
Abstract
Background:
Adult Polyglucosan Body Disease (APBD) is an ultra-rare, genetic neurodegenerative disorder caused by autosomal recessive mutations in the glycogen branching enzyme gene. Knowledge of the demographic and clinical characteristics of APBD patients and the natural history of the disease is lacking. We report here initial results from a patient-reported registry of APBD patients.
Objectives:
(1) Maximize the quality of the APBD Registry survey data; (2) provide an initial report on APBD disease progression and natural history using these data; and (3) specify next steps in the process for testing potential new therapies.
Design:
Data are from members of the APBD Research Foundation (New York), surveyed from 2014 by the Columbia APBD Patient/Family (CAP) Registry. Inclusion criteria are: disease onset at age 18+ and progressive clinical triad of peripheral neuropathy, spasticity, and neurogenic bladder.
Methods:
Genetic testing results were used when available. Respondents found to not have APBD in clinical records were excluded. All changes and exclusions were recorded in a database edit log. Results are reported in frequency tables, bar graphs, time plots, and heat maps.
Results:
The 96 respondents meeting inclusion criteria were predominantly (96.8%) White, highly educated (89.3% at least some college education), and mostly (85.1%) of Ashkenazi Jewish descent. 57.1% had at least one parent born in the United States, with at least one grandparent from Europe (excluding Russia; 75.4%), the United States (42.1%), or Russia (33.3%). 37.2% reported a family history of APBD, and 33.3% had an affected sibling. Median APBD onset age was 51 [Interquartile range (IQR) 11], and median age of diagnosis 57 (IQR 10.5). The 75 reported prior misdiagnoses were mainly peripheral neuropathy (43, 60.6%) and spinal stenosis (11, 15.1%).
Conclusion:
Although from a demographically constricted survey, the results provide basic clinical information for future studies to develop treatments for APBD.
Plain language summary
Adult Polyglucosan Body Disease, or APBD, is an ultra-rare neurological disorder caused by mutations of the GBE1 gene. While potential therapies exist, to establish if they work we need a “natural history” study that shows the normal path of the disease. Our goal was to provide the first patient-reported natural history study of APBD.
We analyzed survey data from 96 patients recruited by the APBD Research Foundation (New York), aged 18 or older, who self-reported having APBD. We maximized data quality by using results from genetic testing when these were available, and by excluding respondents if we could not review clinical records confirming they had APBD.
More than 95% of our 96 patients were white. They were highly educated: 89% had at least some college education. Most (85%) were of Ashkenazi Jewish descent. More than half (57.1%) had a parent born in the United States. Many had at least one grandparent from Europe (excluding Russia) (75.4%), the United States (42.1%), or Russia (33.3%). More than a third (37%) reported a family history of APBD, and a third reported that they had a brother or a sister with a history of the disease. Their average age at APBD onset was 51, and their average age at APBD diagnosis was 57. Previous misdiagnoses were common: 75 were reported. Most were for peripheral neuropathy (60.6%) or spinal stenosis (16.7%).
Although our data come from a survey of patients who are demographically similar, they provide a report on the characteristics of patients with APBD and basic information that is essential for studies to develop treatments for the disease.
Introduction
Adult Polyglucosan Body Disease (APBD) is an ultra-rare, genetic neurodegenerative disorder characterized by progressive spastic paraparesis, sensory deficits in the distal limbs, neurogenic bladder, gait impairment leading to loss of ambulation, and premature death due to complications of myelopathy and peripheral neuropathy.1,2 It is caused by autosomal recessive mutations in the glycogen branching enzyme gene (GBE1) that diminishes enzyme activity to 8–25% of normal levels, and symptoms typically present after the fifth decade of life. The neuropathological hallmarks of APBD are polyglucosan bodies (PBs), which are accumulations of sparsely branched insoluble glycogen both in the central and peripheral nervous system. In neurons, PBs in axons impair flow of cellular components between the cell body and peripheral terminals and lead to central nervous system demyelination, gliosis, and degeneration of peripheral nerves.3–9 In part due to its rarity, the disease is often initially misdiagnosed as multiple sclerosis, benign prostatic hypertrophy, or amyotrophic lateral sclerosis.1,2
In APBD, the ratio of glycogen synthase to GBE activity is increased. This indicates targets for potential therapies,10,11 such as decreasing glycogen synthase activity or increasing GBE activity via antisense oligonucleotide treatments to correct splicing of intronic mutations 12 or viral mediated gene replacement therapy. 13 There are also therapeutic efforts to decrease polyglucosan accumulation with small molecules.10,14 However, these drug development efforts, and any eventual clinical trials, will require detailed knowledge about the natural history of the disease. While one prior publication reports its natural history retrospectively in a small cohort of subjects (N = 50), 15 there is a dearth of information on the natural history of the disease. This is primarily due to its ultra-rarity; there are over 200 genetically confirmed APBD cases worldwide, though it is estimated to affect up to 4000 individuals globally, the majority of whom are of Ashkenazi Jewish descent.16,17 To overcome the challenges presented by a small prevalence, we used a patient-reported registry to perform the largest natural history study of APBD to date.
Aims and research objectives
This project analyzes and reports on data from the first patient-reported registry for APBD which was launched in 2014. The Columbia University APBD (CAP) registry is a collaboration between Columbia University Irving Medical Center APBD investigators and the APBD Research Foundation leaders and its Scientific Advisory Board. The Foundation team shared information about the CAP registry with its community via the Foundation website and newsletters. Additionally, they contacted patients and family members to inform them about the importance of participating in the registry and support the recruitment efforts. The specific objectives for the analysis were: (1) to maximize the quality of the APBD Registry survey data; (2) to provide an initial report on APBD disease progression and natural history using these data; and (3) to specify next steps in the process for testing potential new therapies.
Methods
The data collected in the APBD survey include demographics, age-at-diagnosis, age-at-onset, birth country of parents and grandparents, parents’ consanguinity, and family history of APBD. The criteria for inclusion in the current analysis are the disease onset of at least 18 years of age and progressive manifestation of symptoms, signs, or both of the triad of peripheral neuropathy, spasticity, and neurogenic bladder.
To achieve our first goal of maximizing data quality, free-text responses on parents’ and grandparents’ countries of birth were standardized to generate accurate frequency counts. Duplicate dataset entries with conflicting information were then reconciled. Although the earliest age-at-onset for APBD has not been clearly defined, some previous research has used 30 years as the criterion. To investigate this question, in addition to the inclusion criterion of onset at 18 years and older, the clinicians reviewed all cases with a reported onset age of 30 or younger. Needed clarifications on variables of interest were sought from patients for whom contact information was available. Variables were updated for those who responded, and missing values recorded for those who did not. Genetic testing results were used when available. Respondents found to not have APBD in clinical records available to the clinical team were excluded. A detailed database edit log recording all changes and exclusions was created.
The results are reported in frequency tables, bar graphs, time plots, and heat maps.
Results
126 individuals responded to the initial APBD Research Foundation survey. After data review and cleaning, 96 of these met the criteria for APBD and are included in the current analysis. Table 1 reports their demographic characteristics. Median age of APBD onset is 51 (IQR 11), and median age of diagnosis is 57 (IQR 10.5; Table 2).
APBD respondent demographics (Overall N = 96).

APBD, adult polyglucosan body disease.
Age at APBD Onset and Diagnosis.
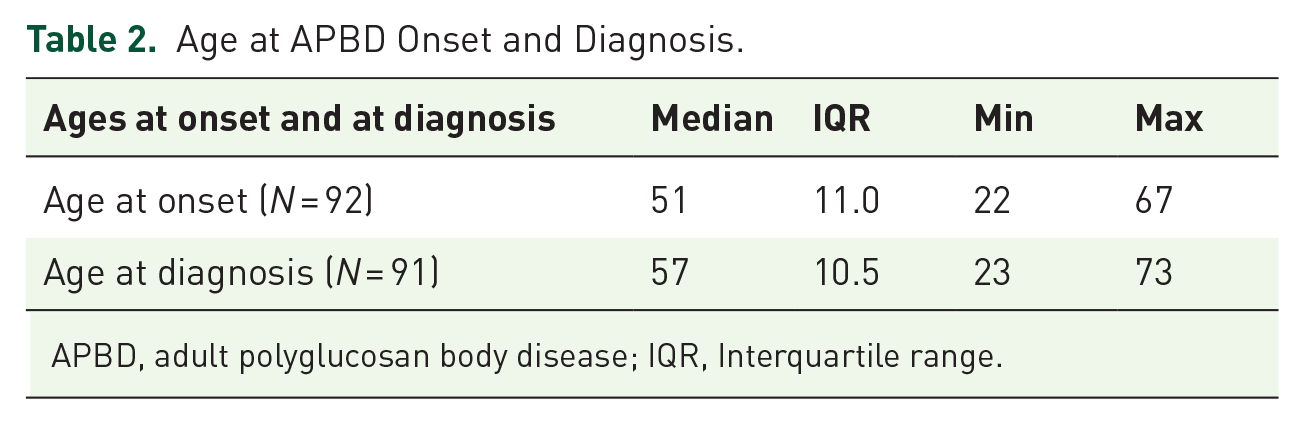
APBD, adult polyglucosan body disease; IQR, Interquartile range.
Our 96 respondents reported receiving a total of 75 prior misdiagnoses from a pre-specified list of peripheral neuropathy, spinal stenosis, amyotrophic lateral sclerosis (ALS), multiple sclerosis (MS), prostate cancer, and benign prostatic hyperplasia (BPH). Peripheral neuropathy was the most frequent, reported by 43 patients (60.6%). Spinal stenosis was the second most frequent, reported by 11 patients (16.7%).
Other selected misdiagnoses were ALS (3), MS (7), prostate cancer (3), and BPH (8) (Table 3). Of the patients who reported any misdiagnoses, 30 reported one, 15 reported two, and 5 reported three. All 20 patients who reported more than one misdiagnosis reported peripheral neuropathy.
Previous Misdiagnoses Reported by APBD Patients (Overall N = 96 patients).

APBD, adult polyglucosan body disease.
The majority of patients had at least one parent born in the United States (57.1%) [Figure 1(a)], while an overwhelming majority of patients (75.4%) had at least one grandparent born in Europe (excluding Russia). The next most common birth countries for at least one grandparent were the United States (42.1%) and Russia [33.3%; Figure 1(b)].

Legend: Countries of birth of parents (a) and grandparents (b) are displayed. Colorcoded heat maps indicate relative numbers of parents (a: mothers = red, fathers = blue) and grandparents (b: orange-yellow) in each geographic region.
Among 78 respondents, 29 patients (37.2%) reported having ‘any’ family history of APBD. Twenty-six patients reported a sibling with a history of the disease and five reported more than one relative with a history (Table 4). Twelve patients reported parental consanguinity.
Reported responses of family history of APBD (Overall N = 96).

APBD, adult polyglucosan body disease.
Discussion and conclusions
APBD has not previously been studied prospectively.15,18 The current retrospective analysis provides an initial foundation for further characterization of the disease. The results can be used to allow more informed planning and design steps for future studies and potential clinical trials for new therapies.
Potential biases of the study include: (i) recall bias for self-reporting ages-at-onset and diagnosis. The survey was patient-reported and, due to the neurodegenerative nature of the disease, recall of age-at-onset or age-at-diagnosis without clinical records could lead to inaccurate results. (ii) Location bias: the APBD Research Foundation is based in the US, which could lead to geographic bias of results. (iii) Socio-economic status bias: it is well known that socioeconomic factors have a sizable effect in healthcare outcomes and research.19–24 As shown in Table 1, this study population is highly educated, with over 70% of patients having a college degree or higher, making it worth considering that the study population may not be an accurate representation of the actual patient population. As genetic testing may not be available for all APBD patients, the patient population with this disease could be larger, spanning wider socioeconomic classes.
As is usual with ultra-rare diseases, the small sample size presents significant challenges in terms of statistical power; however, the APBD survey dataset provides the largest body of information on APBD patients to date. Overall, the results presented here provide the basic information which may lay the groundwork for future prospective natural history studies and clinical trials for potential treatments for APBD.
Moving forward, we plan to use these results to design a prospective natural history study to better understand the progression of the disease. Potential outcomes to measure the disease progression will focus on the APBD symptom triad and other understudied and potentially underreported symptoms such as cognitive changes, sexual dysfunction, loss of vision, impaired thermoregulation, and fatigue. Identifying and describing these key outcome measures will allow us to evaluate potential future therapies.
Footnotes
Acknowledgements
We gratefully acknowledge the creation of the survey by Salvatore DiMauro, MD; all the patients with APBD and their families who responded to the survey; the support of the ABPD Research Foundation in recruiting subjects and relatives; the Foundation’s financial support for data management of the project; Alexander Lossos MD, Edwin Kolodny MD, Or Kakhlon MD, and Raphael Schiffmann MD for contributions to development of the survey; and Jeff Levenson, DDS, David Epstein, and Harriet Saxe of the APBD Research Foundation for their community engagement and support with recruitment.