
Abstract
Bioresorbable vascular scaffolds offer temporary mechanical support and local drug delivery to coronary arteries, ultimately restoring native vessel physiology after resorption. This case describes a 62-year-old man who underwent percutaneous coronary intervention with a second-generation sirolimus-eluting MeRes100 scaffold for significant proximal left anterior descending artery stenosis. Four years post-implantation, the patient remained asymptomatic but presented with intermittent, atypical chest pain. Coronary computed tomography angiography revealed complete scaffold resorption and preserved vessel patency, though interpretation was complicated by blooming artefacts from residual metallic markers. Second-generation scaffolds like MeRes100 show improved mechanical properties, predictable bioresorption profiles, and excellent clinical outcomes, including low rates of thrombosis and restoration of vasomotion. This case highlights both the long-term safety and efficacy of MeRes100 and the limitations posed by imaging artefacts, emphasizing the need for cautious computed tomography interpretation after scaffold resorption.
A 62-year-old male presented with exertional dyspnea. Angiography revealed significant proximal left anterior descending (LAD) artery stenosis. Despite optimal medical therapy, symptoms persisted, and percutaneous coronary intervention (PCI) was performed with a MeRes100 second-generation sirolimus-eluting bioresorbable vascular scaffold (BRS). The patient remained asymptomatic for 4 years post-procedure.
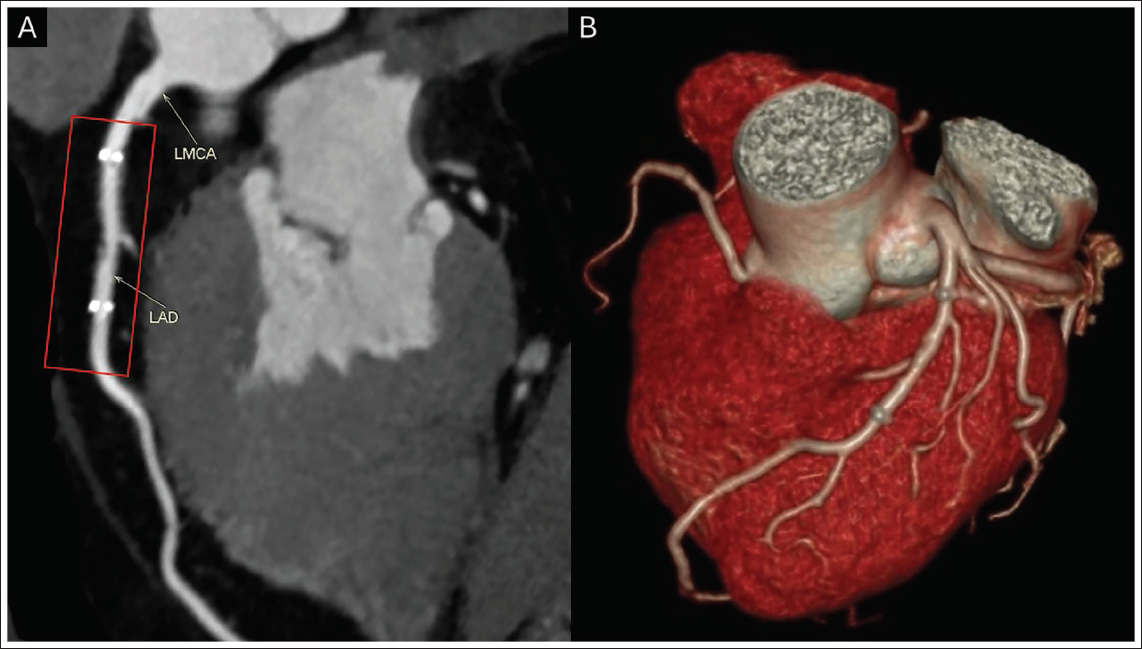
Recently, he reported intermittent, atypical chest pain. An electrocardiogram (ECG) showed no significant abnormalities. To assess for ischemia, a coronary computed tomography (CT) angiogram (Figure 1) was performed, revealing complete scaffold resorption with no significant luminal narrowing. However, blooming artefacts were observed at the site of the proximal and distal scaffold markers, making interpretation challenging.
(A) Multiplanar Reconstructed Image from Multi-slice Computed Tomography (MSCT) Showing Patent Scaffolded Segment (Red Rectangle). (B) Volume-rendered Image Showing Blooming Artefact from the Metallic Markers Along with Patent Scaffolded Segment.
Bioresorbable vascular scaffolds were designed to provide transient vessel scaffolding and drug delivery, while ultimately allowing the restoration of native vessel physiology. 1 Unlike metallic stents that remain permanently, BRS degrade over time, leaving the artery free of foreign material. Second-generation scaffolds, like MeRes100, have addressed the shortcomings of earlier devices with improved deliverability, radial strength, and more predictable resorption profiles. 2 Their theoretical advantages include restoration of vasomotion, late lumen enlargement, and a potentially reduced risk of very late stent thrombosis, though their use is currently reserved for selected patient populations. 3
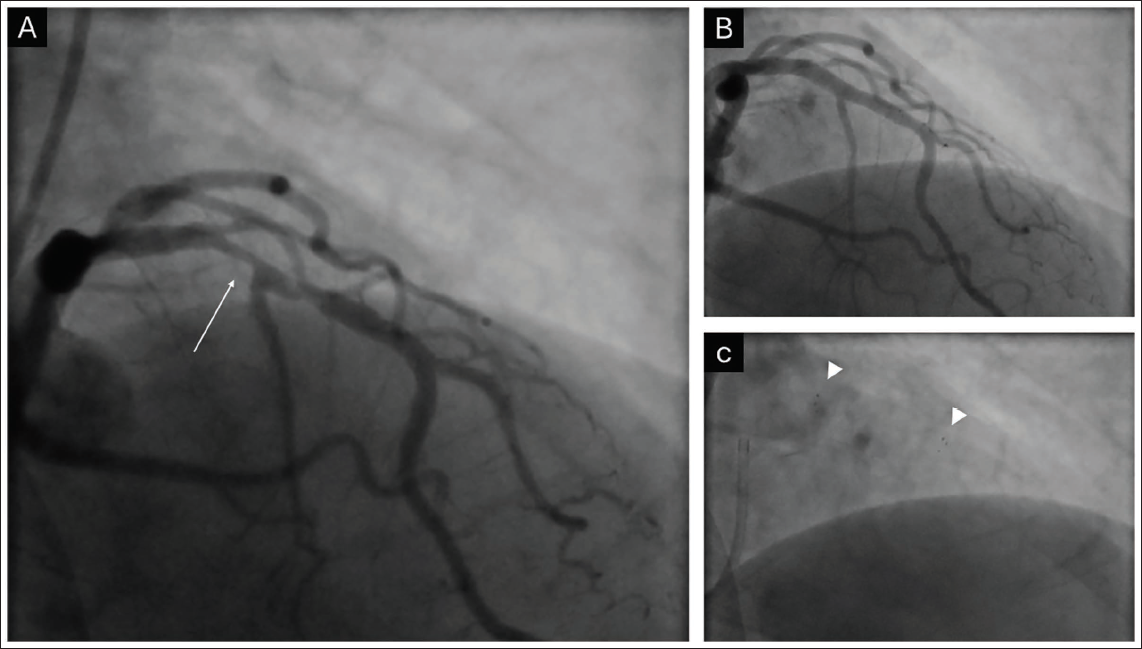
This case demonstrates long-term successful outcomes with BRS and highlights CT blooming artefacts as a limitation in non-invasive assessment post-resorption (Figure 2A-2C).
(A) Coronary Angiogram Showing Significant Narrowing (Arrow) in mid-Left Anterior Descending (LAD) Artery. (B) Percutaneous Coronary Intervention to LAD with MeRes 100. (C) Cine Image Showing the Proximal and Distal Markers (Arrowheads) of the Stent.
Footnotes
Acknowledgment
The authors acknowledge that this article has not been published in any other scientific journal.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval and Patient Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.