
Abstract
Background
Acute coronary syndromes and ST-elevation myocardial infarction remain significant causes of global morbidity and mortality. Despite existing noninvasive risk stratification schemes, ST-elevation myocardial infarction risk prediction requires further characterization. This study aims to assess echocardiographic indices in predicting major adverse cardiovascular events post-ST-elevation myocardial infarction.
Aims and Objectives
Investigate the Tei Index in ST-elevation myocardial infarction and assess its association with major adverse cardiovascular events and coronary lesion severity. Determine if Tei Index, E/e′, and deceleration time independently predict major adverse cardiovascular events in acute ST-elevation myocardial infarction.
Materials and Methods
Conducted at the Department of Cardiology, at a tertiary medical facility from February 2014 to August 2015. Clinical evaluations, laboratory tests, echocardiographic examinations, and coronary angiography were performed among 400 patients. Statistical analyses provided insights into ST-elevation myocardial infarction characteristics and outcomes.
Results
Risk factor prevalence and demographic distribution were highlighted. Left ventricular ejection fraction, Tei Index, deceleration time, and E/e′ ratio exhibited significant associations with clinical severity. Killip class showed a positive correlation, with left ventricular ejection fraction admission (ADM) having an exceptionally high negative correlation. Tei ADM, deceleration time ADM, and E/e′ ADM also revealed significant correlations.
Conclusion
Tei Index, E/e′, and deceleration time are independent predictors of major adverse cardiovascular events in acute ST-elevation myocardial infarction. The Tei Index demonstrated the highest predictive accuracy. Routine Tei Index measurement in acute myocardial infarction patient assessments is advocated for its ease and valuable prognostic insights.
Keywords
Introduction
Acute ST-segment elevation myocardial infarction (STEMI) represents a medical emergency characterized by the sudden occlusion of a coronary artery, leading to compromised blood flow and subsequent myocardial damage. The initial phase of STEMI is critical, requiring timely and accurate risk assessment to guide appropriate therapeutic interventions and improve patient outcomes. Echocardiography, a noninvasive imaging technique, is pivotal in evaluating cardiac structure and function, offering comprehensive insights into the myocardial status postinfarction.
Echocardiography enables the evaluation of both systolic and diastolic left ventricular (LV) functions, which serve as indicators of heart failure (HF). Ejection fraction (EF) is a quantitative measure of LV systolic function, while transmitral inflow patterns, commonly measured using Doppler echocardiography, are important parameters in the assessment of diastolic function. However, both approaches have significant limitations, particularly when evaluating patients with an acute myocardial infarction (MI). An alternative to individually assessing systolic and diastolic functions is the proposal of a single index that may evaluate the overall myocardial performance. 1
In 1995, Tei and colleagues introduced an indicator known as the Tei Index or myocardial performance index (MPI). The same index, which is determined by Doppler echocardiographic measurement, is derived by adding the isovolumic contraction period (IVCT) and isovolumic relaxation time (IVRT), and the total is divided by the ejection time (ET). Furthermore, it has been demonstrated to outperform traditional echocardiographic parameters in terms of its correlation with patient prognosis in different myocardial conditions. Nevertheless, evidence is scarce about the clinical significance of MPI in individuals suffering from acute MI.1–6 Previous research has indicated several factors that might predict major adverse cardiovascular events (MACE) in patients with MI, such as established scoring systems (Global Registry of Acute Coronary Events (GRACE), Thrombolysis In Myocardial Infarction (TIMI), and SYNTAX), the magnitude of the heart attack, and certain echocardiographic measurements. MI causes direct harm and necrosis of the heart muscle cells, resulting in the deterioration of cardiac function. Nevertheless, there is a considerable amount of data available specifically on individuals diagnosed with STEMI alone, which is attributed to a significant proportion of severe initial circumstances. STEMI is classified as a distinct disease entity from non-STEMI (NSTEMI) due to its diverse pathogenesis. STEMI occurs due to a complete and persistent occlusion of the epicardial coronary artery, while NSTEMI arises either due to the severe narrowing of the coronary artery, transient vessel occlusion, or due to the microembolization of a thrombus and/or an atheromatous material. STEMI is defined based on electrocardiogram (ECG) criteria, while NSTEMI is defined based on elevation in the levels of cardiac biomarkers in the absence of ST elevation. 7 Moreover, the use of left ventricular ejection fraction (LVEF) and LV diastolic function to forecast clinical outcomes in STEMI remains a subject of debate. The E/e′ ratio, a Doppler-derived index for the assessment of LV diastolic function, has also been identified as a significant prognostic marker in patients with STEMI. This is because LV diastolic failure develops before LV systolic impairment following myocardial ischemia. 8 Among the many diastolic factors, a decrease in the early filling wave’s deceleration time (DT), which indicates a “restrictive” filling pattern, is associated with larger infarcts and predicts worse outcomes for patients after an MI.9, 10 Thus, we postulated that a reduced DT and increased E/e′ would serve as indicators of a worse prognosis following an acute MI.
This study seeks to comprehensively assess the clinical characteristics and hospital events in patients admitted with acute STEMI. We evaluated the LV filling pressure using echocardiographic color and tissue Doppler E/e′ ratio assessment of the mitral valve. The objective is to evaluate the efficacy of Tei Index, DT, and E/e′ as prognostic markers in patients with STEMI, with or without revascularization treatment, for predicting death during hospitalization and tailor therapeutic approaches accordingly.
Materials and Methods
Ethical Approval and Study Design
In our study, ethical guidelines were strictly observed to ensure accuracy and reliability. All the participants were clearly explained about the study’s aims and provided written informed consent before enrollment.
Patient Selection
This study was conducted at a teaching hospital in the Department of Cardiology at a tertiary medical college and hospital, between February 2014 and August 2015. Approximately 400 subjects were assessed during this study. Based on the clinical examination, patient medical history, and ECG results, the study patients were diagnosed with severe to low-grade MI, particularly ST-segment dilation at inferior leads (II, III, and aVF). A total of 102 patients were selected for this study after a rigorous selection process based on pre-specified criteria.
Inclusion Criteria
Patients were included if they were aged >18 years and had acute MI, ischemic symptoms with ≥0.2 mV, ST-segment elevation in inferior leads, and pathological Q waves in the ECG. Additional inclusion criteria were right ventricular myocardial infarction (RVMI) associated with low levels of MI, namely V4 of V6R lead, which was defined by ST-segment elevation ≥0.1 mV at the center. For an accurate diagnosis, participants had to receive a normal echocardiographic window. Patients were also included if they had a typical rise and/or fall of biochemical markers of myocardial necrosis with at least one of the following: ischemic symptoms, development of pathological Q waves in the ECG, ECG changes indicative of ischemia (ST segment elevation), or imaging evidence of new loss of viable myocardium or new regional wall motion abnormality. In addition, coronary angiography (CAG) confirmed that severe narrowing in the right coronary artery (RCA) was an essential inclusion criterion.
The study included patients aged over 18 years who were diagnosed with acute MI. The criteria for STEMI included a typical rise and/or fall of biochemical markers of myocardial necrosis with at least one of the following features: (a) ischemic symptoms, (b) development of pathological Q waves in the ECG, (c) ECG changes indicative of ischemia, and (d) imaging evidence of new loss of viable myocardium or new regional wall motion abnormality.
Exclusion Criteria
The study did not include patients who denied consent, had prosthetic valves implanted, mitral stenosis or regurgitation, large shunts, atrial fibrillation, or chronic kidney disease (CKD). Additionally, patients with concomitant inflammatory diseases, neoplastic diseases, or any severe uncontrolled systemic disorders were excluded. Patients who died or developed mechanical complications before CAG was performed and those who did not undergo CAG were also not considered for this study.
Clinical Evaluation and Laboratory Tests
A clinical review was first conducted in history and clinical testing to identify signs of RV disorder (RV failure) such as hypotension and increased venous pressure from the jugular vein (JVP), especially when there is a clear lung field. Samples of blood were drawn for laboratory tests to determine complete blood count and lipid profile, including total cholesterol, high-density lipoproteins (HDL), low-density lipoproteins (LDL), as well as triglycerides, random blood glucose, serum urea, and creatinine levels for each patient. Additionally, troponin T was measured to assess myocardial damage.
Conventional Echocardiographic Examination
After initial stabilization, within the first 24 h of hospitalization, all patients were exposed to a comprehensive traditional echocardiographic assessment using the Siemens Accuson Machine CV0 (Siemens Healthineers, Germany). All patients underwent echocardiographic evaluation within 24 h of admission, prior to CAG and any intervention. Exact measurements of mitral inflow dynamics, such as E-wave (E) and A-wave (A) velocities, the E/A ratio, as well as DT, were recorded. LV outflow patterns were scrutinized from the apical five-chamber view, with Doppler profiles analyzed digitally, using an average of three consecutive cardiac cycles. Time intervals were precisely measured from mitral inflow and LV outflow velocity, forming the basis for the Tei Index calculation, expressed as the ratio (a-b)/b, where “a” encompasses IVCT, ET, and IVRT, and “b” signifies LVET.
Septal mitral annular Doppler tissue imaging was performed from the apical four-chamber view using a sample volume of 2-4 mm. From this, e′ was measured. E/e′ ratio was also calculated. LVEF was measured from the parasternal long-axis view by Teichholz’s formula. 11
Right Ventricular Function Parameters
Tricuspid annular plane systolic excursion (TAPSE) measurement was obtained by placing the M-mode cursor over the lateral tricuspid annulus in the apical four-chamber view. Our goal was to quantitatively measure the longitudinal movement of the tricuspid ring on the peak system. Cardiac dynamics were evaluated using pulsed-wave tissue Doppler imaging, with image acquisition being performed through the apical four-chamber view in tissue Doppler mode, focused specifically on the RV free wall. To minimize the effect of translational movement, the Doppler sample volume on the tricuspidal ring at the base of the RV-free wall was placed at the end.
With the help of specific software, a comprehensive velocity profile was generated throughout the cardiac cycle, revealing different peaks and troughs. This evaluation depicted a significant rise in peak systolic velocity (Sm), representing the motion of the annulus toward the apex in systole. Moreover, the initial diastolic myocardial velocity (Em) value is negative, which results in an increase in the ring from the tip. Late diastolic myocardial velocity (Am) readings also depicted negative values afterward. The dynamic patterns of the Sm, Em, and Am waves were nicely demarcated with this analysis. Critical time intervals were meticulously measured to probe deeper into cardiac performance. The extent of the Sm was calculated by employing the ET. The IVRT was calculated from the interval from the end of Sm to the start of Em. Likewise, the interval between the end of Am and the start of Sm provided useful data on the IVCT.
The MPI, a useful index of global cardiac function, was computed according to the formula: MPI = [(IVRT + IVCT)/ET].
Coronary Angiography
Coronary angiography was performed according to the Judkins technique within 24 h of presentation, and decisions regarding PCI or thrombolysis were made thereafter. 12 The study prioritized parameters such as stenosis size, thrombus presence, and TIMI flow, offering a detailed insight into reperfusion dynamics. The intricate TIMI classification, spanning grades 0-3, not only deepened the comprehension of acute MI but also played a pivotal role in clinical diagnosis and intervention planning. The effectiveness of flying pathways in monitoring patients and guiding treatment strategies relied on a comprehensive assessment of these factors.
Follow-up schedule: Patients in this study were observed for a period of up to 30 days after hospital discharge by medical record reviews, OPD visits, or telephone interviews with the patient or their close relative. After discharge, assessments concentrated on the presence of any significant cardiovascular events. Serial measurements of the diastolic parameters were not performed over the follow-up period.
Statistical Analysis
Stata 11.0 (SPSS Inc., Chicago, IL) was used for descriptive statistics in this study. Student’s t-test or Mann–Whitney test (depending on data distribution) was used to compare continuous variables, while the Chi-square test was used for categorical variables. A P value of <.05 was observed as significant. Receiver operating characteristic (ROC) curves were plotted to identify coordinate curves that will point out the sensitivity and specificity of the occurrence of the desired endpoints. Logistic regression analysis was performed to determine how the variables affected the occurrence of the identifier.
Results
Descriptive Statistics of the Study Population
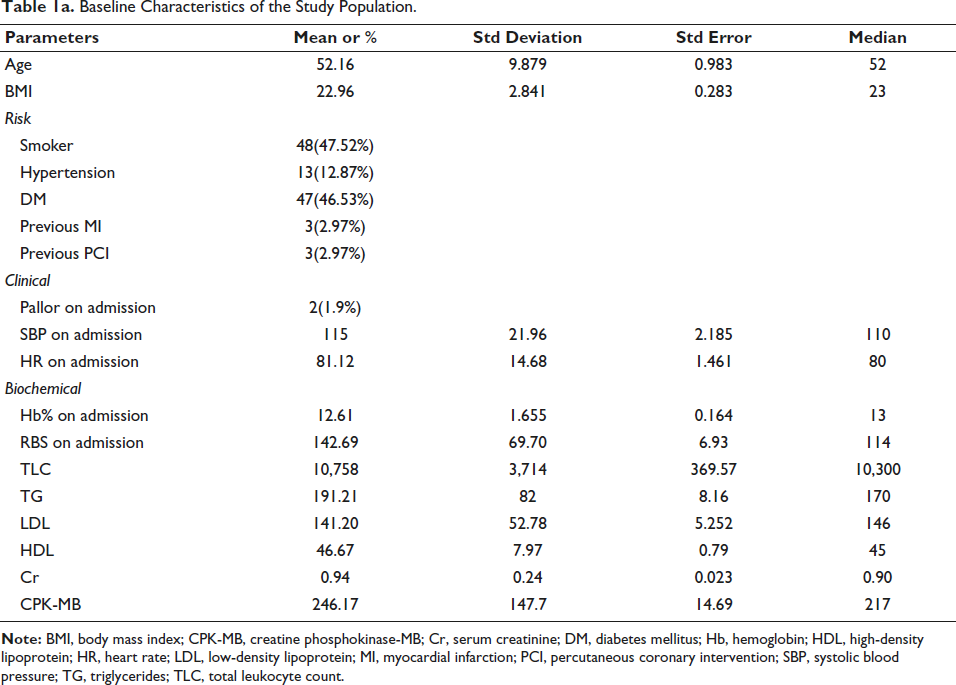
A total of 400 patients were screened during this study. Based on the clinical examination, patient medical history, and ECG results, the study patients were diagnosed with severe to low-grade MI, particularly ST-segment dilation at inferior leads (II, III, and aVF). Ultimately, a total of 101 patients were selected for the study based on a rigorous selection process based on a specific criterion. The demographic parameters, such as age and body mass index (BMI), reflect a mean age of 52.16 years (standard deviation (SD) ± 9.879), and a mean BMI of 22.96 (SD ± 2.841). The prevalence of risk factors, including smoking (47.52%), hypertension (12.87%), diabetes mellitus (46.53%), previous MI (2.97%), and previous percutaneous coronary intervention (PCI) (2.97%), highlights the multifaceted nature of patient profiles. Clinical indicators like pallor on admission (1.9%), systolic blood pressure (mean = 115), and heart rate (mean = 81.12) provide intuition for the initial clinical presentation. Biochemical parameters, including hemoglobin (mean = 12.61), random blood sugar (mean = 142.69), total leukocyte count (mean = 10,758), triglycerides (mean = 191.21), LDL cholesterol (mean = 141.20), HDL cholesterol (mean = 46.67), serum creatinine (mean = 0.94), and creatine phosphokinase-MB (mean = 246.17), contribute to a comprehensive characterization of the physiological status of the patients (Table 1a).
Baseline Characteristics of the Study Population.
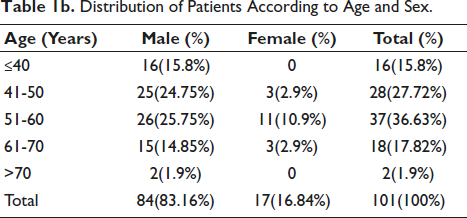
The ages of the participants were grouped into different age brackets (≤40 years, 41-50 years, 51-60 years, 61-70 years, >70 years), and gender information was recorded. Statistical results were summarized to define major tendencies and changes between different age groups (Table 1b). The population number by age groups demonstrates the most arithmetic mass of 51-60 years of age during which the largest part of the cohort represents the age class. Gender gaps show that individuals from about 83.16% of the total sample involved in the project were males. This data also shows excessive female absences in the 71+ age group with evident gender imbalances among the under 40s and a certain less age bracket group.
Distribution of Patients According to Age and Sex.
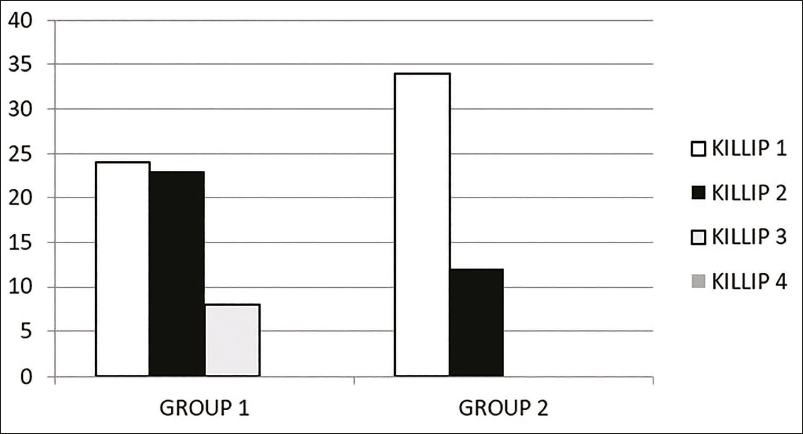
Association of Different Killip Classes Among the Study Population
The Killip classification system is a well-established tool for assessing the severity of HF in patients with acute MI. In this study cohort, the distribution of patients across Killip classes reveals distinct patterns in Group 1 (MACE positive) and Group 2 (MACE negative). In Group 1, a balanced representation is observed across Killip classes; there are 24 patients in Killip 1, as compared to Killip 2 (n = 23), and Killip 3 (n = 8). Notably, no patients in Group 1 fell into Killip 4 (Figure 1). In contrast, Group 2 exhibits a different distribution, with 34 patients in Killip 1, 12 patients in Killip 2, and none in Killip 3 or 4 (Figure 1).
Association of Different Killip Classes Among the Study Population.
The diverse range and variability observed in LVEF, Tei Index, DT, and E/e′ ratio underscore the heterogeneity of cardiac function within the studied cohort. Deviations from the mean in these parameters may indicate potential cardiac health issues or variations in patient profiles. This study provides a detailed characterization of cardiac function parameters in a patient cohort.
In the cardiac function assessment of the studied cohort, LVEF exhibited a range between 30% and 65%, with a mean of 44.93% and SD of 8.710 (Table 2). Similarly, the Tei Index demonstrated variability from 0.27 to 0.95, with a mean of 0.5634 and SD of 0.17715 (Table 2). DT ranged from 89.0 to 214.0 ms, with a mean of 164.663 ms and SD of 26.4618. The E/e′ ratio spanned from 5.90 to 18.90, with a mean of 10.3712 and SD of 3.05526 (Table 2). These findings provide a comprehensive overview of the cardiac parameters, emphasizing the diversity and potential clinical significance within the examined population.
Distribution Pattern of the Important Variables in the Study Population.

Among patients with DT ≥160 ms, 36 out of 59 did not develop MACE, and among those with E/e′ ratio <8, 25 out of 30 had favorable outcomes, highlighting the prognostic relevance of normal diastolic parameters.
The study found a significant association between MACE and increasing age (P value = .002), BMI (P value = .000), presence of diabetes (P value = .04), Killip class at presentation (P value = .002), and ECG showing anterior wall infarct (P value = .006). Additionally, the research established a positive relationship between MACE and some echocardiographic parameters. LVEF, Tei Index, mitral inflow DT, and E/e′ ratio (P value = .000 for all parameters) were all strongly associated with MACE.
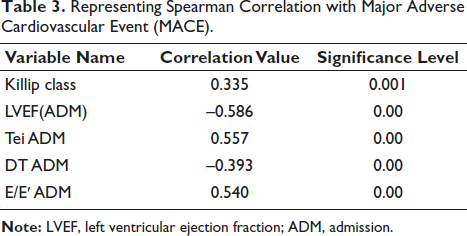
Spearman Correlation with Major Adverse Cardiovascular Events
In this study, we examined the correlation between Killip class and key cardiac parameters, including LVEF, Tei Index (Tei ADM), DT ADM, and E/e′ ratio (E/e′ ADM). The findings reveal significant associations, elucidating the nuanced interplay between clinical severity and cardiac function. Killip class demonstrates a positive correlation (r = 0.335, P = .001), emphasizing its potential as an indicator of clinical severity. LVEF (ADM) exhibits an exceptionally high negative correlation (r = –0.586, P < .001), underscoring its significance as a cardiac function indicator in the context of Killip classification. Tei ADM shows a positive correlation (r = 0.557, P < .001), highlighting its association with clinical severity. DT ADM displays a negative correlation (r = –0.393, P < .001), suggesting its potential as a correlation of clinical presentation (Table 3). E/e′ ADM reveals a positive correlation (r = 0.540, P < .001), implying its role in reflecting clinical severity. These findings contribute to a nuanced understanding of the intricate relationship between cardiac parameters and clinical severity in the context of acute MI.
Representing Spearman Correlation with Major Adverse Cardiovascular Event (MACE).
Receiver Operating Characteristic with Respect to Major Adverse Cardiovascular Events Positive and Negative Patients
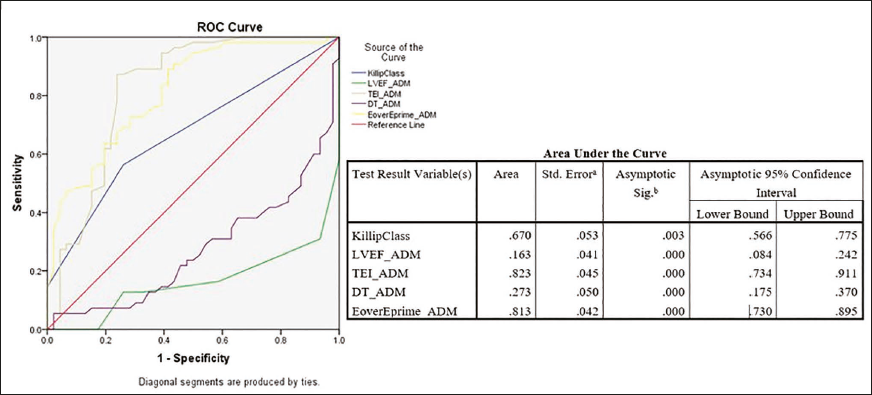
The ROC curve analysis among MACE patients demonstrated that TEI ADM (Tei Index) and E/E′ ADM (E/e′ ratio) exhibited strong abilities with area under the curve (AUC) values of 0.823 and 0.813. It showed significant discrimination between different classes. Killip class demonstrated moderate discriminative ability with an AUC of 0.670, suggesting a moderate capacity to distinguish between various clinical conditions. In contrast, LVEF ADM and DT ADM showed limited discriminative power, with AUC values of 0.163 and 0.273, respectively, indicating challenges in effectively distinguishing between different conditions based on these variables. These nuanced AUC values offer detailed insights into the varying effectiveness of each variable in characterizing clinical severity (Figure 2).
Receiver Operating Characteristic with Respect to Major Adverse Cardiovascular Events Positive Patients.
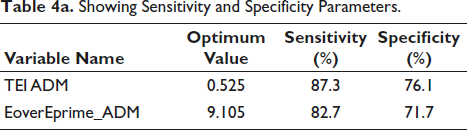
The optimal cutoff values for discriminating clinical conditions were determined for TEI ADM (Tei Index) at 0.525, achieving a sensitivity of 87.3% and specificity of 76.1%, and for E/E′ ADM (E/e′ ratio) at 9.105, with a sensitivity of 82.7% and specificity of 71.7% (Table 4a).
Showing Sensitivity and Specificity Parameters.
Receiver Operating Characteristic with Respect to Major Adverse Cardiovascular Events Negative Patients
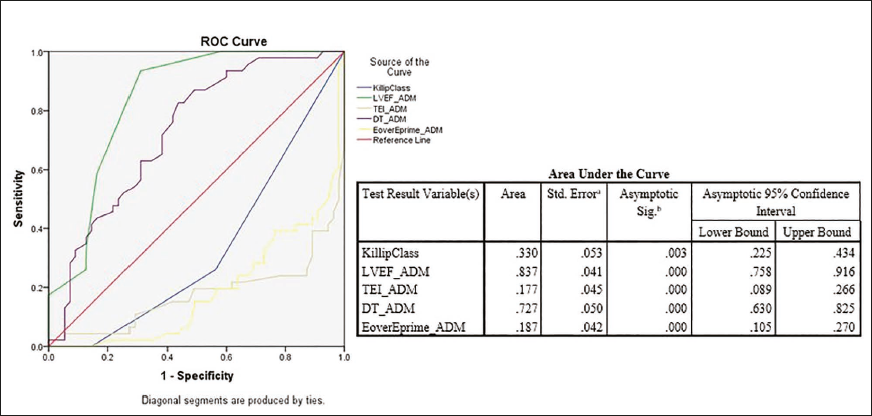
The ROC curve analysis in the non-MACE patients revealed the discriminative performance of various variables: Killip class exhibited a modest discriminative ability (AUC = 0.330), LVEF ADM demonstrated strong discriminative power (AUC = 0.837), TEI ADM showed limited discriminative ability (AUC = 0.177), DT ADM displayed substantial discriminative capacity (AUC = 0.727), and E/E′ ADM exhibited limited discriminative ability (AUC = 0.187) (Figure 3). These findings, along with standard errors and confidence intervals, offer comprehensive insights into the effectiveness of each variable in distinguishing between different clinical conditions.
Receiver Operating Characteristic with Respect to Major Adverse Cardiovascular Events Negative Population.
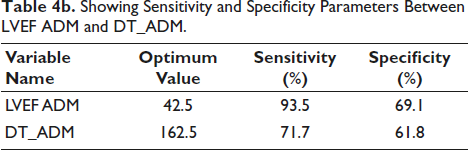
The optimal cutoff value for LVEF ADM was determined at 42.5, resulting in a sensitivity of 93.5% and specificity of 69.1%. In contrast, the optimal cutoff value was 162.5 for DT ADM, yielding a sensitivity of 71.7% and specificity of 61.8%. These findings highlight the trade-off between sensitivity and specificity for each variable at their respective optimum values (Table 4b).
Showing Sensitivity and Specificity Parameters Between LVEF ADM and DT_ADM.
Discussion
Acute MI continues to be a significant cause of illness and death on a global scale. 13 Despite the implementation of various methods to assess risk, there is still a lack of comprehensive understanding regarding the prediction of risk associated with acute MI. 14 The Tei Index is a measure that combines systolic and diastolic dysfunction.
The SAVE Trial investigated the prognostic value of the MPI in post-MI patients with reduced LVEF. In a cohort of 512 patients, an MPI of 0.50 or higher independently predicted adverse cardiovascular events. 14 A subsequent study supported these findings, showing that a Tei Index exceeding 0.40 successfully predicted MACE within 30 days, even in individuals with preserved LV function. This highlights the broad applicability of the Tei Index as a prognostic marker across diverse post-MI patient profiles. However, its potential to predict complications in cases of acute MI is not yet adequately addressed. Echocardiographic indicators of elevated LV filling pressures have been linked to adverse remodeling and an increased occurrence of HF. The DT of early transmitral flow serves as a simple yet powerful tool for predicting these outcomes. An increase in the E/e′ ratio, the ratio between the initial transmitral flow velocity and the initial mitral annular velocity, indicates an increase in LV filling pressure. Another study by Sakaguchi et al. identified anteroseptal MI, infarct size, and re-vascularization procedure as key determinants of LV remodeling, showing significant differences between MACE and no-MACE groups. 15 Therefore, we have formulated a hypothesis that a shortened DT and elevated (E/e′) levels could serve as predictors of unfavorable outcomes following acute MI. Consequently, our plan was to evaluate these echocardiographic indicators to predict MACE subsequent to the initial occurrence of STEMI.
In a study by Poulsen et al., the Tei Index was significantly higher in 64 acute MI patients within 1 h of hospital arrival compared to 39 healthy subjects (P < .0001). Patients with MI and in-hospital congestive heart failure (CHF) had higher Tei Index values than those without CHF. The Tei Index >0.45 was identified as the strongest independent predictor of CHF development in multivariate regression analysis. Our study corroborates these findings, supporting the Tei Index as a predictive marker for CHF in acute MI. 16
Our study was conducted on patients who were admitted to the Cardiology Department of a tertiary care medical college and hospital, between February 2014 and August 2015. An echocardiographic assessment was done within 24 h of admission for a total of 101 patients diagnosed with STEMI. In addition to routine evaluation, the Tei Index, E/e′, and mitral DT were recorded. These patients were reevaluated on the 30th day from admission to assess for MACE.
Out of the 101 patients, 55 experienced MACE (Group 1) while 46 did not (Group 2). Among the patients, 84 (83.16%) were male and 17 (16.84%) were female. The majority of patients (37% and 36.63%, respectively) fell into the age group of 51-60 years. In terms of presentation, 71 (70.30%) patients had anterior wall myocardial infarction (AWMI), 19 (18.8%) patients had inferior wall myocardial infarction (IWMI), and 11 (10.9%) patients had IWMI + RVMI.
The study found a significant association between adverse outcomes (MACE) and increasing age (P value = .002), BMI (P value = .000), presence of diabetes (P value = 0.04), Killip class at presentation (P value = .002), and ECG showing anterior wall infarct (P value = .006). Additionally, the research established a positive relationship between MACE and some echocardiographic parameters. LVEF, Tei Index, mitral inflow DT, and E/e′ ratio (P value = .000 for all parameters) were all strongly associated with MACE.
In Group 1, only 10 patients received PCI treatment, while 22 patients in Group 2 underwent this procedure. In contrast, 22 patients in Group 1 and 47 patients in Group 2 did not receive PCI treatment. Treatment with PCI also showed a strong association with favorable outcomes in MACE patients (P value = .002). There was no statistically significant correlation between the frequency of MACE and the gender of the patient (P = .143), smoking status (P = .122), or the occurrence of hypertension (P = .215). The study did not find any significant correlation between the occurrence of MACE and whether or not the patient received thrombolysis (by Streptokinase; P = .68) or the number of vessels involved (revealed during diagnostic CAG; P = .122).
To summarize, the data indicate that during the initial stage of acute MI, evaluating the Tei Index through echocardiography, along with other factors such as mitral inflow DT and E/e′ ratio. It helps identify patients at high risk of experiencing short-term cardiac events, which is usually considered for 30 days. Further research, however, is necessary to establish whether these parameters are of long-term prognostic significance.
Study Limitations
There were a few limitations to our observational study. The study had a limited population size and was conducted in a tertiary center where most of the patients were serious and had complications, which may have resulted in bias. Due to the limited availability of beds for female patients, the majority of participants were male, which may introduce a gender bias. Patients with failed PCI were not analyzed as a separate subgroup due to small numbers. This study did not compare the Tei Index with other established parameters, such as strain echocardiography or the Gensini score. Future studies may incorporate these parameters along with the Tei Index for a more comprehensive understanding.
Restrictive physiology reduces the IVRT due to the increased left atrial pressure. During the acute phase of MI, a short IVRT is not counterbalanced due to the satisfactory systolic function, resulting in a reduction of the index value (pseudonormalization of the Tei Index). Hence, the Tei Index may not be measured precisely. This can also occur in patients with atrial fibrillation, frequent supraventricular and ventricular extrasystoles, and atrioventricular and intraventricular conduction disturbances. The RV Tei Index was not separately assessed for patients with RV MI. Since our study had a follow-up period of up to 30 days, future studies may require a longer timeframe to obtain definitive conclusions. Additionally, we relied on clinical data to rule out infections or inflammatory diseases, but the chances of elevated serum uric acid levels in some patients could possibly be attributed to conditions that were not diagnosed. Moreover, using the E/e′ ratio in acute MI may not be very reliable as the e′ value depends on the region affected by the infarction, and different parts of the mitral annulus behave differently. This ratio cannot be applied in cases of severe mitral annular calcification, significant mitral/aortic regurgitation, or left bundle branch block.
Footnotes
Acknowledgment
The authors thank Monkwriter (
Authors’ Contributions
KS conceptualized and designed the study, conducted data analysis, and drafted the initial manuscript. SC contributed to data collection, patient enrollment, and echocardiographic assessments. DR assisted in statistical analysis, interpretation of results, and manuscript revision. SSS supervised the overall project, provided critical revisions, and approved the final version of the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients/caretakers have given their consent for their images and other clinical information to be reported in the journal. The patients/caretakers understand that their names and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Statement of Agreement
All authors of this study have reviewed and completely agree with the content presented in this manuscript. The requirements for the authorship have been met by all the authors, and that each of us believes that the manuscript represents honest work.