
Abstract
The burden of ischemic heart disease has increased globally. In India, the estimated prevalence of angina was around 3.7%. Chronic coronary syndrome, angina pectoris, occurs from an imbalance between oxygen supply and demand in the myocardium. Current antianginal therapies include beta-blockers, calcium channel blockers, nitrates, potassium channel openers, and statins to alleviate symptoms of angina, reduce recurrence, and improve quality of life. Despite conventional therapy, patients remain symptomatic. Hence, there is a need for a new treatment that modulates cardiac energy metabolism and provides promising outcomes in patients with chronic coronary syndrome. Trimetazidine is a metabolic modulator that improves cardiac metabolism by shifting the energy source toward glucose during myocardial ischemia. In this case-based review, we present the role of trimetazidine through hypothetical clinical case scenarios and the clinical evidence of trimetazidine to understand the ideal patient profile. Clinical studies of trimetazidine have demonstrated efficacy in reducing angina frequency, nitrate usage, and improving exercise duration in patients with angina. Trimetazidine could be beneficial as an add-on therapy in patients with chronic coronary syndrome who are inadequately controlled by beta-blockers alone or in combination with other antianginal drugs. Furthermore, trimetazidine is well-tolerated and has been shown to provide survival benefits. Overall, this review could aid practitioners in the use of trimetazidine for different patient indications in clinical cardiology settings in India.
Introduction
Cardiovascular diseases (CVDs) are the leading cause of death worldwide. 1 Ischemic heart disease accounted for half of CVD fatalities. 2 Chronic coronary syndrome (CCS), known as angina pectoris, is the most common symptom of ischemic heart disease and is characterized by pain and discomfort in the heart. 3 The global prevalence of angina was lower in individuals aged <60 years (3.8%) versus those aged >60 years (9.5%) and fivefold greater in males versus females. 4 Moreover, individuals with stable angina pectoris had 3%-4% of annual incidence of myocardial infarction (MI). 2 In India, the prevalence of CCS was estimated to be 1.1%-7.5% in urban areas versus 2.1%-3.7% in rural areas. 5
Angina is caused by episodes of myocardial ischemia, owing to an imbalanced oxygen supply and oxygen demand to the heart. Systemic factors, such as changes in heart rate (HR), muscle contractility, and ventricular size and pressure, can lead to an increase in oxygen demand, whereas coronary factors, such as atherosclerotic coronary plaque or conditions like anemia, can lead to a decrease in oxygen supply.2, 6 Stable (typical) angina occurs as pain during exercise or stress and follows a predictable pattern. Unstable angina occurs as pain with/without physical exertion and does not follow a consistent pattern. Furthermore, vasospastic angina, Prinzmetal angina, or variant angina, is rare and results from spasm of the heart muscles. 3 Trimetazidine is beneficial for CCS, particularly in certain subgroups of patients, such as those with post-MI, those with left ventricular dysfunction, and diabetic patients. It enhances myocardial efficiency and restores the oxygen supply–demand balance, potentially lowering post-MI mortality. In patients with left ventricular dysfunction or heart failure with reduced ejection fraction, trimetazidine improves functional capacity without adverse hemodynamic effects. Additionally, it may shift energy metabolism toward glucose oxidation in diabetic patients, leading to better functional outcomes. These findings support the use of trimetazidine in selected CCS populations.7, 8
Treatments for angina are targeted to reduce angina episodes, provide symptomatic relief, prevent recurrence, and improve patients’ quality of life (QoL). 13 Statins, antiplatelet agents, vasculoprotective renin–angiotensin–aldosterone system inhibitors, and beta-blockers (BBs) have been shown to be effective in reducing the rates of cardiovascular events and improving survival, whereas antianginal drugs tend to offer symptomatic angina relief and have been shown to prevent cardiovascular events in patients with CCS. 14 Despite conventional hemodynamic therapy such as BBs, calcium channel blockers (CCBs), and long-acting nitrates (LANs), some patients remain symptomatic. Moreover, the combination of hemodynamic drugs does not seem to enhance antianginal efficacy. Hence, there is a need to consider medical therapy with a unique mechanism of action. 7
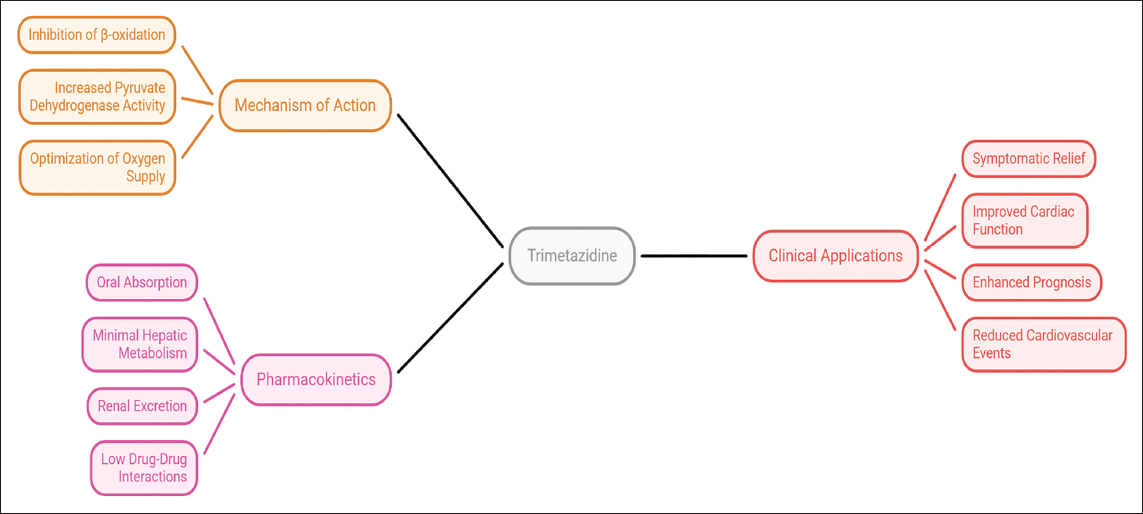
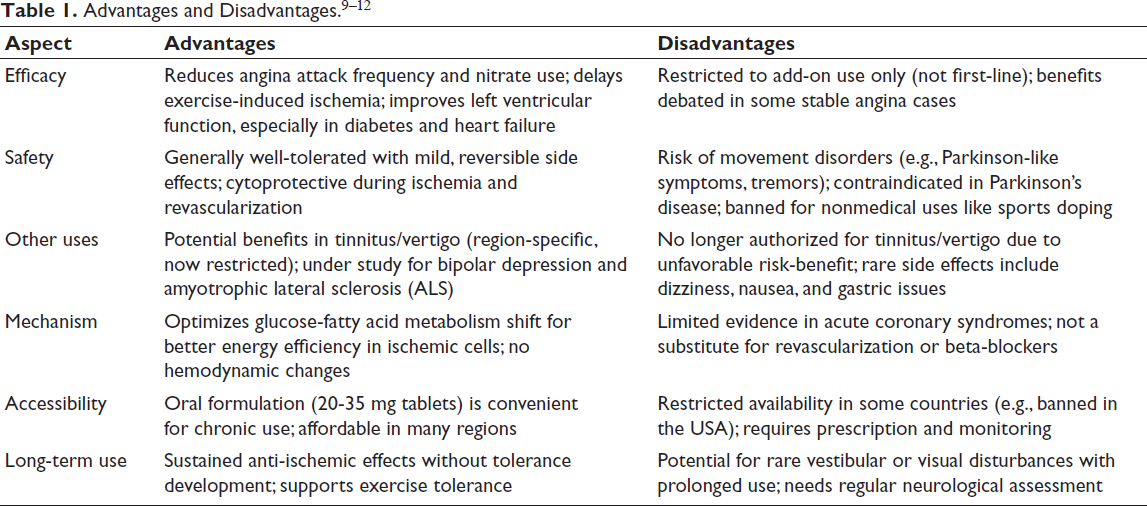
Trimetazidine is a metabolic modulator used as an antianginal drug, which has direct action at the myocardial cell level. It inhibits the intracellular β-oxidation pathway via suppression of the mitochondrial 3-ketoacyl CoA thiolase enzyme; thereby, cardiac cell metabolism shifts from fatty acid oxidation to glucose oxidation.10, 15, 16 Additionally, trimetazidine restores homeostasis between glucose oxidation and glycolysis by increasing pyruvate dehydrogenase activity (Figure 1). This optimizes diminished cardiac oxygen supply and preserves the integrity and function of the cardiac cells during ischemic episodes. 16 Furthermore, the adjunct trimetazidine to conventional medical therapy has been shown to improve symptoms, cardiac function, and prognosis without causing negative hemodynamic effects.10, 12, 16-18 Modulating cardiac energy metabolism by reducing fatty acid oxidation and/or increasing glucose oxidation represents a promising approach in treating patients with CCS. This case-based review presents the role of trimetazidine in patient profiles using hypothetical clinical case scenarios and the clinical evidence of trimetazidine to understand the ideal patient profile. Trimetazidine is a unique cytoprotective metabolic agent that differs from standard antianginal therapies. It is quickly absorbed after oral intake, avoids significant hepatic metabolism, and has a low risk for drug–drug interactions. Its primary excretion route is renal, necessitating caution with renal impairment. Trimetazidine has minimal interactions with common cardiovascular medications, making it a safe addition for patients with chronic stable angina (CCS). Its favorable pharmacokinetics and hemodynamic neutrality enhance its tolerability among diverse patient groups (Table 1 and Figure 2).19, 20
Mechanism of Action of Trimetazidine and Its Clinical Applications.
Trimetazidine’s Role in Angina Management.
Role of Trimetazidine in Patients with Persistent Angina
A Case 1 with Symptomatic Chronic Stable Angina Despite Being on Beta-blockers
A 65-year-old male with angina attacks during daily activity presented to the cardiology department. He had chronic stable angina for the last 2 years. His current medications included metoprolol succinate 50 mg twice daily, atorvastatin 40 mg once daily, aspirin 75 mg once daily, and clopidogrel 75 mg once daily. He had diabetes and was prescribed metformin 500 mg twice daily, teneligliptin 20 mg once daily, and pioglitazone 15 mg once daily to maintain glycated hemoglobin (HbA1c) of 6.5%. He was a non-smoker and had no other risk factors. His other clinical examinations and basic laboratory investigations were normal. His blood pressure (BP) was 110/70 mm Hg and HR was 60 bpm. Despite taking an optimal dose of BBs, the patient continued to experience symptomatic angina. To manage angina, the physician decided to up-titrate his antianginal therapy, prescribing trimetazidine 80 mg once daily and a sublingual short-acting nitrate (SAN) as needed.
More than 75% of patients with stable angina are prescribed conventional antianginal therapy, including BBs. 21 However, the cause of angina could be multifactorial, and patients may require multiple drug therapy to reduce angina symptoms and improve QoL. Evidence showed that trimetazidine as an add-on therapy ameliorates angina symptoms by shifting myocardial metabolism from free fatty acid oxidation to glucose oxidation and reducing oxygen demand. 16 The Modus Vivendi observational study assessed the effect of the addition of trimetazidine 80 mg once daily (OD) to conventional antianginal agents in 1,939 patients (mean age 65.6 ± 8.8 years) experiencing persistent angina despite receiving conventional antianginal therapy. Trimetazidine as an add-on to BBs and as a double or triple combination with other hemodynamic agents such as CCBs and LAN significantly reduced angina attacks (from 6.2 ± 6.5 angina attacks/week to 1.58 ± 2.63 angina attacks/week, P < .05) over a 3-month follow-up period. 16 Additionally, consumption of SAN was significantly (P < .00001) reduced, and patients showed improvement in physical activity and good adherence to therapy after 1- and 3-month follow-up. 16 The ODA study, an observational, multicenter, prospective study in 3,066 patients (mean age 62.8 ± 7.3 years) from Russia, reported the efficacy and tolerability of trimetazidine 80 mg OD as an add-on to antianginal treatment in terms of significant reduction in angina attack frequency from 4.7 ± 3.5 to 0.9 ± 1.3/week (P < .001). Moreover, the majority of physicians rated the tolerability and effectiveness of therapy as “very good.” 22
Role of Trimetazidine as Add-on Therapy
A Case 2 with Symptomatic Angina Despite Triple Hemodynamic Therapy
A 58-year-old male patient with moderate obesity presented to the cardiology department with a complaint of angina during daily activities. With a medical history of chronic stable angina for the last 8 years, he was on a regimen of maximum tolerated doses of LANs, BBs, CCBs, statin, and antiplatelet drugs. He had no risk factors, except a history of dyslipidemia. He quit smoking for the last 5 years. Clinical examination and basic laboratory investigations were normal. His HR was 65 bpm, and BP was 104/70 mm Hg. Despite standard pharmacotherapy, he experienced constant symptomatic angina and was unwilling to undergo coronary angiography or revascularization. Therefore, along with his current therapy regimen, trimetazidine 80 mg once daily was added to manage angina symptoms.
Hemodynamic agents such as nitrates, BBs, and CCBs play a crucial role in managing angina by reducing HR, relaxing blood vessels, and improving blood flow to the coronary arteries. Prolonged use of nitrates can result in tolerance. 23 Whereas trimetazidine, a hemodynamically neutral agent, 10 enhances adenosine triphosphate (ATP) production by changing the myocardial energy substrate, increasing myocardial blood flow, and improving oxygen demand. 23 Hence, combining trimetazidine with hemodynamic drugs can be beneficial. 10 In an observational, prospective, comparative study in South India, 100 patients with coronary artery disease and a history of smoking or hyperlipidemia, when administered trimetazidine 30 mg twice daily along with standard treatment, showed a significant (P < .05) reduction in total cholesterol, triglyceride levels, and systolic BP, with fewer side effects and no reported deaths compared to standard treatment after 6 months. 24 The CHOICE-2 multicenter, open-label, prospective, observational study included 741 patients with angina who had stable angina for 4-9 years and assessed trimetazidine 35 mg twice daily as an add-on to antianginal therapy in a real-world setting. 25 The study demonstrated that trimetazidine reduced angina attacks, decreased the need for SAN (by 1.5 times), increased angina-free walking distance, and improved patient well-being. These effects were observed at the earliest 2 weeks and were maintained throughout 6 months of follow-up, regardless of angina duration. These findings suggest that combining standard therapy with trimetazidine could optimize angina treatment. 25
Role of Trimetazidine in Patients Who are Inadequately Controlled with Beta-blockers
A Case 3 with Chronic Stable Angina Intolerant to Hemodynamic Drugs
A 75-year-old male patient with chronic stable angina presented with a complaint of constant headaches. He had comorbid conditions such as bronchial asthma, hypertension, hypothyroidism, and diabetes with normal renal function. He was on an antianginal regimen of LAN, nicorandil, and amlodipine. His BP was 130/74 mm Hg, and HR was 90 bpm. Clinical and systemic examinations, as well as basic laboratory investigations, did not reveal any abnormalities. He could not tolerate BBs due to asthma. The patient experienced side effects with LANs and amlodipine; hence, these drugs were discontinued. He was subsequently prescribed trimetazidine 80 mg once daily, diltiazem extended release 90 mg once daily, telmisartan 40 mg once daily, nicorandil 5 mg twice daily, atorvastatin 40 mg, and clopidogrel 75 mg to manage angina and BP.
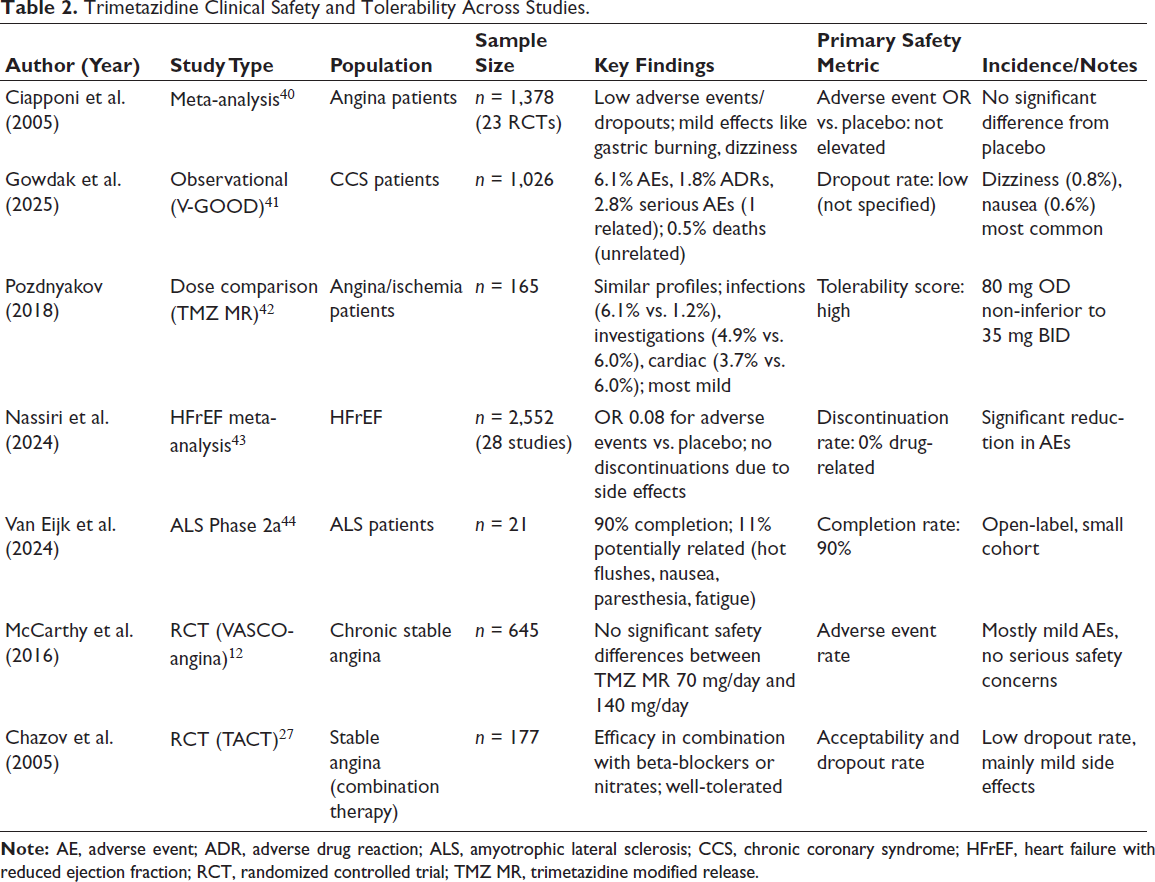
Patients with stable angina are often effectively managed with monotherapy or combination therapy using BBs or CCBs. However, those with comorbid conditions such as hypertension and diabetes may remain symptomatic. 26 In such cases, trimetazidine can be used as an add-on therapy to improve oxygen supply by shifting cardiac cell metabolism toward glucose oxidation without having an impact on HR and BP in patients.26, 27 The TACT (Trimetazidine in Angina Combination Therapy) study, a randomized, placebo-controlled, multicenter trial, evaluated trimetazidine combination versus conventional therapy in patients (n = 177) with stable angina who were resistant to nitrates or BBs. 27 The study reported an increase in exercise test duration and a decrease in the mean number of angina attacks per week (5.6 ± 0.6/week to 2.7 ± 0.5/week) after adding trimetazidine to the conventional regimen. Additionally, the usage of SAN and LAN decreased in these patients. 27 A double-blind, randomized, placebo-controlled trial evaluated the efficacy of the combination of trimetazidine and diltiazem and reported improvement in male patients (n = 64) with stable angina. The combination therapy reduced the cellular metabolic consequences of ischemia without affecting renal function, blood glucose, or plasma lipids. Further, this combination did not show adverse hemodynamic side effects such as reflex tachycardia, hypotension, bradycardia, fatigue, and overt left ventricular failure or atrioventricular block. 28 Another randomized, double-blind, placebo-controlled study with 50 patients investigated the efficacy of the combination of low-dose diltiazem with trimetazidine and reported substantial additive symptomatic control with infrequent side effects. 29 Furthermore, trimetazidine as an adjunct to nicorandil showed improved clinical efficacy and overall treatment rate in patients with coronary heart disease. 30 These findings suggest that combining trimetazidine with conventional therapies could be a promising alternative for managing stable angina, particularly in patients who do not respond adequately to conventional therapy (Table 2).
Trimetazidine Clinical Safety and Tolerability Across Studies.
Clinical Safety and Tolerability of Trimetazidine
Patients with angina might be inadequately controlled on antianginal therapy owing to hemodynamic intolerance or chronotropic incompetence. Trimetazidine, a cytoprotective drug, can be added to first-line antianginal drugs to improve treatment outcomes. 11 Clinical studies, such as TRIMPOL I, TRIMPOL II, and the VASCO (Efficacy of trimetazidine on functional capacity in symptomatic patients with stable exertional angina), demonstrated that combining trimetazidine with BBs is an effective and well-tolerated therapy in patients with symptomatic angina.31-34 A meta-analysis of 12 randomized trials by Marzilli and Klein confirmed the efficacy and tolerability of trimetazidine, both as monotherapy and as combination therapy with conventional antianginal agents. 35 Long-term safety of trimetazidine and its benefits in the therapeutic armamentarium of stable angina were also reported in clinical evidence.36, 37 The METRO (Management of angina: a retrospective cohort) study reported that adding trimetazidine to antianginal treatment for stable angina significantly reduced 6-month mortality after MI. 38 Early combination of metabolic agent trimetazidine to standard therapy consisting of nitrates, BBs, calcium channel antagonists, and/or nicorandil is likely to alter the oxygen demand–supply balance, which may confer a survival benefit in the management of stable angina. 38 The most reported adverse event with trimetazidine includes gastrointestinal disturbance such as nausea, gastric burning, anorexia, and constipation; however, these incidences were generally low.19, 35 A recent systematic review reported that elderly patients treated with trimetazidine for angina experienced Parkinsonism, which was reversible upon discontinuation of trimetazidine. Therefore, while using trimetazidine therapy, it is advisable to examine patients, especially the elderly and those with preexisting neurodegenerative diseases, for Parkinsonian symptoms. However, the mechanism behind such adverse events remains unclear. 39
In the European Society of Cardiology (ESC) 2024 Guidelines for CCS, trimetazidine is recommended as a second-line metabolic agent with a Class IIb indication for symptomatic angina relief. It optimizes myocardial energy metabolism by inhibiting fatty acid oxidation, promoting glucose utilization for greater efficiency during ischemia, without significant hemodynamic changes, making it suitable for patients intolerant to BBs or CCBs.45-47
Practical use involves add-on therapy at 35 mg modified-release twice daily after optimal first-line treatment fails to control symptoms or exercise tolerance. It reduces angina frequency, nitrate consumption, and ischemia time in clinical trials, particularly benefiting diabetics or those with heart failure, where left ventricular (LV) function improves. Peri-percutaneous coronary intervention (PCI) use shows cytoprotective effects against reperfusion injury.7, 45, 47
However, guidelines emphasize that it does not replace revascularization or core therapies like BBs and contraindicate it in Parkinson’s disease due to extrapyramidal risks requiring neurological monitoring. Dose adjustments are needed in renal impairment. Evidence from meta-analyses indicates benefit in unstable angina, but its role is limited to adjunctive use. Overall, trimetazidine supports symptom management in select CCS cases per PubMed-sourced ESC-aligned evidence.7, 8
Conclusion
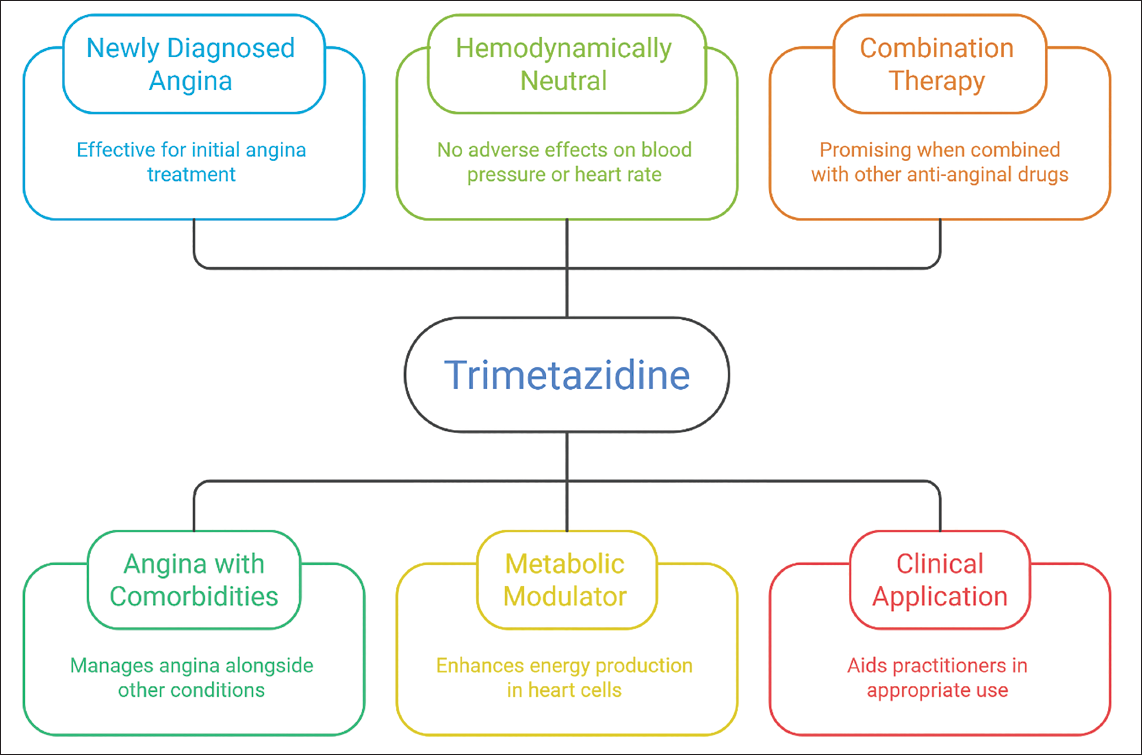
This review article summarizes the role of trimetazidine in different patient profiles, such as newly diagnosed angina and angina with comorbidities. Evidence showed that trimetazidine is effective and well-tolerated in the management of angina in patients with CCS.7, 25, 38, 48 In addition to being a metabolic modulator, trimetazidine is hemodynamically neutral and has no adverse effects on BP or HR, unlike other antianginal drugs. 10 Studies suggest that it could be a promising drug as combination therapy in patients with CCS whose symptoms are inadequately controlled with BBs alone or in combination with other antianginal drugs.16, 27, 31-33 Overall, this review aids practitioners in understanding the appropriate use of trimetazidine in various patient profiles seen in routine clinical cardiology settings in India.
Footnotes
Acknowledgement
We would like to acknowledge Smolt Life Sciences LLP for Editorial support.
Authors’ Contributions
R. B. conceived the review, performed the literature search, drafted the manuscript, and created tables/figures. V. D. and A. B. screened citations, extracted data, and revised the draft. All authors approved the final version and agree to be accountable for all aspects of the work.
Data Sharing Statement
All data analyzed are publicly available in the cited references; no new data were generated.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not required (literature-based review).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Not applicable.