations of medical advances in news media can frequently employ language that frames disabled persons as ‘having an inherent problem needing to be cured or fixed by medical intervention’. The issue being that this rhetoric could misinform prospective parents about living well with a disability and have far-reaching implications for families, such as termination of pregnancy, financial and time costs, perceived burden on the state, among others. Furthermore, if there is a widely held misperception that a health condition has been ‘cured’, one might imagine both public and political sympathy and endorsement for the patient community to wane, particularly in relation to: charitable and research donations, support with daily living, care and accessibility requirements as well as social welfare entitlement (the latter a system in the UK that already has stringent conditionality rules and a kind of ‘epistemic sabotage’ in the evidential standards governing eligibility of claimants 34 ).
Van Balen et al. 35 have also documented how ‘the societal financial burden of current haemophilia treatment’ weighs heavily on the conscience of some PLwH, which they attribute to ‘recent media attention surrounding health technology assessments, pricing and reimbursement decisions for expensive drugs’. The apparent high cost of gene therapy seems to be a recurring negative theme when evaluating PLwH’s treatment preferences and choices across different countries,36–38 including the UK. 39 When it comes to the economics of gene therapy, as Goodman et al. 40 explain, ‘[r]ather than being spread over years or decades as is usual for managing chronic conditions, the cost of gene therapy is concentrated into a single administration’, meaning manufacturers/innovators can command a steep ‘list’ price. From a single-payer perspective, this significant upfront outlay results in high so-called ‘budget impact’ and subsequent opportunity costs (i.e. displacing more health benefits than are generated). 41 Therefore, to manage both the clinical uncertainties and financial challenges associated with haemophilia gene therapy, alternative payment models based on risk-sharing arrangements are being applied to facilitate patient access while ensuring good value for the healthcare system, 40 with a typically lower ‘net’ price paid determined through confidential commercial negotiations 42 ; as is seemingly the case with Hemgenix®.7,8
Despite this evolution in reimbursement solutions, news media have been quick to exploit the prevailing concerns over affordability of new technologies like gene therapy within the NHS, 43 not least by readily referring to the product list price,25,26 including such eye-grabbing headlines as ‘NHS watchdog approves ‘world’s most expensive drug’ that costs £2.6million a dose. . .’. 44 In our view, this unfortunately poses a greater chance of exacerbating feelings of shame or guilt as PLwH contemplate their options. The efficiency-equity dilemma – essentially, balancing the control of rising drug expenditure with the promotion of innovation 43 – could further fuel resentment between different health service user groups, where there is a perceived disadvantage in the distribution of scarce resources. As Shakespeare 45 alluded to more than a quarter of a century ago, yet still highly relevant today, simplistic and one-sided framings of budgetary impact only serve to propagate reductive conceptions of smaller populations affected by less-common conditions and/or those living with disabilities as an ‘unnecessary social cost’. These sorts of discourse will inevitably be noticed and felt by PLwH and are likely to have an impact on how individuals navigate their treatment journey. For this reason, there is a need to think much more critically about actively deconstructing news media narratives in the present paradigm of haemophilia gene therapy.
‘Bursting’ the media hype bubble
Corresponding with the introduction of new country-specific clinical guidelines in this space, 46 it is our hope that key stakeholder groups facilitating patient learning can seek to adopt a proactive stance in countering haemophilia gene therapy-related misinformation (Figure 1). We strongly recommend that healthcare professionals (HCPs) be more cognisant of the ways in which news media has the power to shape community expectations and support their patients in interpreting press coverage, ensuring open and transparent two-way dialogue to help close treatment knowledge gaps and reduce the spread of inaccuracies. Likewise, we would encourage PAGs to combine their programmatic endeavours in promoting haemophilia gene therapy literacy with media literacy competencies as a preventative measure for members to ‘read between the lines’ of news media portrayals of genomic science. Lastly, we appeal to gene therapy innovators and partnering institutions to be mindful of avoiding making claims that compromise scientific integrity, particularly in company press releases.
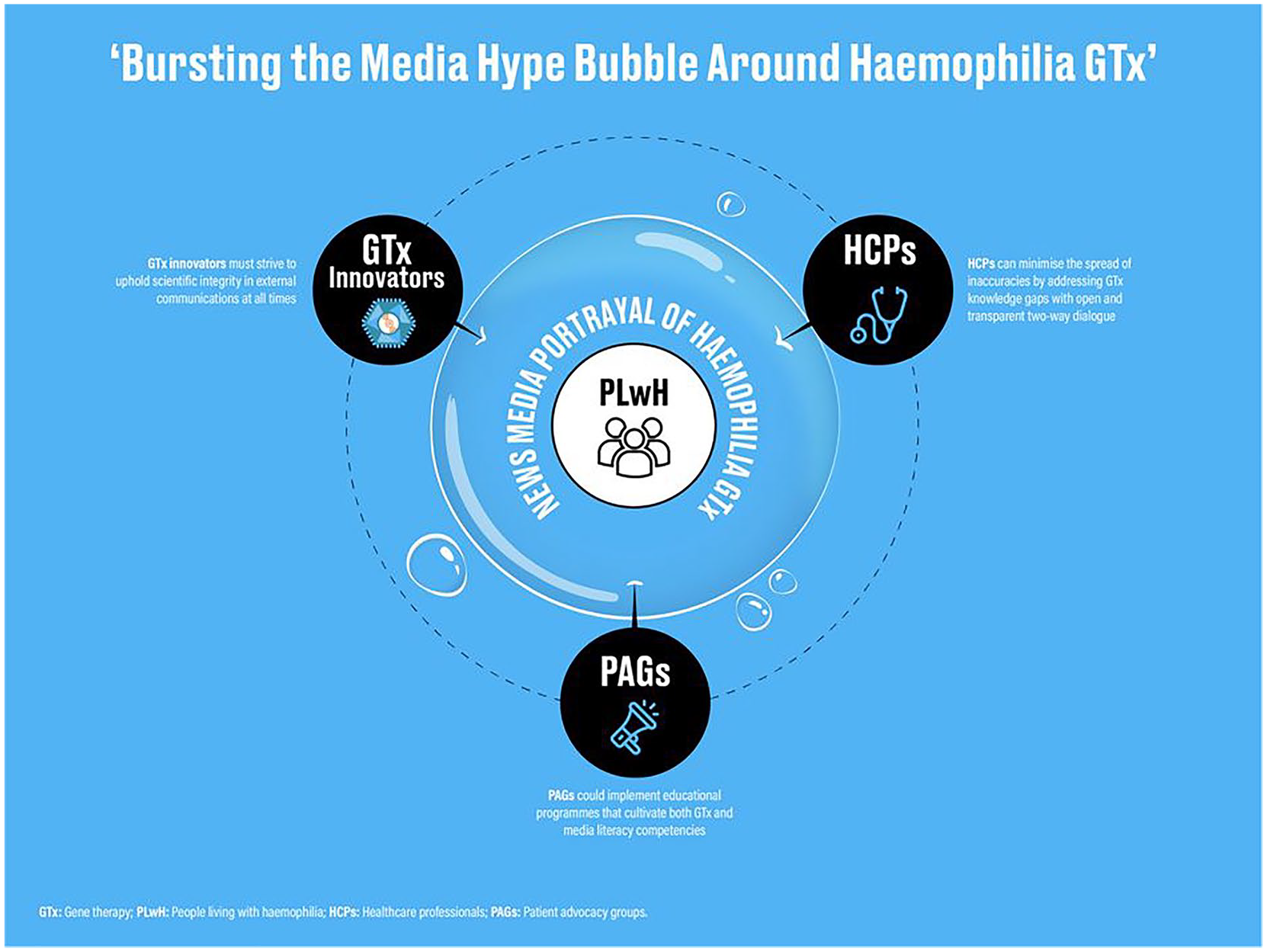
People Living with Haemophilia may find themselves caught up in a gene therapy hype bubble inflated by news media, necessitating the efforts of relevant stakeholders to mitigate the potentially harmful effects of disinformation and proactively manage their expectations.
As noted earlier in this manuscript, there exist challenges associated with the language of ‘cure’ for current first-generation AAV-based gene addition strategies for treating PLwH. We have outlined some of the reasons as to why continued use of this phraseology in news media could be problematic, with unintended consequences on patient care and wider societal ramifications. Like others, 30 we are sceptical about the value of this term without adequate context or explanation, alongside expectation management. Herein lies a tension between ensuring community expectations of haemophilia gene therapy are realistic, while on the other hand, recognising the ambition and generative power of ‘curative’ language in, say, attracting funding and support for research. Power et al. 47 have expressed the equivalence in terms of HIV treatment; balancing the need to maintain scientific, public and political energy and interest on the ‘longer-term goal of achieving elimination of [the virus] from the body’ while also tempering expectations among affected individuals through faithful representation of the ‘shorter-term research outcomes’. While there is no obvious alternative to the use of the term ‘cure’, in the gene therapy arena, several authors12,48,49 across multiple disease areas have stressed the major role of patient education to reduce potential therapeutic misestimation in order for individuals and their families to make an informed and measured judgement as part of SDM.
SDM is frequently presented as a neat dyadic relationship between HCPs and PLwH. By casting a spotlight on the potential for news media’s influence in and outside of the clinic, we hope our editorial draws attention to the considerable complexity of messaging as well as both the health system and societal pressures acting upon PLwH when it comes to decision-making about gene therapy. We propose this subject area be given greater attention within scientific literature and practice, with further research that goes beyond our limited critique to encompass a more internationally representative and methodologically rigorous content analysis of articles published by news media about haemophilia gene therapy. Efforts to capitalise on a promising new era of treatment management in haemophilia should not be at the detriment of PLwH; equitable decision-making relies on sound scientific information and realistic discussions of knowns, unknowns and uncertainties to minimise possible future regrets, whether choosing AAV vector-mediated gene therapy or not.