
Abstract
In this cross-sectional study, we analyzed data from the Survey of Risk Factors in a Secondary School Students (FRESC) representative survey among secondary school students aged 13 to 19 in the city of Barcelona. At all school grades, sexual harassment was more commonly reported by girls than by boys (17% of girls vs 4.2% of boys). The factors associated with sexual harassment were higher school grade, having a mental health disorder, cannabis abuse, and discrimination because of sexual orientation in girls and discrimination because of sexual orientation in boys. These findings highlight the potentially strong impact of sexual harassment on adolescents’ lives and underscore the importance of preventing this form of violence.
Introduction
The United Nations defines sexual harassment as “any unwelcome sexual advance, unwelcome request for sexual favor, verbal or physical conduct or gesture of a sexual nature, or any other behavior of a sexual nature that might reasonably be expected to be perceived as causing offense, humiliation, or intimidation to a person” (United Nations, 2008). In this article, we focus on exposure to sexual harassment and the health consequences that this type of violence can have on the adolescent population, who is subjected to it.
Theoretical bases of gender inequalities
Sexual harassment is a form of gender-based violence rooted in gender inequality and injustice. Anybody can experience this violence, regardless of their background, identity, or situation, although women, girls, and gender-diverse people are at high risk of sexual harassment. This study is grounded in a conceptual framework that aims to understand the determinants of interpersonal-relational models (Forcadell-Díez et al., 2023). In this framework, relational models based on equity contribute to well-being, while asymmetrical relationships based on hierarchies and power differences generate gender inequalities and violence and have a negative impact on mental, physical, and social health. Structural and intermediate determinants are identified as the combined action of systems of oppression, the socio-historical context that legitimizes and normalizes violence through social and cultural structures, and social stratification and segregation, resulting in inequitable access to power, resources, and opportunities. Intermediate determinants include individual, psychosocial, behavioral, and community aspects.
The feminist perspective conceives sexual harassment in western patriarchal capitalist societies as a mechanism to produce and perpetuate asymmetric power relationships (Conroy, 2013). It aims to penalize individuals who do not conform to the social rules determined by hegemonic heterosexual masculinity, which are also present in the school setting and continue to oppress women. However, hegemonic masculinity oppresses not only women but also men, particularly those who do not conform to traditional gender roles. In the construction of heterosexual hegemonic masculine identity, gender identity options are limited for men, creating asymmetric power relations and oppressing boys who do not match social norms, such as those with non-heterosexual orientations (Fineran, 2002; Robinson, 2005).
Health impact of sexual harassment
Gender-based violence is a major public health problem due to its multiple impacts on physical, mental, and social health (Artazcoz et al., 2019). Gender inequality is transformed into a health risk through discriminatory values, norms, beliefs, and practices; differential exposures and susceptibilities to disease, disability, and injuries; biases in health systems; and biases in health research (Sen and Östlin, 2007). The health impacts of gender-based violence are not only a consequence of living with and experiencing such violence: gender-based violence abruptly shapes the world around us, sustaining and legitimizing social structures, norms, and values. It also configures a differential access to rights, resources, and opportunities. Gender-based violence is both the driving force and mechanism of social inequities in health (Giammarioli et al., 2023).
Sexual harassment encompasses behaviors ranging from disturbing comments to psychological, sexual, or physical assaults. Being subjected to sexual harassment is a traumatizing experience with health consequences (American Association of University Women Educational Foundation, 2001; Fineran, 2002). A study conducted in Catalonia reported that 30% of teenagers aged 12–18 had experienced sexual harassment, and 19% had experienced this form of violence via social networks in 2016–17. A total of 12.7% of students had been subjected to sexually offensive comments, 6.1% to unwanted sexual interactions, and 1.7% undesired sexual molestations with violence (Idescat, 2018). According to the 2014 European Violence against Women Survey, one in 10 women experienced some form of sexual violence since the age of 15, while almost the same proportion reported that they had experienced some form of sexual violence by an adult before that age (European Union Agency for fundamental rights, 2014).
Multiple factors are related to sexual harassment victimization, including structural determinants such as ethnicity and socioeconomic level (Chiodo et al., 2009), as well as intermediate determinants, some of which involve the family setting, such as low parental education, unemployment, and family involvement (Dahlqvist et al., 2016; Kaltiala-Heino, Fröjd, and Marttunen, 2016b). In addition, sexual harassment victimization seems to be more common in non-heterosexual individuals (Mitchell et al., 2014). A total of 71% of non-heterosexual middle and high school students reported being sexually harassed during the school year compared with 32% of their heterosexual peers (Gruber and Fineran, 2008).
Sexual harassment victimization has been associated with a variety of psychosocial and physical health concerns, such as low self-esteem, depressive symptoms, use of alcohol, tobacco, cannabis, and self-harm, both in boys and girls (Bucchianeri et al., 2014; Eom et al., 2015). In boys, sexual harassment is associated with delinquency (Kaltiala-Heino, Fröjd, and Marttunen, 2016a), and in girls, it is linked to body image preoccupation, bodily dissatisfaction, and eating disorders (Petersen and Hyde, 2013). Girls are also at increased risk of academic problems, school absenteeism, and school disengagement (AAUW, 2011). Women also have a greater likelihood of depression, which increases in a dose-response manner among women reporting sexual harassment more than once (Gale et al., 2019). Additionally, individuals with non-heterosexual orientations more frequently report depressive symptoms than other groups (Collier et al., 2013). A study conducted in Australia found that non-heterosexual youths experienced higher rates of victimization because of their sexual orientation or gender identity, increasing the risk of suicidal ideation, suicide plans, and suicide attempts (Bouris et al., 2016).
Although non-heterosexual orientation has been described as a factor that may be related to sexual harassment (Bendixen et al., 2018; Fineran, 2002; Mitchell et al., 2014), few studies have explored the possible relationship between sexual harassment, sexual orientation, and health in youth. After conducting a literature review, we hypothesized that sexual harassment might be associated with poor mental health, poor physical health, and health-related factors, as well as non-heterosexual orientation or having been discriminated against because of sexual orientation.
The aim of this study was to analyze the prevalence and factors associated with exposure to sexual harassment victimization in high school students in Barcelona in 2016, taking into account sexual orientation, health, and health-related factors stratified by sex.
Methods
Design, setting, and sample size
In this cross-sectional study, the data analyzed were drawn from the Survey of Risk Factors in a Secondary School Students (Enquesta sobre Factors de Risc en Estudiants de Secundària [FRESC]) conducted by the Barcelona Public Health Agency (ASPB) in 2016 (Santamariña-Rubio, Serral-Cano, Pérez, and Ariza, 2017). FRESC is a periodic survey that is representative of the school population in the city of Barcelona. The survey is part of the Annual Statistical Action Program of Catalonia, which is specifically protected by law (Catalonia, Decree 255/2015).
The necessary sample size was calculated from official data on the number of students enrolled in schools in Barcelona from 2015 to 16. Considering a 3% precision and a 5% alpha error, and assuming a non-response rate of 20%, the required number of students needed in the survey was 4200 (2400 from ISCED Level 2 lower secondary education, aged 13–16 and 1800 from ISCED Level 3—upper secondary education, aged 17–19). Classrooms were used as the sample unit and were randomly selected, stratifying by school type (public or private), and the socioeconomic level of the school’s neighborhood. The survey was self-administered online to all students from the selected school classrooms. Before administering the survey, the ASPB obtained consent from the parents of students younger than 18 and from the young people themselves. The anonymous questionnaire was completed by 3888 students at their schools. The FRESC survey is part of the Statistical Action Programme of the autonomous government of Catalonia (Generalitat de Catalunya). Specifically, the survey is included in the Annual Statistical Action Program (PAAE) (adapted to Law 5/2016, of December 23, of the Statistical Plan of Catalonia, 2017–2020 and amending Law 23/1998 of statistics of Catalonia) under registration number: 09 01 03. For our study, we analyzed the anonymized data from the FRESC survey provided by the ASPB.
Dependent variables and covariates
The dependent variable was exposure to sexual harassment, which was defined in the survey as “any verbal or physical behavior with sexual content that is not welcome and that you perceive to be offensive.” This variable was measured through the question: “Have you ever been subjected to sexual harassment?” The dependent variable used was dichotomous (yes/no), while the stratification variable was dichotomous sex (boy/girl).
The main explanatory variables were: (a) Self-perceived health (good/excellent or regular/bad); (b) Mental health (no mental disorder, possible or probable mental disorder) measured as the probability of having a mental health problem with the Strengths and Difficulties Questionnaire (SDQ) (Goodman et al., 2000); (c) Binge drinking, defined as the consumption of five or more alcoholic drinks on the same occasion in the last 30 days (yes/no, never); (d) Cannabis use (yes in the last 30 days, yes but not in the last 30 days, never); (e) Bodily satisfaction (satisfied/dissatisfied) measured by the Contour Drawing Rating Scale (CDRS) (Dion et al., 2015); (f) Having experienced discrimination because of sexual orientation (yes/no), defined in the questionnaire as “feeling upset or feeling inferior because of your sexual orientation”; and (g) School grade (ISCED Level 2—lower secondary education for students aged 13 to 16 years, or ISCED Level 3—upper secondary education for students aged 17–19 years). Data analyses involved descriptive univariate and bivariate analyses to determine variation in the frequency distribution of sexual harassment across independent variables using the chi-square test. Bivariate prevalence of sexual harassment was also calculated separately for boys and girls. Additionally, bivariate and multivariate logistic regression analyses were conducted to obtain crude odds ratios (ORc) and adjusted odds ratios (ORa) with their respective 95% confidence intervals (95% CI). All analyses were stratified by sex. Stata 13 was used for all analyses.
Results
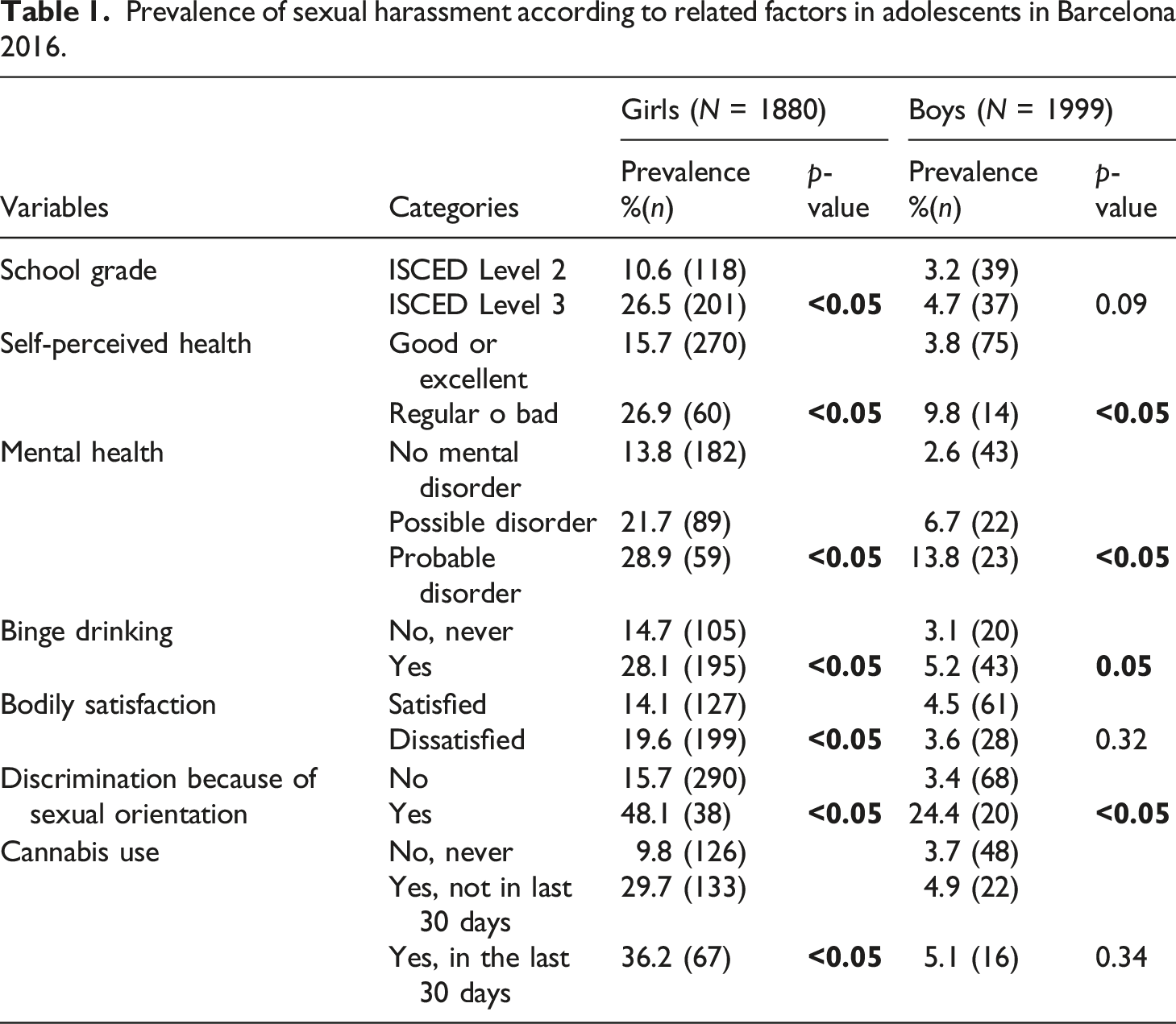
Prevalence of sexual harassment according to related factors in adolescents in Barcelona 2016.
Associations for sexual harassment and related factors in adolescents in Barcelona 2016.
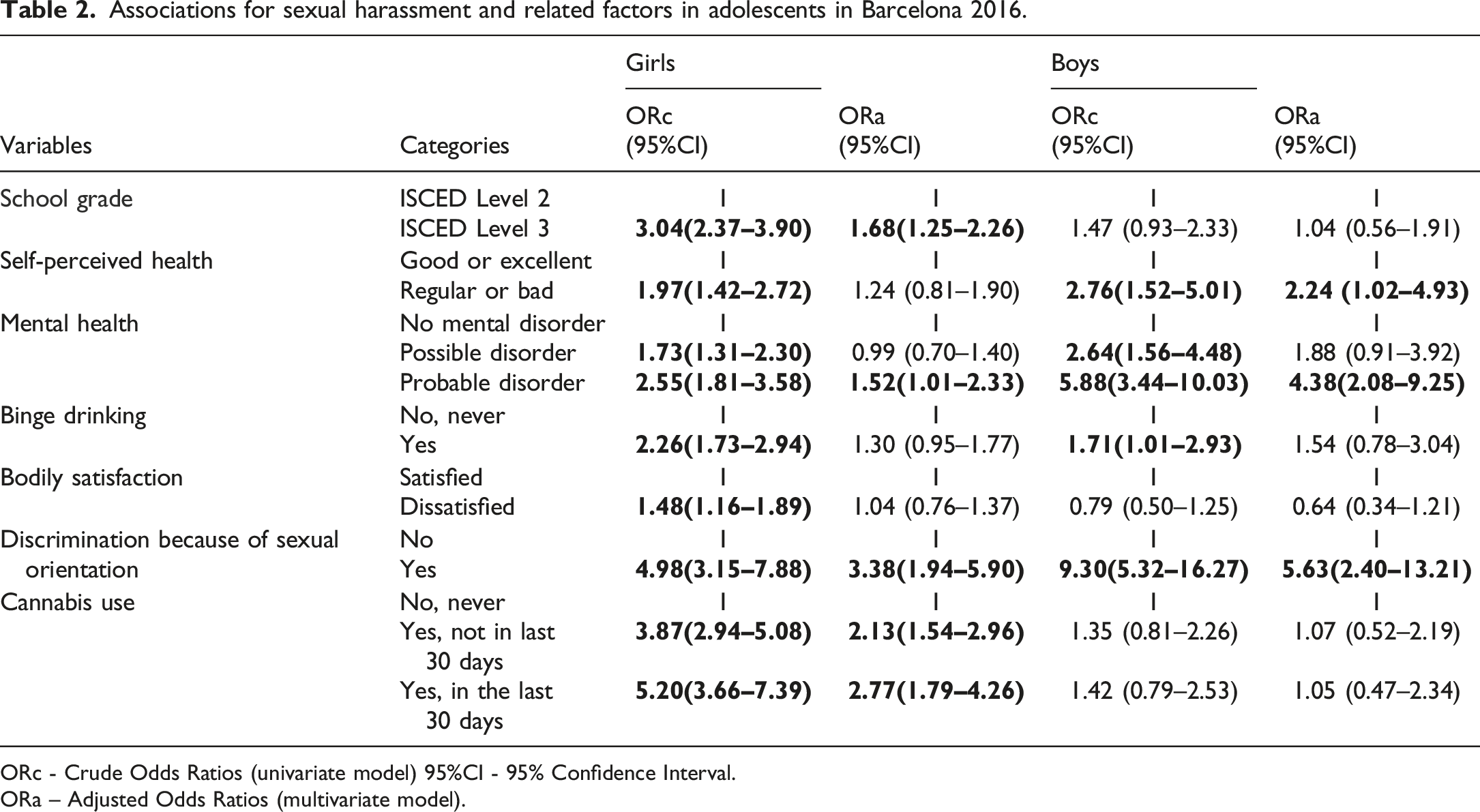
ORc - Crude Odds Ratios (univariate model) 95%CI - 95% Confidence Interval.
ORa – Adjusted Odds Ratios (multivariate model).
In the multivariate analysis, among boys, a regular or bad self-perceived health (aOR = 2.24; 95% CI = 1.02–4.93), having a probable mental health disorder (aOR = 4.38; 95% CI = 2.08–9.25), and experiencing discrimination because of sexual orientation (aOR = 5.63; 95% CI = 2.40–13.21) were associated with sexual harassment. Binge drinking was associated with sexual harassment in the crude model but was not statistically significant in the multivariate model. No relationship was found between sexual harassment in boys and school grade, bodily satisfaction, or cannabis use.
Discussion
This study found that mental health and health-related behaviors were associated with sexual harassment victimization in girls, who experienced more sexual harassment than boys. Among boys who experienced sexual harassment, self-perceived health and mental health were worse. Additionally, sexual harassment was associated with discrimination because of sexual orientation in both genders.
Prevalence of sexual harassment
A systematic review on teen dating violence in European countries concluded that there is a wide variability in the prevalence rates of teen dating violence, with adolescent girls reporting higher rates of all forms of teen dating violence victimization than their male counterparts (Tomaszewska and Schuster, 2021). In Spain, 57.4% of women aged 16 or older have experienced gender violence during their lifetime, but in younger women (aged from 16 to 24), the prevalence rises to 71.2% (Delegación del Gobierno contra la Violencia de Género, 2019). In Finland, the prevalence of sexual harassment among adolescents aged 14 to 18 has been reported to be 55% for girls and 40.1% for boys (Kaltiala-Heino et al., 2016a). Indeed, comparing prevalence rates across countries can be challenging due to methodological differences among studies. Variations in the definition of sexual harassment, sample selection, and the wording and grouping of survey questions can significantly impact reported rates (Bondestam and Lundqvist, 2020; Ilies et al., 2003). Defining sexual harassment is challenging, and published studies often utilize distinct measurement instruments. Definitions are frequently rooted in perceptions of cultural values, strongly influenced by cultural norms and gender roles that normalize or condemn sexual harassment. The definition and measurement approach play a crucial role in determining prevalence rates. Previous studies relying solely on the direct query model reported lower prevalence rates than those incorporating questions on specific behavioral acts such as suggestive comments, inappropriate staring, unwanted touching, and sexual telephone calls (Ranganathan et al., 2021). Some studies recommend analyzing physical harassment and non-physical harassment separately to identify potential differences in the factors leading to each type and to ascertain whether the consequences vary (Bendixen et al., 2018). It is essential to differentiate sexual harassment as a much broader term than sexual assault. While sexual harassment can encompass verbal, psychological, sexual, or physical actions, sexual assault specifically refers to physical acts. Unwanted touching, kissing, and groping are all types of sexual assault. It also includes situations in which a victim is forced to touch an abuser sexually. When sexual assault is perpetrated against children, the term most often used to describe it is sexual abuse. Until an individual turns 16 or 18, depending on the state, they cannot legally consent to sexual activities. If a sexual activity occurs with a child who has not reached the age of consent, it is considered sexual abuse. Before 2022, at the time the survey was conducted, in Spain, sexual abuse was legally differentiate of sexual assault. The so-called “only yes is yes” law (as the Ministry of Equality calls it) came into force on October 7, 2022. The main change it incorporates is the equalization of sexual abuse and assault. But it includes other important modifications that affect the Spanish Penal Code.
Health and health-related behaviors of sexual harassment
Our study’s findings align with existing research, emphasizing the association between mental health disorders and sexual harassment victimization, particularly in boys. Other studies have also indicated that boys who experience sexual harassment may exhibit depressive symptoms (Kaltiala-Heino et al., 2016a). The observed gender difference in mental health impact suggests that boys may perceive sexual harassment as a threat to their masculinity, leading to heightened stress and challenging coping mechanisms. The unexpected nature of these experiences for boys, who may not anticipate being targets of sexual harassment, contributes to the psychological toll (Folkman, 1984; Kaltiala-Heino et al., 2016a; Wolff et al., 2017).
Among girls, the relationship between mental health disorders and sexual harassment could be explained by studies that describe sexual harassment as a mediator between pubertal timing and depressive symptoms. Early puberty in girls has been linked to a higher likelihood of experiencing sexual harassment, and those girls may also be more prone to developing depressive symptoms (Skoog et al., 2016). The prevalence of sexual harassment was higher among girls with poor body self-image aligns with the reported effects of aesthetic pressure that operates to oppress women from a very young age in a patriarchal society. While the association did not reach statistical significance in the multivariate model, the trend suggests a potential impact of societal expectations and beauty standards on experiences of sexual harassment. It is notable that some authors have identified sexual harassment as a risk factor for both body image preoccupation and eating disorders. This relationship is reported to be especially strong in girls but is also present in boys (Buchanan et al., 2013). These findings highlight the interconnectedness of various societal pressures and their potential impact on mental and emotional well-being, emphasizing the need for holistic approaches in addressing the complex factors influencing adolescents’ experiences.
The study conducted by Petersen and Hyde (2013), supports the notion that experiencing sexual harassment during adolescence can have a profound impact on girls’ perceptions of their bodies. This experience may lead them to perceive their bodies as objects and develop negative feelings associated with bodily dissatisfaction and eating disorders. The findings underscore the complex interplay between societal influences, interpersonal experiences, and mental health outcomes during the crucial period of adolescence. Moreover, the exposure of girls and their bodies to hypersexualization can contribute to increased bodily dissatisfaction, eating disorders, and mental health problems. This highlights the need for a comprehensive understanding of the socio-cultural factors influencing body image and mental health in adolescence, as well as the importance of addressing these issues in a holistic manner.
Our study’s findings, indicating an association between sexual harassment and substance use in girls, align with previous research that has reported similar relationships (Bucchianeri et al., 2014). However, the observation that the association was found only with alcohol abuse in boys in the crude model suggests potential gender-specific nuances in the impact of sexual harassment on substance use. The discrepancy with other studies that reported an association between sexual harassment and higher substance use in both sexes could indeed be influenced by the lower number of boys experiencing sexual harassment in our study. It highlights the importance of considering gender-specific variations and the prevalence of experiences when interpreting associations between sexual harassment and health-related behaviors (Bucchianeri et al., 2014). Understanding these nuances is crucial for tailoring interventions and support mechanisms that address the specific needs and experiences of boys and girls in the context of sexual harassment and its potential consequences.
The insights derived from our study are in line with existing research, underscoring the variability in the impact of sexual harassment based on how individuals, particularly girls, cope with such experiences. It is important to note that the repercussions of sexual harassment are not limited solely to girls identifying as feminists. The finding that girls who identify as feminists, characterized by the belief in equal treatment for males and females, are more likely to confront perpetrators and seek social support suggests that active coping strategies may help protect individuals from the negative psychological effects of sexual harassment (Leaper et al., 2013; Brown, 2016). Empowering girls through preventive programs that promote awareness, assertiveness, and support-seeking behaviors can be valuable in addressing and mitigating the impact of sexual harassment. By fostering a sense of agency and resilience, such programs contribute to creating a supportive environment that encourages individuals to stand up against harassment and seek help when needed. These findings underscore the importance of multifaceted approaches that encompass both preventive measures and support mechanisms to address the complex challenges posed by sexual harassment.
Gender, sexual orientation, and sexual harassment
Discrimination indeed manifests in various forms and can be rooted in power imbalances related to gender, sexual orientation, ethnicity, disability, and other factors. Secondary school students may face discrimination on multiple fronts, reflecting societal inequalities. The intersectionality of these identities adds complexity to the experiences of discrimination and underscores the importance of considering multiple dimensions when addressing these issues. The increased likelihood of transgender and non-binary youths reporting experiencing sexual violence compared to cisgender individuals, highlights the vulnerability of specific groups within the student population (Ybarra et al., 2022). Our analysis aligns with previous studies indicating an association between sexual harassment and discrimination due to sexual orientation. As reported in previous studies, non-heterosexual youth report higher victimization rates than their heterosexual peers (Mitchell et al., 2014); in 2014, 11.8% of the non-heterosexual youths in Australia experienced sexual assault (Hill et al., 2020). While our study found a link between sexual harassment and discrimination based on sexual orientation, it is essential to recognize that heterosexual orientation should not be assumed when inquiring about such discrimination. Discrimination itself can have profound impacts on people’s health, and societal relationships between different groups, including non-heterosexual and heterosexual individuals, play a significant role in shaping health outcomes (Krieger, 2014). The higher prevalence of mental health disorders among non-heterosexual individuals is often attributed to the stressors associated with stigma, prejudice, and discrimination (Friedman, 1999). Social stress theory aligns with the broader understanding of the impact of social determinants on mental and physical health. Social stress theory posits that conditions in the social environment, beyond personal events, can serve as sources of stress, potentially leading to adverse health effects. This theory is particularly relevant for individuals belonging to stigmatized social categories, including those related to socioeconomic status, race/ethnicity, gender, and sexuality (Link and Phelan, 2001; Meyer, 2003; Pitoňák, 2016). One elaboration of social stress theory can be referred to as minority stress theory. Minority stress is additive to the general stressors experienced by everyone; this form of stress is chronic, is related to relatively stable underlying social and cultural structures and is socially based, stemming from social processes, institutions, and structures beyond the individual rather than from individual events or conditions of the person or the group (Meyer, 2003). The parallel mechanisms leading to both sexual harassment and discrimination due to sexual orientation are noteworthy. Both behaviors (sexual harassment and discrimination) are also tools to perpetuate power relations and inequalities and to victimize and subjugate people not following the established social norms or “normality,” in this case, heterosexuality (Conroy, 2013).
Strengths and limitations
Acknowledging the study’s limitations is an important aspect of scientific research. The recognition that the results may underestimate the prevalence and associations of sexual harassment in the older age group (17 to 19 years) due to the survey’s representation only of those attending school at these ages is a valid consideration. This limitation is inherent to the sampling strategy and highlights the need for caution when generalizing findings to the broader adolescent population in that age range. On the positive side, the study’s results are representative of the adolescent population in Barcelona aged 13 to 16 (ISCED 2), as secondary education is compulsory in Spain until this age. This indicates the importance of considering the specific context and educational policies when interpreting and applying the study findings.
Another limitation is that the number of effectives does not allow us to stratify the analysis by sex and age simultaneously. However, we have stratified the analysis by sex and we have included the grade, a proxy of age in the multivariate models adjusting the association measures to control the possible confounding effect of age.
Also, the consideration of social-desirability bias in responses related to binge drinking and cannabis use is insightful. Nevertheless, as the questionnaire is anonymous and was conducted online, the effect of this bias was minimized. Because this is a cross-sectional study, we cannot assume causality, and therefore do not know the direction of the association and therefore there could also be a bias of inverse causality. In other words, the exposure causes the risk factor.
Another limitation of the study is that the survey used does not include questions about participants’ gender diversity, which would have been interesting to analyze possible associations. The survey was designed before we started the study and consequently, we used the data available at that moment.
Finally, a major strength of this study is that we included sexual orientation discrimination simultaneously with health and health-related behaviors as explicative variables, which has not been explored in previous studies.
Conclusions
Sexual harassment is a pervasive issue among girls and boys school-aged adolescent in Barcelona and is experienced by one in four older girls. This traumatic experience not only affects their health and well-being but also exacerbates discrimination based on sexual orientation. There are two key points to address sexual harassment: Firstly, information sources, and secondly, programs and interventions aiming to prevent sexual harassment and provide comprehensive education to promote healthy and equitable relationships among adolescents.
Regarding the first point, the data source in this study was the FRESC survey (Factors de Risc en Estudiants de Secundària), which is carried out every 4 or 5 years in representative samples of the educational centers of the city of Barcelona. The survey is a valuable tool that helps identify the health and health behaviors of the adolescent population schooled in the city. However, this tool also allows us to monitor sexual harassment in the city’s adolescent population. It is essential to continue monitoring the trends in this form of behavior and to improve the tools to better capture all dimensions of sexual harassment and its health-related impact.
Regarding the second point, we believe the educational system to be one of the most powerful agents of socialization, because it can help to perpetuate the gender system and tolerance towards violence or, in contrast, to reduce violence by promoting more equitable and healthy relationship models.
In Catalonia, there are different programs for the prevention, detection, notification, referral, and coordination of situations of child and adolescent abuse in the educational context (Generalitat de Catalunya, nd), as well as the program for prevention, detection, and intervention in the face of school harassment of LGBTI people (Departament d’Educació, Generalitat De Catalunya, 2017). However, these programs are insufficient to address sexual harassment. Consequently, the Agència de Salut Pública de Barcelona designed a strategy to prevent violence by promoting equitable and healthy relationships at different educational levels in schools in the city of Barcelona (Pérez et al., 2023). The characteristics of this strategy are: (1) use of a participatory approach to ensure the quality and coherence of the process; (2) creation of a theoretical framework for the strategy; (3) use of intervention mapping methodology as a strategy for the diagnosis, planning, design, development, and evaluation of interventions to promote equitable and healthy relationships; and (4) adaptation or design and evaluation of various programs to incorporate different educational stages.
The strategy plans interventions to promote equitable and healthy relationships framed within a global educational strategy that starts in early childhood education and continues through all stages of compulsory education. Moreover, a conceptual framework has been designed to enhance understanding of the determinants of interpersonal-relational models (Forcadell-Díez et al., 2023).
Footnotes
Authors’ contributions
M.B.-A. and Gloria Perez conceived the original idea of this study and drafted the first version of the manuscript. B.B.L.-G., L.F.-D., V.E.-F., and G.S. contributed significantly to the study design and analysis and discussion of the results. M.J.L., C.V.-C., and B.S.B. contributed to the final version with a critical revision of the manuscript. All authors have read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by Carlos III Health Institute as intermediate from FEDER and FSE in the multicentric project “Promoción de activos protectores de la violencia de género en la adolescencia y pre-adolescencia” (2019–2021) (PI18/00590 and PI18/00544).