
Abstract
Background
Cardiovascular disease ranks as the top cause of mortality globally. The incidence and mortality associated with acute coronary syndrome are increasing in Sri Lanka. There is a lack of extensive data regarding acute coronary syndrome and its treatment in the Sri Lankan population. This study primarily aimed to outline the management trends of acute coronary syndrome at a hospital in Sri Lanka, a tertiary care facility in South Asia.
Method
The acute coronary syndrome registry was designed as a cross-sectional observational study. All individuals diagnosed with acute coronary syndrome were enrolled.
Results
Recruitment for the study began in 2024, with final results expected by the end of 2027.
Conclusion
The acute coronary syndrome registry will offer valuable information regarding patient demographics, local treatment approaches, reasons for not following the recommended guidelines, and clinical outcomes, thereby facilitating further research in this field, creating a national acute coronary syndrome registry in the future, and formulating local treatment guidelines.
Introduction
Globally, cardiovascular disease (CVD) has surpassed infectious disease as the leading cause of death, particularly in South Asia. 1 The 2023 Annual Health Bulletin of Sri Lanka reported that ischemic heart disease is the primary cause of hospital admissions and in-hospital deaths. In 2022 and 2023, government hospitals recorded 66,498 and 67,355 deaths, respectively, with ischemic heart disease accounting for 13% of these fatalities, underscoring its substantial impact on the national health. 2
Acute coronary syndrome (ACS) refers to a spectrum of clinical conditions that include unstable angina (UA), non-ST-elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI). Treatment options include percutaneous coronary intervention (PCI), fibrinolysis, antithrombotic therapy (ATT), and various medications. 3
In low- and middle-income countries, limited availability and access to medical treatment contribute significantly to higher mortality rates. 4 While Sri Lanka has invested considerable resources in acute myocardial infarction (AMI) treatment, including catheterization labs, imaging facilities, pharmacological support, and laboratory services, there is a lack of data on the quality of care in different local hospitals and post-treatment patient outcomes. This highlights the need for a registry and an ongoing hospital monitoring system to improve patient care. Registries play a crucial role in tracking disease progression, characterizing region-specific clinical features and management practices, and highlighting gaps in treatment. 1
National cardiovascular registries exist in 12 (52.2%) of the 23 countries belonging to the Asia Pacific Society of Cardiology, with seven focusing on acute ACS, and five on AMI. These registries serve as crucial benchmarking tools for cardiovascular care and aid in the development of local guidelines. 5
The lack of country-specific data on the demographic, clinical, and biological characteristics of ACS patients in Sri Lanka represents a major limitation, hindering both evidence-based clinical policies and the development of population-specific preventive interventions. Cultural and socio-economic factors significantly influence healthcare-seeking behaviors, treatment adherence, and patient outcomes. Consequently, a study examining ACS in Sri Lanka should investigate these contextual factors to enhance understanding of the challenges and opportunities in delivering optimal care.
This study discusses the establishment of an ACS registry in the university medical unit of the second-largest hospital located in the western province of the country. This registry aims to evaluate current ACS management practices at the Colombo South Teaching Hospital and assess discrepancies between guideline-directed medical treatment (GDMT) and real-time clinical practice. This initiative will serve as a pilot project with plans for the future implementation of similar registries in hospitals across the nation. We are confident that this effort will yield significant data for government authorities, aiding the enhancement of both preventive and curative measures related to the ACS burden in Sri Lanka.
Methods
Study Design
The ACS registry was established as a prospective observational study, including patients admitted with ACS to the University Medical Unit of the Colombo South Teaching Hospital, with follow-up extending to 1 year. The primary aim was to document patterns of ACS management in a tertiary care setting in South Asia.
Study Setting
Colombo South Teaching Hospital ranks as the second-largest medical institution in the nation, with a capacity of 1,281 beds as of December 2024. In 2023, out of 168,451 admissions, 3,751 patients were hospitalized for ACS. Acute coronary syndrome accounts for the second-highest cause of in-hospital mortality, with a reported death rate of 8.23%. These statistics underscore the significance of conducting this study in this particular hospital environment.
Aims and Objectives
This study describes the demographic, clinical, and anthropometric characteristics, and treatment outcomes of patients with ACS. It will also assess the current use of reperfusion therapies, factors influencing invasive management, and discrepancies between recommended medical treatment and actual clinical practice. Additionally, the study will analyze both short-term (less than 1 month) and long-term (12 months) ACS complications, as well as evaluate the existing overall ACS management structure in this unit.
Inclusion and Exclusion Criteria
The requirements for patient inclusion stipulate that individuals must exhibit chest pain symptoms consistent with ACS, and individuals younger than 18 years will be excluded.
The criteria for defining ACS were as follows: STEMI is characterized by chest pain or discomfort, along with persistent ST-segment elevation (lasting 30 min) of ≥0.1 mV in at least two adjacent electrocardiogram (ECG) leads or a presumed new left bundle branch block (LBBB) upon admission, and an increase in cardiac biomarkers (creatine kinase-myocardial band (CK-MB), troponins) with at least one value exceeding the 99th percentile of the upper reference limit. Non-ST-elevation myocardial infarction involves chest pain or discomfort, the absence of persistent ST-segment depression, LBBB, or intraventricular conduction disturbances, and elevated cardiac biomarkers (CK-MB, troponins) with at least one value above the 99th percentile of the upper reference limit. Unstable angina is identified by angina symptoms at rest or with minimal exertion, temporary ST-T changes, and no significant rise in necrosis biomarkers, but with objective evidence of ischemia through non-invasive imaging or significant coronary stenosis observed in angiography. 3
Study Duration
The study’s enrollment process commenced in 2024.
Data Collection
Data will be gathered through a questionnaire administered by an interviewer, and additional investigation results will be sourced from the patient’s previous records and the bed head ticket (BHT). Three to four interviewers, who have been briefed on the process, will collect data. Furthermore, the consultant periodically reviewed the data to ensure consistency and provided feedback to the interviewers for improvement.
Information will be collected at the initial visit (visit 1) and during routine follow-up appointments at 1 month (visit 2) and 12 months (visit 3) (Figure 1). Following discharge from the hospital, the patients were monitored at a monthly medical clinic led by a consultant. All medications were provided free of charge, and the patients were educated on the importance of medication adherence. Invariably, as Sri Lanka has no definite referral pathway, there will be a loss to follow-up.
Flowchart of Study Procedure and Key Data Collection Points.
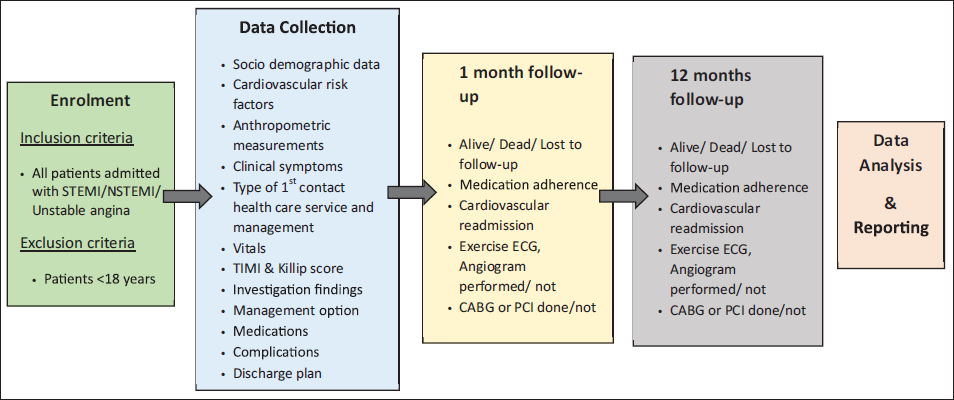
Study Variables
The characteristics of patients will include factors such as age, sex, place of residence, median household income, highest educational level achieved by the time of admission, occupation, ethnicity, and cardiovascular risk factors comprising diabetes, 6 hypertension, 7 dyslipidemia, 8 aspirin use status, smoking habits, significant family history of CVD (having a first-degree relative who experienced either a myocardial infarction or stroke before the ages of 55 for males and 65 for females), prior myocardial infarction, established coronary artery disease (indicated by more than 50% stenosis on computed tomography angiography (CTA), angiogram, or evidence of ischemia on functional cardiac imaging techniques such as nuclear, magnetic resonance imaging (MRI), or echocardiography), chronic stable angina (lasting over 2 weeks), new-onset angina (lasting under 2 weeks), heart failure, 9 renal conditions, chronic lung diseases, 10 cerebrovascular issues, peripheral vascular disease, 11 body mass index (measured in kg/m2 at the time of admission), waist-to-hip ratio, waist circumference, 12 and hip circumference will be gathered.
Factors related to clinical presentation, including the initial complaint, onset and duration of symptoms, promptness in seeking medical attention or any delays, reasons for these delays, type of initial healthcare contact, systolic and diastolic blood pressure readings, heart rate, pulse pressure, thrombolysis in myocardial infarction (TIMI) score, 13 and Killip classification 14 upon admission, as well as values from baseline investigations (CK-MB, troponin T and I, total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglycerides, fasting blood sugar, HbA1c, hemoglobin, serum creatinine, aspartate aminotransferase (AST), alanine aminotransferase (ALT), ECG abnormalities, and left ventricular ejection fraction) will also be collected.
Information will be gathered on the treatment option administered (PCI/thrombolysis), pharmacological treatments provided during hospitalization, and at the time of discharge, and the discharge plan (including plans for angiography, exercise ECG, optimal medical therapy, and cardiac rehabilitation). Instances of complications that arose during the hospital stay (acute heart failure, arrhythmia, cardiogenic shock, stroke, re-infarction, death, and bleeding) will be documented, along with outcomes at 1 and 12 months post-discharge, which encompass whether the patient is alive, deceased, or lost to follow-up, as well as medication adherence assessed using the Morisky Medication Adherence Scale, 15 cardiovascular readmissions due to complications, and whether assessments such as angiograms or exercise ECG, and procedural interventions such as PCI or coronary artery bypass grafting (CABG) were performed.
Data Analysis
Categorical variables were described using proportions and percentages. The central tendency of the numerical variables is represented by the mean, while dispersion is indicated by the range and standard deviation. The associations between categorical variables were evaluated using the chi-square test. Depending on the sample size at follow-up, advanced statistical modeling or machine learning could be explored.
External Validation
At the end of the 3-year study period, we aimed to perform external validation by comparing our dataset with similar cohorts from other South Asian countries. This will help to assess the generalizability and robustness of our findings in broader regional contexts.
Data Dissemination
We plan to disseminate key data and findings to the Ministry of Health to inform and potentially enhance clinical practice and health policy planning in Sri Lanka.
Discussion
Sri Lanka faces substantial health challenges due to ACS. According to the Indoor Morbidity and Mortality Return (IMMR), major non-communicable diseases (NCDs) account for approximately half of the fatalities in government hospitals across the country. Accounting for 12.6% of deaths, ischemic heart disease ranked as the leading cause of mortality. Furthermore, CVDs resulted in the hospitalization of approximately 419,934 patients, making them the most common reason for NCD-related hospital admissions. 2 The factors contributing to these high numbers remain unclear, and investigating the epidemiological and lifestyle aspects of affected patients could be valuable. Currently, Sri Lanka lacks adequate registries, and establishing them at local hospitals would facilitate the collection of essential data.
Several South Asian nations currently maintain ACS registries that provide crucial information. Studies on these registries have shown a higher proportion of male patients and an average age of onset between 65 and 74 years. 16 This observation is consistent with data from Sri Lanka, which report a mean age of 61.3 ± 12.6 years. 17 In the Kerala ACS registry, hypertension (48.4%) was identified as the leading risk factor for STEMI, followed by diabetes and smoking. 18 Similarly, in Sri Lanka, hypertension (45.9%) was found to be the most prevalent risk factor among patients with STEMI. 19
Data from the Severe Cutaneous Adverse Reactions (SCAR) Registry (2011) and the Argentine ST-segment Elevation Acute Myocardial Infarction (ARGEN IAM-ST) Registry (2015, Argentina) reported reperfusion rates of 99% and 96%, respectively, with primary PCI utilized in 89.2% and 95.6% of the cases. 16 In contrast, our region demonstrated lower reperfusion rates. The Kerala ACS registry reported that 41.4% of patients underwent thrombolysis, 18 whereas the Nepal ACS registry showed that 32.7% received reperfusion therapy. 16 The Pakistan ACS registry indicated that 33% received reperfusion, 20 of which also provided data on discharge medications, post-ACS complications (with heart failure being the most common), 16 and clinical outcomes following discharge.
The Acute Coronary Syndrome Sri Lanka Audit Project (ACSSLAP) is the nation’s first large-scale clinical audit, designed to evaluate patient profiles, treatment practices, and clinical outcomes across government hospitals. The findings indicated that more than 90% of patients received aspirin, clopidogrel, and statins during both acute care and discharge. This performance is on par with quality standards in the UK and Europe and exceeds figures reported in other South Asian nations, 19 demonstrating that Sri Lanka’s healthcare system delivers effective pharmacotherapy for ACS, in line with international guidelines.
Nevertheless, in Sri Lanka, fibrinolytics were the primary treatment for most patients with STEMI (63.2%), whereas only a small percentage underwent primary PCI (3.8%). Timely thrombolysis within the first 30 min was achieved in only 42.3% of patients, 18 and a recent study examining AMI care in low- and middle-income countries identified delays and inefficiencies in providing in-hospital interventions as a significant challenge. Additional factors contributing to delayed healthcare seeking included lack of patient education, late diagnoses, inadequate referral systems, limited rural hospital resources, and insufficient funding. 4 To improve healthcare outcomes and guide future interventions, it is imperative to collect extensive data on ACS patients in Sri Lanka, which can be achieved by implementing a national- or hospital-based registry.
Furthermore, the ACS Registry will provide crucial information on patient demographics, regional treatment strategies, factors influencing non-adherence to recommended guidelines, and health outcomes. These data will contribute to advancing research in this field, support the establishment of a nationwide ACS registry in the future, and assist in developing localized guidelines.
Footnotes
Authors Contribution
Anne Thushara Matthias and J. Indrakumar conceptualized the study and drafted the manuscript. Shangavi Navaretnam contributed to the literature search. Chirani Ratnayake and Mahima Suresh contributed to drafting the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the ethics review committee of Colombo South Teaching Hospital, Sri Lanka (No. 2060) on May 15th, 2024.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Informed verbal consent was obtained from the study participants.