
Abstract
Vieussens’ arterial ring is a persistent embryological communication between the proximal right coronary artery and the left anterior descending artery (Germing & Mugge, 2003, Clin Cardiol, 26, 9, 441). Although this vascular connection normally regresses, it remains present in approximately 48% of individuals. In rare circumstances, Vieussens’ arterial ring may function as an important collateral channel (Hansen & Merchant, 2006, Circulation, 114, 16, e545-e546). We report two cases in which complete ostial occlusion of the left anterior descending artery was effectively compensated by the Vieussens’ arterial ring, thereby preventing the occurrence of myocardial infarction.
Introduction
The proximal epicardial connection between the right coronary artery (RCA) and the left anterior descending artery (LAD) was first described by Raymond de Vieussens in 1706. 1 This anatomical structure, later termed the Vieussens’ arterial ring (VAR) in the nineteenth century, represents a remnant of the embryonic conotruncal vascular ring. Under normal physiological conditions, pressures within the RCA and LAD systems are comparable, resulting in minimal or absent blood flow through the VAR.2, 3 However, when significant stenosis develops in either coronary artery, a pressure gradient may arise, leading to progressive enlargement of the VAR and enabling collateral perfusion to the compromised vessel, which can be clinically life-saving.4, 5
Coronary artery development during embryogenesis involves contributions from both distal and proximal vascular components. Initially, a primitive vascular plexus forms within the interventricular and atrioventricular grooves and subsequently establishes connections with the extracardiac great vessels. As development progresses, selective regression and persistence of these vessels shape the definitive coronary anatomy. By approximately the 9th week of gestation, the distal coronary vascular network induces the formation of coronary buds within the truncus arteriosus. Concurrently, the proximal epicardial coronary plexus expands circumferentially around the truncus, creating a vascular ring. As the truncus divides into the aorta and pulmonary artery, rapid connections are established, predominantly with coronary buds arising from the sinuses of Valsalva adjacent to the pulmonary trunk. 6
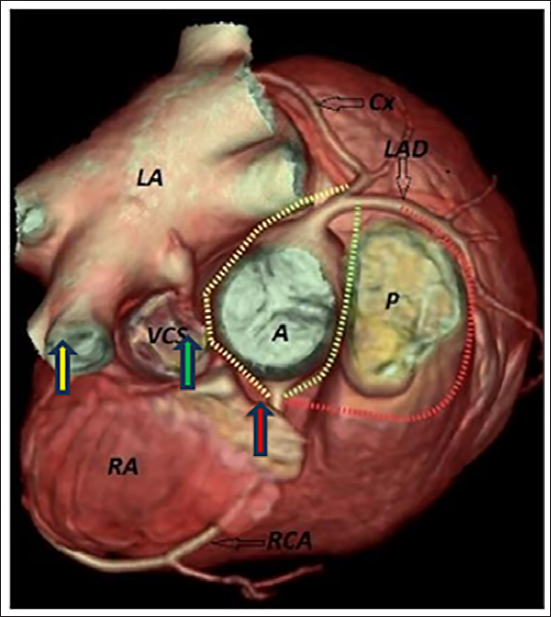
During embryonic development, three principal collateral pathways exist between the right and left coronary systems. The first is the VAR, which connects the conus branch of the RCA to the proximal right ventricular branch of the LAD. The second pathway is the Kugel artery, linking the atrioventricular nodal branch of the RCA with the proximal circumflex artery. The third is the retroconal anastomotic ring, an interarterial connection between the RCA and LAD located between the aorta and pulmonary artery. 7 A schematic representation of these embryonic collateral pathways is shown in Figure 1
Case 1
A 45-year-old female with a history of diabetes and hypertension for 10 years presented with shortness of breath (NYHA Class II) for 1 month and an episode of angina lasting 30 min, which resolved spontaneously. Clinical examination was unremarkable. Echocardiography (ECHO) showed a normal ejection fraction with no valvular abnormalities. Treadmill testing (TMT) was positive for inducible ischemia.
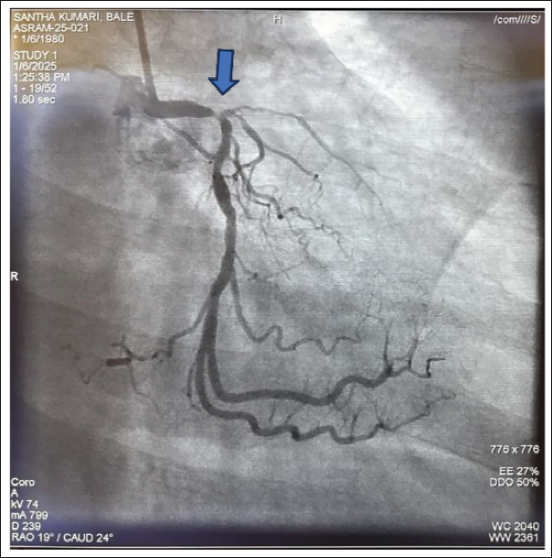
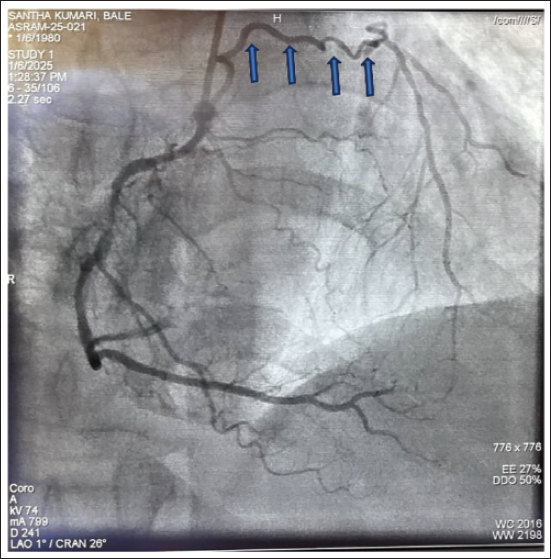
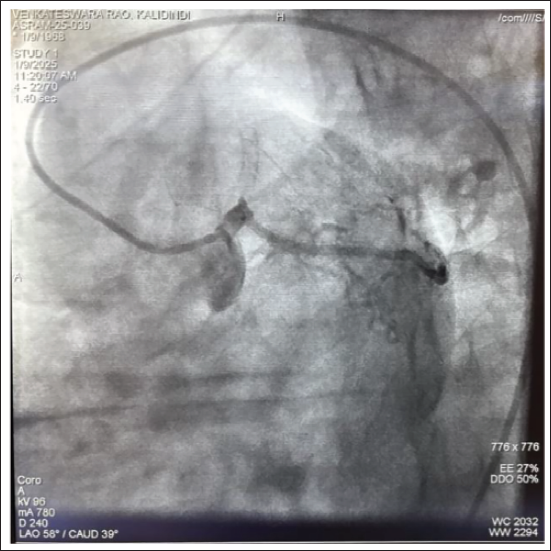
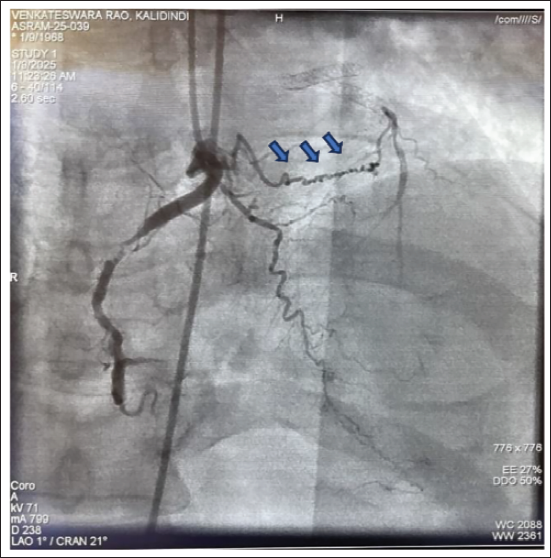
Subsequently, coronary angiography revealed triple-vessel disease with total ostial occlusion of the LAD (Figures 2 and 3). Surprisingly, there were no stigmata of infarction on clinical or imaging evaluations. Detailed angiographic analysis identified VAR as the collateral pathway supplying the LAD territory, thereby preventing ischemic damage (Figures 4 and 5).
Case 2
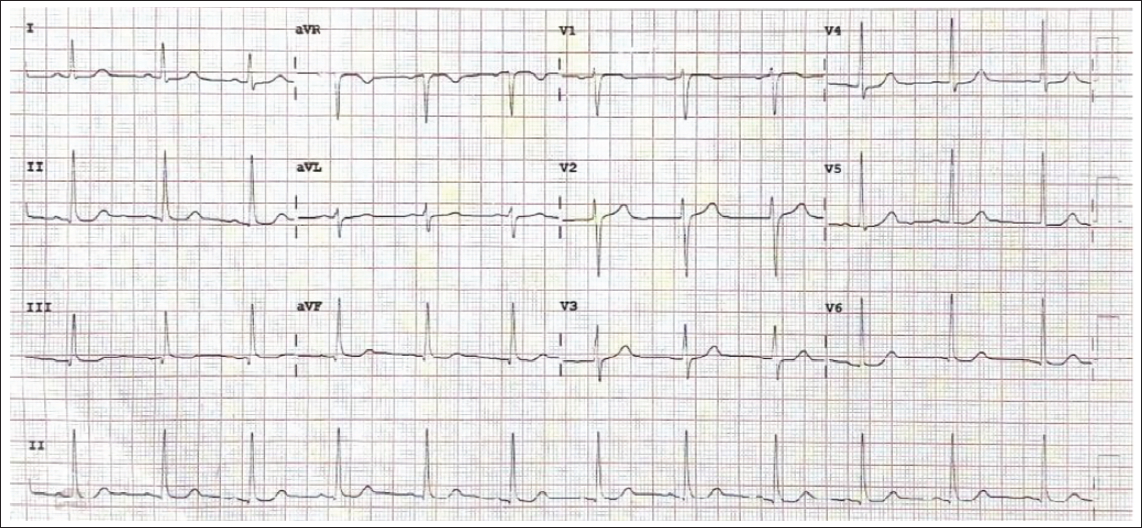
A 55-year-old male patient, type 2 diabetic, hypertensive, CAD-S/P PCI to LAD and LCX 2 years prior, non-compliant to medications, visited the cardiac OPD with complaints of exertional breathlessness (NYHA Class II). His electrocardiography (ECG) showed poor progression of the R wave, and ECHO revealed mild left ventricular (LV) dysfunction. He was initially treated medically. However, due to persistent symptoms, he underwent a coronary angiogram. Coronary angiogram of the patient revealed stent thrombosis of the previous stent and LAD total occlusion from the ostium, as shown in Figure 4. Again, VAR, along with right ventricular (RV) collaterals, come into rescue and fill LAD antegrade, as shown in Figure 6.
Discussion
Vieussens’ arterial ring represents a persistent remnant of the embryonic conotruncal vascular ring and is reported to be present in approximately 48% of the population. Despite this relatively high prevalence, VAR is infrequently identified on imaging studies. A review of 56 documented cases demonstrated a marked male predominance (75%), with clinical presentations ranging from incidental findings to clinically significant contributors in the management of coronary artery disease (CAD). Although Germing and Mügge reported the presence of this embryonic remnant in nearly half of individuals, its detection in routine clinical practice remains uncommon. 2 Doğan et al., using multidetector computed tomography coronary angiography, reported a VAR detection rate of only 3.19%. While published case reports remain limited, the clinical relevance of VAR is increasingly recognized, particularly in patients with CAD, where it may serve as a critical collateral pathway.
Vieussens’ arterial ring is considered a form of collateral circulation that represents a mature, preexisting vascular remnant rather than a newly developed collateral vessel. In adults, its anatomical location corresponds to the site of the embryonic conotruncal arterial ring. Consequently, VAR can be regarded as a persistent conotruncal loop that functions as an anastomotic channel when coronary artery obstruction occurs. Under normal physiological conditions, there is minimal or no blood flow through this structure because pressures within the connected coronary systems are balanced. However, progressive stenosis or occlusion of the proximal RCA or LAD creates a pressure gradient that leads to gradual dilation of the VAR, ultimately enabling perfusion of the compromised coronary circulation. 6
Vieussens’ arterial ring is most commonly detected during coronary angiography, where it appears as a vascular connection between the conus branch of the RCA and the proximal segment of the LAD. Recognition of this anatomical variant is clinically important, as its presence may significantly influence revascularization planning and therapeutic decision-making. Identifying VAR can also alter the perceived severity of coronary lesions and guide appropriate management strategies. In both cases described, complete ostial occlusion of the LAD would typically be expected to result in extensive myocardial infarction with prominent symptoms and hemodynamic compromise. However, collateral perfusion via the VAR maintained antegrade flow within the LAD. Both patients subsequently underwent coronary artery bypass graft surgery.
Conclusion
These two cases highlight the critical role of VAR in preserving myocardial viability in the presence of total LAD ostial occlusion. VAR’s compensatory mechanism underscores its potential life-saving significance in selected cases.
Footnotes
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author, Dr. Sankara Rao Meegada, upon reasonable request and with permission from Madras Medical Mission Hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Patient Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.