
Abstract
Sanfilippo syndrome (Mucopolysaccharidosis Type III or MPS III) is a family of rare, lysosomal disorders characterized by progressive cognitive and motor deterioration. Even though individuals with MPS III present with complex communication needs, research regarding augmentative and alternative communication (AAC) in this population is scarce. While life expectancy for individuals with MPS IIIA typically does not exceed 20 years of age, this case report involves a 22-year-old adult with postregression MPS IIIA. Prior to this study, the participant could not communicate using speech and only responded to yes/no questions using eye blink responses. The participant was given a low-tech AAC system utilizing eye gaze so that she could respond to a variety of caregiver questions and take conversational turns. The following communication outcomes were measured during each session in which caregivers used the AAC system: number of eye gaze responses, total number of responses (using any means), the percent of responses to questions asked, and the total count of expressive vocabulary words available to the participant with the AAC system. Increases were observed in the number of eye gaze responses per session and in the expressive vocabulary accessible via the eye gaze board. A higher percentage of responses given caregiver questions was noted for the intervention sessions (71%) compared to the baseline sessions (55%). There were also qualitative changes characterized by the types of questions the participant could respond to during conversational exchanges. Despite the progression of MPS IIIA, the results suggest that use of the eye gaze board resulted in quantitative and qualitative changes in functional communication. This case report provides preliminary evidence that AAC can improve communication in a young adult with postregression MPS IIIA.
Plain language summary
This article reports a case of a 22-year-old woman who was diagnosed with mucopolysaccharidosis type III (MPS III) or Sanfilippo Syndrome. MPS III is a rare lysosomal disorder characterized by progressive cognitive and motor deterioration. Children with MPS III experience regression in speech and communication skills and speech is typically lost by age eight years. AAC (Augmentative and Alternative Communication) are systems or devices that can be used by individuals with limited to no speech to aid or supplement communication. Even though individuals with MPS III have significant impairment in communication and could potentially benefit from AAC, research regarding the use of AAC (Augmentative and Alternative Communication) by this population is scarce. In this case, an eye-gaze AAC system was introduced to a young adult with postregression MPS IIIA who is well beyond average life expectancy for this disease. Despite the progression of MPS IIIA and complicating medical issues, there were quantitative and qualitative changes and improvement in this woman’s functional communication after the eye gaze board was introduced. This case study provides preliminary evidence that AAC use can potentially improve communication in individuals with postregression MPS IIIA.
Keywords
Introduction
Mucopolysaccharidosis (MPS) III (or Sanfilippo syndrome) is a rare recessive metabolic lysosomal storage disease that causes progressive childhood dementia, loss of natural speech, and complex communication needs (CCN). Augmentative and Alternative Communication (AAC) provides a way for individuals with CCN, including those who cannot use natural speech to communicate and participate in all aspects of life.1,2 AAC includes a wide range of methods and systems that use symbols, pictures, and words, and include aided and unaided options. Aided AAC involves external equipment or technology and is classified as either a high-tech system (e.g., computer) or a low-tech system (e.g., eye gaze board). Unaided AAC does not have external equipment and includes sign language, gestures, vocalizations, and eye blink responses.1–3 Research investigating the use of AAC (aided or unaided) by individuals with MPS III is limited; however, there is ample research showing the benefits of AAC by those with developmental and/or acquired disabilities.4–17
MPS III includes four subtypes (A, B, C, and D) that vary in severity, symptomatology, and disease progression. Regardless of subtype, the initial symptom is language impairment and is followed by motor regression. MPS IIIA is characterized by three phases and includes (1) normal development, (2) delayed development including behavioral challenges and progressive cognitive deterioration, and (3) no further behavioral challenges but worsening motor difficulties. 17 Life expectancy for individuals with MPS III is 15.22 ± 4.22 years. 18
In children with MPS IIIA, language and cognitive abilities regress during childhood, with regression of both receptive and expressive language abilities. Language and cognition for children with MPS IIIA was found to reach a plateau around age 20–30 months followed by a period of severe regression occurring between ages 40–60 months and loss of natural speech by age 8 years.19,20 Few studies have investigated intervention for children with MPSIII focused on communication, and these studies only included children.20,21 Pérez-Núñez et al. conducted a study with three children with MPS III and found increased verbal and nonverbal communication given music stimulation. 21 Schreck et al. found that applied behavioral analysis therapy for a single 12-year-old child with MPS IIIA resulted in improved learning, maintenance of motor skills, reduction of behavioral challenges, and successful AAC use even after a period of cognitive and physical regression. 20 The current case report extends these previous investigations by introducing an aided low-tech AAC system to an adult with MPS IIIA who has lived beyond average life expectancy for this disease and presents with severe speech, motor, and cognitive impairments.
Case report
The current participant, Jane (name changed to protect privacy), was a 22-year-old female adult previously diagnosed with MPS IIIA at age 4 years (for full timeline, see Figure 5, Supplemental Materials). She experienced a progressive loss of language, motor, and cognitive abilities from ages 4 to 8 years and had lost all functional speech by age 8 years. AAC systems had been previously introduced between ages 8 and 16 years, but at the time of this study, she only communicated using eye blink responses to indicate “yes” or “no” in response to parent/caregiver questions. She had no other AAC systems or means of communication.
Initial assessment
A comprehensive assessment of language and communication was not conducted to comply with the wishes of the participant’s parents. An informal assessment (i.e., no standardized protocols) was completed to answer several diagnostic questions relevant to this case: (1) Could the participant respond in any way to caregiver responses; if so, how? (2) Could the participant use eye gaze toward an object when two objects were presented and she was asked to make a choice? (3) Could she use eye gaze toward a desired object or colors in an array of four photos when asked a question? This assessment was conducted prior to the start of the first baseline session. The participant demonstrated use of a blink to indicate yes versus no. She also used eye gaze to indicate one of two clothing items presented (when asked, “which coat do you want to wear”). Finally, she responded to questions using eye gaze toward colors and preferred objects when presented with an eye gaze board with a four-photo array, with photos placed in the four corners of the eye gaze board. These trials were not included in the baseline data and were used to determine if this young woman would potentially be able to respond to questions using an eye gaze board in response to caregiver questions.
AAC intervention materials
A 18 × 14 inch clear acrylic AAC eye gaze board, or E-Tran frame, was set up to display an array of four pictures (photos and/or images) at a time, with one image at each corner (see Figure 1). The vocabulary selected for use with the eye gaze board included the most relevant and functional words given the participant’s daily routine, preferred activities, and communication needs (e.g., activities, clothing items, locations, hair styles, animals, foods/drinks, colors, and emotions). It has been suggested that vocabulary selection for AAC be guided by two main principles including the need to convey essential messages and to promote language development. 1 With the participant in this case report, we considered the first of these two principles to be most relevant since this young woman was unlikely to show meaning gains in language development given her progressive cognitive decline. The selected functional vocabulary aimed to foster meaningful communication exchanges that were highly relevant to contexts and situations that our participant frequently encountered.22,23
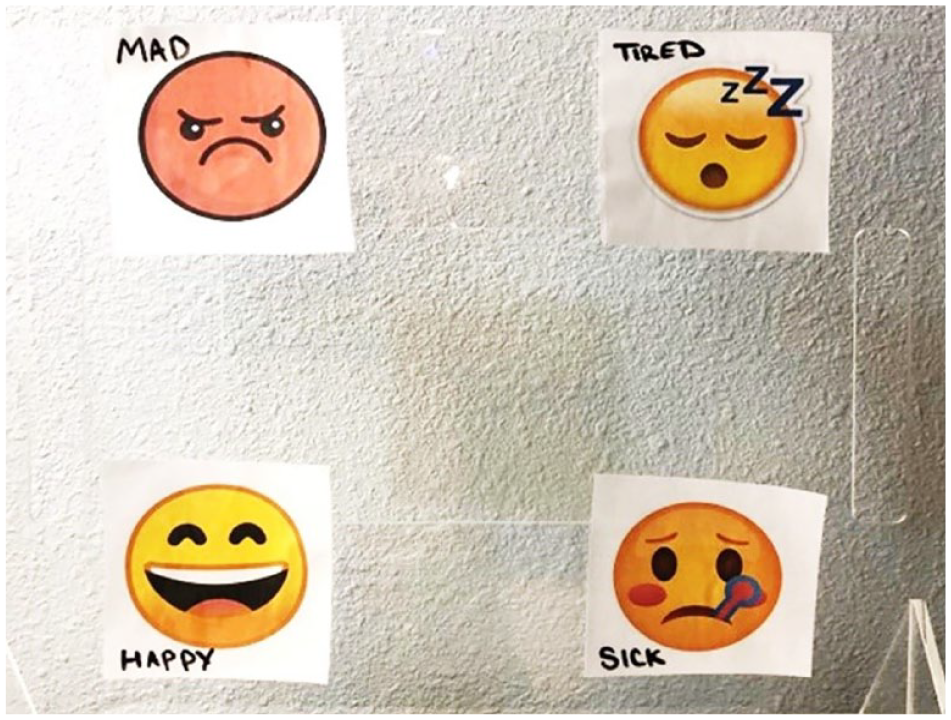
The eye gaze board was set up with a four-image array. This is an example of an array of emojis showing mad, tired, happy, and sick.
The size of all images/photos varied very slightly with images/photos being exactly or very close to 2 × 2 inches square. Color photos and printed color images were laminated and affixed to the eye gaze board using Velcro. Pictures were not always put on the board in the same location, and the location for a given picture was switched during each session and from session to session (see Figure 1). The picture array offered for any given question were all from the same semantic category (e.g., for a color question, choices offered may have included light purple, dark purple, yellow, and pink).
AAC intervention procedures
The participant received 29 AAC sessions occurring over 10 nonsequential days spanning 5 weeks. Sessions were not implemented by speech-language pathologists directly but were implemented by two nonfamily paid caregivers who had been working with the participant (and hired by her parents) for at least 6 months prior to the study. At the time of this study, these caregivers were providing daily care, including bathing, dressing, toileting, feeding, and engaging in leisure activities and therapies. After parents provided informed written consent for their daughter to participate in this study, her caregivers were given basic instructions and modeling regarding use of the eye gaze board and suggestions about how to use it with this participant by a speech-language pathologist with expertise in AAC and eye gaze systems. Session length was variable and ranged from 2 to 15 min (average of 9 min per session, with 22/29 sessions being 10 min in length) depending on the client’s level of alertness, mood, cooperation, fatigue, general health, and prioritization of other noncommunicative activities such as toileting, feeding, and addressing medical issues. The caregivers were responsible for data collection using videos, a notebook, and shared digital spreadsheet.
The initial 13 sessions were dedicated to the collection of baseline data and the only form of communication demonstrated by the participant was the already established yes/no blink response. Sessions 14–29 included the introduction and implementation of the eye gaze board. Caregivers were not told to change the types or numbers of questions they asked the participant, and they were told they could choose the pictures they used with the eye gaze board. They were given the freedom to use the board as much possible when they were working with the participant. While the original plan was to include more AAC sessions, a sudden change in the participant’s health resulting in a hospitalization led the decision to terminate the study after the 29th session. The participant kept the board and all pictures/photos after the study ended so that she could continue to use the system with her caregivers and parents, although no additional data for this study was collected.
During AAC sessions, caregivers engaged in typical daily activities for the participant, including bathing, dressing, feeding, and leisure activities such as art, music, listening to a book, and going out for a walk or to a coffee shop. The difference from the baseline sessions was that during these sessions the caregivers included use of the eye gaze board with up to four pictures at a time and asked the participant about her preferences, directing her to look at what she wanted/or how she felt. They provided multiple opportunities for her to respond to open-ended questions using the eye gaze board rather than only asking yes/no questions. For example, during dressing, a caregiver asked, “What color shirt do you want to wear today?” Other questions included but were not limited to, “How are you feeling today?” and “What do you want to do today?”
When asking open-ended wh-questions, caregivers implemented partner-assisted auditory scanning. They held up the eye gaze board for the participant to see her options and verbally named each picture on the board (i.e., partner-assisted scanning). Partner-assisted scanning was used here because this strategy has been recommended for use with individuals with CCN that include complex physical, cognitive, and sensory needs.24,25 Additionally, since this was a new system for this participant, the caregivers wanted to make sure the participant was attending to all possible choices. The participant could select her preference by looking at the desired picture for a minimum of two seconds, as judged by the caregivers. Initially, highly desirable pictures (e.g., music, pool) were offered along with less desirable options (e.g., stay home). Caregivers provided a wait time after asking questions for about 10 s to make sure the participant could scan the images before making her selection. During the initial sessions with the eye gaze board, the participant was occasionally asked to confirm her responses by also responding with yes/no blink responses. Best practice would have communication partners provide the item looked at and if it was not the item wanted (even though it was the item selected), the participant could initiate “no” to protest. In this case, the research team was aware of the participant’s existing yes/no blink responses and wanted to provide ongoing opportunities to use these responses and ensure they were not inadvertently extinguished.
The research team directed the caregivers to introduce four new photos/pictures every one to two sessions or as soon as natural opportunities arose (which ended up being almost every session). Since it had been several years since she used any form of AAC other than the blink response, the research-caregiver team wanted to slowly introduce the new system and prevent fatigue and/or rejection of the device.
Reliability
We measured interobserver reliability using video recordings for 20 out of 29 sessions so that coding of Jane’s eye gaze responses could be reviewed by multiple people. The caregivers reviewed the videos and coding together. Additionally, the lead researcher (first author) also met with the caregivers and reviewed their coding and agreement process. The team confirmed an interobserver reliability of 100% between the two caregivers for all of the participant’s responses for all of the recorded sessions.
AAC outcomes
The first outcome measure was the number of responses made or communication turns taken in response to caregiver questions using the eye gaze board during the treatment sessions. This outcome aimed to determine if the participant would use the eye gaze board to respond to questions in a real-world context once it was introduced and if her use of this system would increase over time. For this outcome, we only considered the treatment sessions since the eye gaze board was not available during the baseline sessions. While there was variability in the number of responses made using the eye gaze board per session ranging from one to five (see Figure 2), the trendline (calculated using the least squares method to find the line of best fit) showed a positive slope and suggested a small increase over time. For the sessions that included the eye gaze board (sessions 14–29), the participant responded to caregiver questions using this system at least once during all sessions.
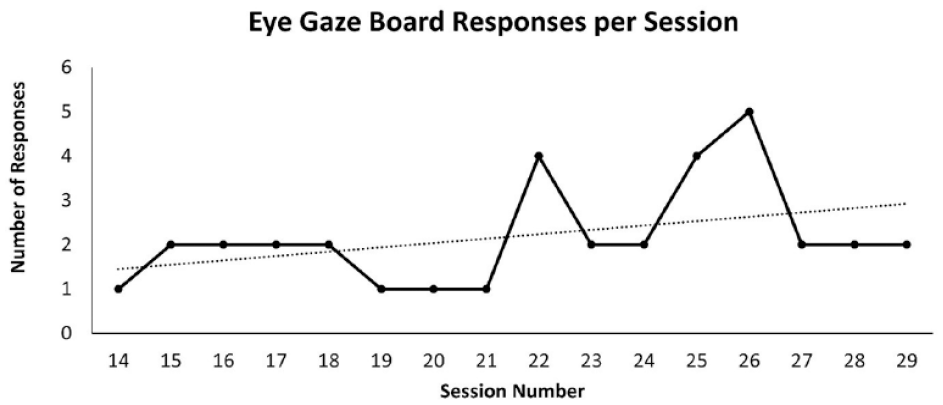
Number of responses made per session when asked choice-based questions using the eye-gaze communication board during the AAC treatment sessions only.
The second outcome measured was the total number of responses (or communication turns) to caregiver questions using either the eye gaze system or unaided yes/no responses. A visual analysis of the of the graphed data revealed notable session-to-session variability (see Figure 3). Despite this variability, the average total number of responses/communication turns remained relatively stable between the baseline and intervention sessions, with an average of 4.2 responses per session during the baseline and an average of 3.7 responses during the treatment phase. Visual inspection of the data plotted in a stacked bar graph suggested that during the treatment phase, the number of responses for each modality was similar (i.e., when yes/no responses were low, the eye gaze responses were also low). When the participant was responsive to caregiver questions, she utilized both her yes/no blink responses and responses using the eye gaze board. On days she was less communicative, she responded less across both modalities. The graph also includes the length in minutes for each session. While statistical tests were not conducted, there does not appear to be a trend or pattern between the session length and number of responses using either modality (see Figure 3).
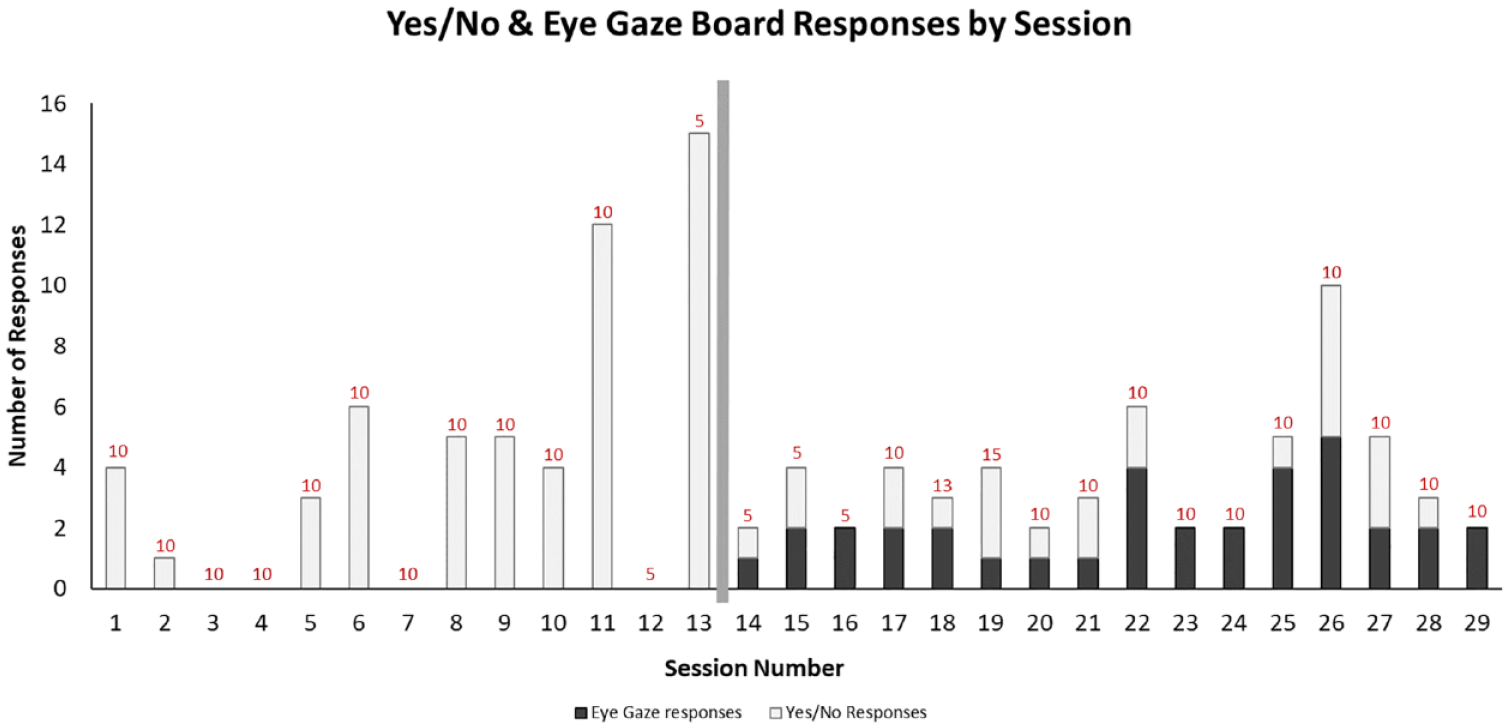
Total number of Yes/No (Blink) and eye-gaze responses per session.
The third outcome measured was the percentage of responses to caregiver questions. A visual analysis of the graphed data shows variability from session to session (see Figure 4). The trendline, calculated using the least squares method to find the line of best fit, shows a small positive trend over time. Additional inspection revealed four baseline sessions with 0% responses to caregiver questions, but no instances with 0% responses after the eye gaze board was introduced. Additionally, once the was introduced, there were no sessions with less than a 40% responses rate. While variability continued after the eye gaze board was introduced, the ratio of responses to caregiver questions increased, and there was less variability once the AAC system was being used. The percentage of responses to caregiver questions before the eye gaze board was used was 55%, and the percentage of responses to caregiver questions after the eye gaze board was used was 71%.

Ratio of responses using all communication methods (Yes/No Blink and eye gaze board responses) to all questions asked.
The fourth outcome measured was the total count of expressive vocabulary items that were being offered with the eye gaze board. While this is not necessarily a participant-driven outcome (since it depends on what pictures the caregivers present at any time), it does reflect the possible variety of responses that could be communicated with communication partners. During the initial sessions, the participant’s only responses were blinks to indicate “yes” and “no.” Therefore, her repertoire of possible expressive vocabulary was restricted to two words (“yes” and “no”). By session 29, caregivers were using 49 unique photos/images with the eye gaze board when asking the participant questions. While 49 pictures were being used with the eye gaze board, her responses included selection of 30 of these items across all questions asked and all AAC sessions.
Accuracy of eye gaze responses
During the AAC intervention sessions, yes/no questions were used to validate some choices or unclear choices, but responses to all of these questions were either “yes,” or there was no responses. We cannot interpret nonresponses as “no,” and it is not possible to determine exactly why she did not respond to those questions; however, her caregivers reported that she sometimes refused to answer questions when she was feeling fatigued or unwell or when she was unhappy with the current activities.
It was common for this participant to not respond at all or to respond to questions in way that was not clear to her caregivers, rather than to respond “no.” In total, across all sessions, 81 yes/no questions were asked, and 12 (14.8%) of the clear responses were “no.” None of these “no” responses followed a verification or confirmation of an eye gaze choice (100% of the confirmation responses were “yes”; see Table 1 for examples of communicative exchanges during several sessions). This could be interpreted as the participant making intentional choices with accuracy, but an alternative interpretation is that she went along with the eye gaze selections as interpreted by her caregivers. These interpretations will be addressed further in the discussion.
Samples of conversational exchanges between caregiver and participant.
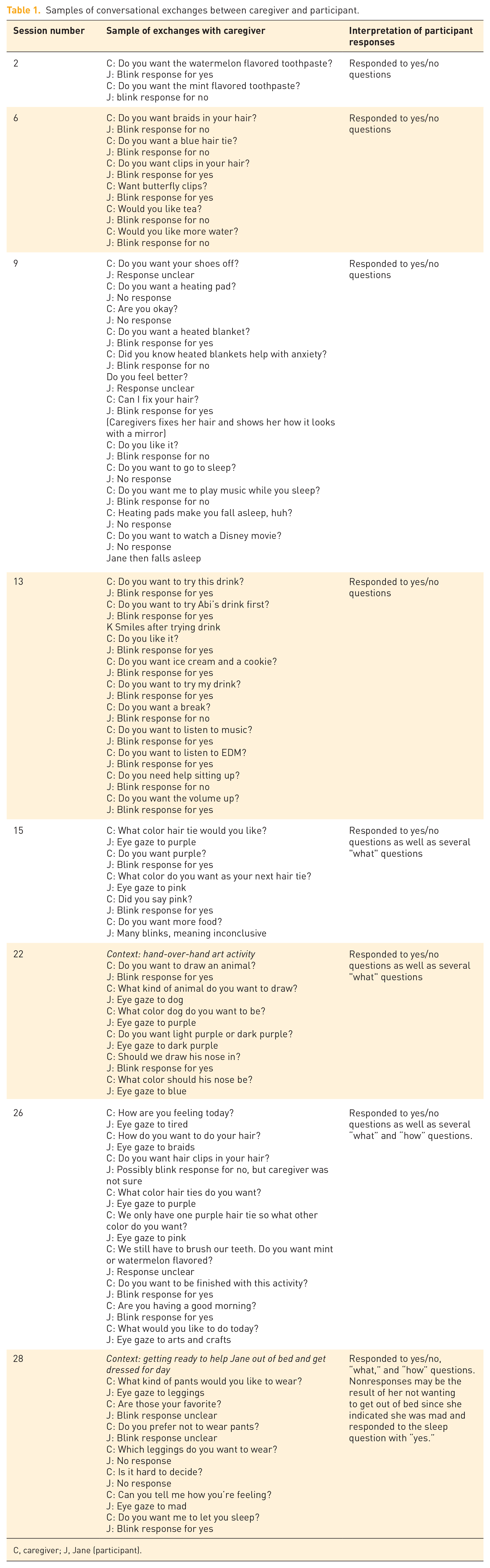
C, caregiver; J, Jane (participant).
The caregivers commented that when there were situations in which participant responses were more appropriate than other possible responses. For example, she had two coats that she wore regularly. A heavy one that was purple and a lighter one that was blue. When told what the weather was like and then asked what color coat she wanted to wear (given four colors), the participant reportedly always picked the color purple or blue and not a color that didn’t match a coat she owned (e.g., pink or green). Additionally, the caregivers reported that she also picked the most appropriate coat given the weather (i.e., the heavier coat when it was very cold, and the lighter coat when it was cool but not cold).
One of the caregivers shared an anecdotal story that also relates to intention and accuracy. When asked what color socks they should get for the participant’s father as a gift for his upcoming birthday, the participant kept selecting pink and confirming with a yes blink response. The caregiver thought this was strange since she did not recall seeing the father wearing pink and she wondered if this was an eye gaze error or reflected an unintended response. When she told the parents this later, they laughed and said suggesting pink clothes for the father was an ongoing family joke since he never wore pink clothes. Knowing this, the caregiver felt confident that the participant was using the eye gaze board to share the joke with her.
Qualitative changes to participant responses
Examination of the types of caregiver questions that the participant responded to provides additional information regarding qualitative changes to her responses to caregiver questions. Specifically, during the baseline period, the participant only responded to yes/no questions, but once the eye gaze board was introduced, she also responded to “what” and “how” questions. Because the ability to respond to different questions depends on the vocabulary offered/accessible, the participant was not able to answer “what” and “how” questions when solely relying on a yes/no blink response. This qualitative change appeared to be due specifically to the introduction of the eye gaze board as a new communication modality. As noted previously, see examples of communicative exchanges between the participant and her caregivers in Table 1. Finally, both caregivers reported feeling as if use of the eye gaze board gave them an opportunity to get to know the participant better. One of them reported that she, “got to learn more about Jane’s personality and sense of humor” than she had when they were relying solely on the yes/no responses.
Discussion
The participant in this study, a 22-year-old adult with postregression symptoms of MPS IIIA and no natural speech, showed quantitative and qualitative changes to her communication behavior after an eye gaze AAC board was introduced. Prior to this study, the participant was in a passive communication role, only responding to yes/no questions by blinking her eyes. After the eye gaze board was introduced, she responded to a greater percentage of questions per session, and she responded to qualitatively different types of questions (e.g., “what” and “how” questions) related to her daily activities and her emotions. During the baseline when only yes/no questions could be answered, several sessions included zero responses to all caregiver questions. Once the eye gaze board was introduced, the participant responded to at least one question in every session using either modality. There was also a slight positive trend in the number of eye gaze responses over time and no decrease in the total number of responses to questions during individual sessions. In other words, the level of overall communicative responses was similar during the baseline and the intervention sessions, but we interpret this to mean that while the participant’s engagement in communicative exchanges stayed constant, the quality of her responses changed. These outcomes support the conclusion that the young adult in this study was able to use the eye gaze board to supplement her existing modality of communication and to respond or take communication turns given caregiver questions. It also supports her potential to initiate more communicative interactions rather than responding to questions, which is common among AAC users.
In AAC intervention, one of the primary goals is to promote use of the AAC system in interactions, allow the user to learn the system itself, and increase conversational and social exchanges with others. When someone is starting to use a new system, his or her selections should be validated to promote use and confidence. Expanding the nature of language used and improving the accuracy with clearly correct answers may not be the initial goals of AAC intervention. In this case, the participant only had 16 intervention sessions. We argue that her accuracy at this stage was less critical than the fact that is evidence that she was looking at selections that the caregivers interpreted as meaningful, shaping, and reinforcing her attempts to communicate. At the same time, the participant continued to use her established yes/no blink responses without any loss to the number of communicative responses made during sessions over time. Light and McNaughton suggested that individuals who require AAC must develop skills to meet functional communicative demands for real-world interactions within their natural environment. 3 They state that communication should not be the end goal, but rather, individuals with CCN should be able to use AAC to participate effectively and attain their goals across multiple natural settings. Based on these recommendations, we argue that this participant’s accuracy at this early stage of using this AAC system is less critical than the fact that we found evidence that she is responsive to this system. Specifically, her eye gaze responses are acknowledged by her caregivers and she is continuing to respond to questions using both modalities, her established yes/no blink responses and the eye gaze board. Most importantly, the qualitative nature of her expressive communication has changed. We further suggest that it is less relevant whether or not this participant’s selections were made intentionally or were even accurate representations of her intentions, but that what was most important was that she was engaged in social interaction during real-world activities in her natural environment using a system that could be a vehicle for personal empowerment. Through the availability and ongoing use of this new system, accuracy can be targeted as a future expressive communication goal.
The data for the targeted communication goals reveal a significant amount of variability. According to the caregivers, who knew the participant well prior to the initiation of this study, her daily health and level of fatigue varied. They reported that she had “good days” and “bad days.” On good days, she was more alert and communicative, using both the eye gaze board and yes/no blinks in response to caregiver questions. On what the caregivers considered bad days, she would refuse to look at the board or at the caregivers and often whined or cried. Most likely, the variation that is noted in the graphs is a product of the fluctuations in her health and level of fatigue.
Currently, over 100 rare (and ultrarare) neurodegenerative genetic disorders that result in childhood dementia have been identified, including the seven types of MPS. 26 While the current study addressed a gap in the literature related to one subtype of MPS III and AAC, it potentially provides information (albeit limited) about how AAC may be beneficial to other children, adolescents, and young adults with CCN due to neurodegenerative genetic disorders and childhood dementia. The current findings are encouraging. Clinicians, educators, and caregivers working with other children and young adults with degenerative conditions may find that this case report provides some ideas for ways in which AAC may be beneficial; however, caution is recommended to those who are eager to find evidence to support clinical or educational treatment planning since the current results may not generalize to others.
In this case, the primary role of the caregivers was on caregiving (bathing, clothing, attending to medical needs, and engaging in daily activities) rather than on AAC intervention. This can be seen as both a limitation and a benefit to this study. It is a limitation because the caregivers were not AAC experts and did not have extensive experience in AAC implementation, yet the participant still appeared to use the system to respond and take turns, resulting in positive changes to the quantity and quality of her communication. Caregiver implementation is also a benefit because the use of the AAC system was naturalistic (e.g., embedded into daily routines versus scheduled sessions implemented outside of her typical routine). The naturalistic setting in which the AAC was used should make its use easier to maintain than if it were introduced solely in more restrictive clinical settings. Additionally, the AAC intervention was implemented when possible, rather than during a set schedule or for a set duration of time. Again, this is both a benefit, because it provided flexibility based on the participant’s needs, and a limitation, since the schedule was variable (and thus, not easily replicable). While not having a set schedule for AAC intervention sessions will make it difficult to replicate the procedures here, the level of flexibility utilized here can also be seen as further evidence that participant was able to expand her communication with caregivers using the new system within her natural environment despite a lack of regular and frequent AAC intervention sessions.
Conclusion
In this case report, we introduced an eye gaze board to a 22-year-old adult without speech and with postregression MPS IIIA and found quantitative and qualitative changes to functional communication. The participant used the eye gaze board to respond to caregiver questions in a naturalistic setting. The caregivers who provided the AAC intervention had minimal training and oversight and only implemented short AAC sessions as their time allowed since their primary focus was on caregiving needs. Despite this, the participant consistently responded with the eye gaze system during all sessions and accessed 30 vocabulary items presented as pictures on the eye gaze board. She also maintained use of her preexisting yes/no blink responses. These outcomes occurred despite health issues, fatigue, fluctuating motivation, a limited number of treatment sessions, and implementation by caregivers with limited AAC knowledge and experience. To date, this is the first study that focused on AAC and communication outcomes for an adult with MPS IIIA. While all case studies have inherent limitations, this study addresses a gap in the literature by demonstrating that a young adult with MPS IIIA could use a new eye gaze board to respond to caregiver questions, improving the quantity and quality of functional communication and promote a greater quality of life.
Supplemental Material
sj-docx-1-trd-10.1177_26330040241275672 – Supplemental material for Successful use of an eye gaze AAC communication board by a young adult with advanced Sanfilippo Syndrome (MPS IIIA): Case report
Supplemental material, sj-docx-1-trd-10.1177_26330040241275672 for Successful use of an eye gaze AAC communication board by a young adult with advanced Sanfilippo Syndrome (MPS IIIA): Case report by Christine Brennan, Abigail Matthews and Sherri Tennant in Therapeutic Advances in Rare Disease
Footnotes
Acknowledgements
We thank the participant, her family, and her two caregivers for their participation in this study.
The results reported here were also reported as part of a senior honors thesis project completed in March 2023 by author Abigail Matthews, B. A., under the direction of Christine Brennan, Ph.D. CCC-SLP at the University of Colorado, Boulder. The authors would like to thank those who served as committee members for Ms. Matthew’s thesis, including coauthor Sherri Tennant, Department of Speech, Language, and Hearing Sciences, and Emily Richardson, Ph.D., Department of Psychology and Neuroscience. Preliminary results from this study were presented at the American Speech-Language Hearing Association (ASHA) convention in November 2022, the Colorado Speech-Language and Hearing Association (CSHA) Convention in October 2022, and the Assistive Technology and Industry Association (ATIA) in January 2023
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.