
Abstract
Cardiovascular diseases are a major health concern worldwide, and South Asians are known to have a higher risk of developing cardiovascular diseases compared to other ethnic groups. This risk is largely attributed to genetic predisposition, lifestyle factors, and comorbidities such as diabetes and dyslipidemia. The first international South Asian Cardiovascular Disease conference was organized, bringing together a diverse group of stakeholders, including public health researchers, patients, health practitioners, policymakers, and social scientists to discuss the current challenges and future directions in addressing the burden of cardiovascular diseases in this population.
Topics of discussion included the epidemiology and pathophysiology of cardiovascular diseases in South Asians, the role of genetics and epigenetics, lifestyle modifications, pharmacological interventions, and the use of technology in prevention and management. The need for a holistic approach that addresses the social determinants of health, promotes healthy lifestyles, and provides equitable access to healthcare was highlighted. Overall, the conference provided a platform for interdisciplinary collaboration and knowledge-sharing to address the significant burden of cardiovascular diseases in South Asians. It underscored the need for continued research and innovation to develop effective strategies that can reduce the incidence and impact of cardiovascular diseases in South Asians, and emphasized the critical need for effective prevention and management strategies that are culturally appropriate and tailored to this population.
Introduction
The South Asian (SA) community, consisting of individuals from the Indian subcontinent with origins in Bangladesh, Bhutan, India, the Maldives, Nepal, Pakistan, and Sri Lanka, is one of the fastest-growing racial and ethnic minorities in the United States, with almost 5.4 million people.1, 2 Despite their diversity, SAs encounter significant cultural, socio-economic, linguistic, and structural challenges that impede their access to good health, including an increased burden of cardiovascular disease (CVD) and mortality rates compared to other racial and ethnic populations. Even though the prevalence of conventional risk factors such as smoking, hypertension, and obesity may be the same or slightly less in SAs, the increased prevalence of diabetes, dyslipidemia, metabolic syndrome, abdominal obesity, and genetics may contribute to an alarmingly higher rate of more severe and aggressive CVD, with a younger age at the time of the first cardiac event, with significantly poorer surgical outcomes and survival rates as compared to other populations.3, 4 Amid the COVID-19 pandemic and a doubling in the prevalence of CVD cases over the past 30 years, the emphasis on preventing CVD has grown more critical than ever. 5
South Asians in the United States face a significant lack of resources for managing their elevated risk of CVD and its risk factors, leading to poor health outcomes and worsening racial and ethnic disparities.6, 7 This challenge is further exacerbated by a lack of detailed data on the unique risks, mechanisms, and effective interventions for CVD within this population. It is essential for healthcare providers, patients, and stakeholders to identify these risk factors, draw insights from global CVD-management programs, and recognize the importance of research participation to set future priorities for managing CVD in SAs in the United States.8, 9 To address these concerns, the first international South Asian Cardiovascular Disease (SACVD) conference was organized after 2 years of meticulous planning. This conference brought together a diverse group of stakeholders, including leading public health researchers, patients, healthcare practitioners, policymakers, and social scientists from around the world. With a multifaceted approach, the conference aimed to identify best practices and create synergies in research on health disparities affecting SAs, culminating in an action plan to address the high incidence of CVD in the SA community.
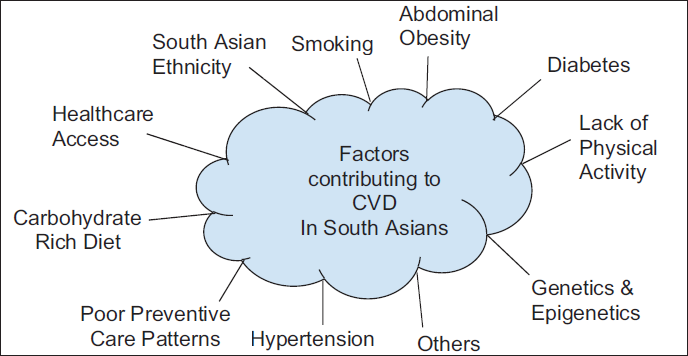
The 2-day conference covered various themes related to CVD risk factors, including genetic, epigenetic, and traditional risk factors, diabetes and metabolic syndrome, and health care access (Figure 1).
Factors Contributing to Cardiovascular Disease (CVD) in South Asians.
Through a collaborative environment that included patients and providers, ground-breaking scientific discoveries in CVD causes, and thought-provoking patient-provider dialogues on understanding hurdles to CVD management were discussed.
The conference aimed to understand and learn from successful global models to improve the identification of risk factors for CVD in SAs, and develop strategies for prevention, early diagnosis, and targeted treatment. The conference’s success highlighted the unique and robust partnership between patients, academia, healthcare, and non-profit SA community organizations. The need for an integrative approach was outlined and emphasized to overcome the challenges in the prevention and management of CVD in SAs (Figure 2).
Integrative Approach to Management and Prevention of Cardiovascular Disease (CVD) in South Asians.
The Burden of Cardiovascular Health Disparities in South Asians
The conference’s groundwork began with a keynote address by a distinguished public health expert, author, and researcher based in the United Kingdom, who had dedicated his career to investigating the causes of heart disease in SAs across both developed and developing nations. He addressed the “Epidemic of CVD in SAs: introduction to some mysteries and hypotheses, old and new,” discussing various hypotheses that have been proposed and/or studied so far to explain why SAs have a high susceptibility to heart disease. 10 Some of these hypotheses included the thrifty-genetic hypothesis, adipose-tissue distribution hypothesis, developmental hypothesis, and cooking hypothesis, which have been described in detail by him in his latest textbook entitled “Epidemic of Cardiovascular Disease and Diabetes: Explaining the Phenomenon in South Asians Worldwide.” The thrifty gene hypothesis has attributed food shortages as the reason for developing insulin resistance, with preferential usage of glucose by the brain, whereas the adipose tissue distribution hypothesis discusses environmental and epigenetic factors that have resulted in the distribution of fat to the abdominal and truncal regions in SAs. 10
The second keynote address, “An International Approach to the Prevention of Heart Disease,” discussed the international INTERHEART study, which revealed that several factors were significantly related to acute myocardial infarction, including smoking, ApoB/ApoA1 lipoprotein ratio, history of hypertension, diabetes, abdominal obesity, psychosocial factors, low daily consumption of fruits and vegetables, regular alcohol consumption, and lack of regular physical activity. 4 The study identified key steps such as avoiding tobacco, lowering low-density lipoprotein (LDL), and control of hypertension, which resulted in the reduction of CVD risk by 75%. The discussion highlighted the importance of primary intervention to reduce CVD risk and emphasized that underdetected and undertreated people at risk are prevalent, particularly in low-income countries with limited access to healthcare. Therefore, it was suggested that the use of community health workers for health education on prevention and to manage the progression of CVD in such settings was critical to reach these people at risk.
The Role of Genetics in South Asian Cardiovascular Disease
Genetics and/or family tendencies have been explained as the non-preventable cause of SACVD, often leading to a lack of modification of the risk factors by the patient. Research in human genetics and functional genomics of lipoprotein metabolism and atherosclerosis has focused on three objectives: first, to review the evidence for elevated triglycerides and low high-density lipoprotein (HDL) levels in SAs; second, to discuss the genetic factors that may contribute to dyslipidemia in this population; and third, to discuss the available data on the role of elevated Lp(a) in CVD in SAs. 11 Common patterns of dyslipidemia in SAs, which are characterized by increased triglycerides, elevated Apo B/ApoBa, increased LDL cholesterol, and lower HDL cholesterol, 12 have been associated with a genetic predisposition to these patterns, although the specific factors involved are currently unknown. Some research suggests that increased cholesterol transfer protein (CTP) levels in SAs may be linked to atherogenic dyslipidemias and that elevated Lp(a) levels may be leading factors in the development of CVD. While elevated HDL-C levels in SAs are thought to protect against coronary heart disease (CHD), more detailed research data are needed to develop personalized, precision medicine approaches to treat and prevent CVD in this population.
A presentation on the “Relationship of Genetics and Obesity to CVD in SAs” aimed to achieve three objectives: to recognize the differences in body composition between SAs and other race/ethnic groups, to understand the limitations of anthropometric measures in SAs for identifying high-risk individuals, and to describe the current knowledge of the genetic underpinnings of obesity and body composition. The discussion emphasized the need for a good polygenic risk score for SAs to determine their risk for CVD13, 14 was discussed as it relates to the various body types and the need for different body mass index (BMI) cutoffs to define overweight and obesity in SAs. Although SAs tend to have lower BMIs, their body fat content may be much higher, increasing their risk for insulin resistance, diabetes, and CVDs. South Asians also have a tendency towards a pear body shape with central abdominal obesity, which further increases their risk for these conditions.
Key Stakeholders and Organizational Perspectives on South Asian Cardiovascular Disease
Both keynote speakers emphasized that Identification of key stakeholders with alignment of interests helps to gain support for the goals to reduce CVD in SAs. Representatives from several notable institutes and organizations, such as the National Heart, Lung, and Blood Institute (NHLBI), American Diabetes Association (ADA), and American Heart Association (AHA), were invited to discuss the significance and consequences of SACVD health disparities for their organization. The Chief of the Epidemiology Branch at the NHLBI highlighted the lack of disaggregated data for highly heterogeneous Asian subgroups, which leads to poor understanding of the true health disparity of SACVD. 15 He outlined the National Institute of Health (NIH) strategic vision, which includes understanding human biology, developing resources and the workforce, reducing human disease, and advancing translational research. The NIH-NHLBI mission uses the approach of populomics to comprehensively understand disease, beyond classical epidemiology, with a research scope from molecular to population levels and cross-disciplinary collaborations.
The President of the ADA for Medicine and Science focused on the ADA perspective regarding the cardiovascular (CV) health of SAs. He reviewed the current national understanding of diabetes in SAs and its relation to CVD health and emphasized the earlier onset and more aggressive course of diabetes and CVD in SAs than in other populations. Poor control, with episodes of severe hypoglycemia, has been associated with a higher rate of CVD. He also reiterated that lifestyle management, such as decreasing obesity, controlling blood pressure, aiming for normal lipid profiles, and avoiding tobacco use, is crucial for preventing CVD in patients with diabetes. 16
The former President of the AHA discussed the AHA perspective on CVD health of SAs, aiming to highlight and synthesize recently published research and future national research goals concerning SAs’ CV conditions and disease. He acknowledged the increased rate of diabetes and insulin resistance in SAs, linked with a higher incidence of CVD, 17 and suggested that the World Health Organization guidelines for lower BMI cutoffs for obesity may be more suitable for SAs. 18 He also mentioned that the AHA 2024 Goals and Framework will aim to improve access to CV health for all, reduce health disparities, and combat structural racism, while promoting primordial prevention. 19
Successful Community-based Interventions
Prevention of CVD in SAs relies heavily on learning from the success of community-based awareness and their interventions. Community organizations possess grassroots connections that enable them to influence their community members to be proactive in managing their risk factors. Two such organizations shared their experiences with their respective communities. One described multiple testing sites that screen SAs for diabetes and prediabetes, and those at risk are directed to educational programs to prevent the onset or complications of the disease. The center also screens social determinants of health (SDOH) to connect underinsured or uninsured patients with charitable healthcare services. 20
The other organization described their community-based screening program for SAs, aimed at preventing CVD.21, 22 The Center’s AIM to Prevent and STOP-D programs provide culturally tailored, comprehensive screening, and lifestyle-focused interventions. The AIM to Prevent model includes assessing risk through a lifestyle and demographic questionnaire, lab tests for CVD and diabetes risk, blood pressure checks, and computed tomography (CT) scans for calcium scores. The intervention stage educates patients on medications, exercise, diet, and sleep, and the management stage supports patients through health coaches and trained community volunteers via telehealth. 23 This community-based care model has helped reduce CVD risk in patients across the United States.
Communication and Understanding of the Patient—Provider Perspectives on South Asian Cardiovascular Disease
Communication and understanding between the patient and the provider help the dyad to identify the unique risk factors and treatment needs for each patient to promote shared decision-making.
A patient experience panel was moderated and led by a prominent health researcher who focused on SA patients’ cultural beliefs, needs, and challenges in living with heart disease. The panel aimed to understand patients’ experiences of illness in their sociocultural context and receive their recommendations on improving heart health and optimal disease management. The panel, consisting of four SA patients and caregivers selected from regional medical practices and community groups, used a patient-centered questionnaire interview to explore coping skills, health values, social and cultural context, impact on life, and readiness for care. The questions were designed to elicit information about non-modifiable risk factors (e.g., ethnicity, genetics, age, sex) and modifiable risk factors (e.g., diet, exercise, interaction with the healthcare team, family and community resources, support), as well as the difficulty in managing the healthcare system and the impact of SDOH.
A provider panel led by a Chief of Endocrinology focused the discussion on the prevention and care of heart disease in SA patients. The panel, which consisted of a cardiologist leading a multi-site research and clinical institute, and a hospital administrator/leader with extensive experience using charity care as a solution to community health needs, an international researcher and internist, a coach navigator, and a community outreach director aimed to identify provider perspectives and key recommendations for improving heart health care in SA patients. The panel addressed themes such as best practices, necessary services to support SA heart health and improve health literacy, strategies for identifying and serving at-risk populations, challenges for SA-specific research collaborations, and the importance of health literacy and personal connection in delivering education to improve compliance.
Diagnostic Imaging in the Management of South Asian Cardiovascular Disease
New advances in technology, with the utilization of diagnostic imaging, have helped to identify CVD in the early stages. A professor of Cardiology and CV Research outlined the “heterogeneity of risk among Asians and SAs and the role of Imaging for CVD risk assessment in SAs.” He focused on the pathophysiology and epidemiology of atherosclerosis, specifically in SAs, and discussed the use of machine learning in analyzing large sets of data. The session aimed to achieve two objectives: first, to discuss available imaging techniques for evaluating CV risk in SAs, and second, to describe the heterogeneity of risk factors and related pathophysiology for atherosclerotic CVD in this population. 24
Highlighting the importance of using imaging studies to identify those at risk for CVD, specifically evaluating the characteristics of coronary artery magnetic resonance imaging (MRI) plaque to improve risk prediction of CVD events, 25 the professor emphasized the significance of understanding the length of time a person has lived with a risk factor, rather than just its prevalence, and how this heterogeneity could be attributed to factors such as culture, food, and religion. In addition, he emphasized the importance of primordial prevention in preventing the development of risk factors and suggested that subclinical atherosclerosis could potentially be controlled by managing hypertension, glucose levels, and BMI.
Comorbidities and Lifestyle Management for Prevention of South Asian Cardiovascular Disease
Diet and diabetes have been quoted as two main factors associated with SACVD. A leading, internationally renowned diabetologist participated in a virtual session, where he discussed the importance of large, community-based studies in SA populations to understand the relationship between diabetes and CVD. He highlighted the higher prevalence of diabetes and CVD in SAs, with diabetes occurring 15-20 years earlier than in Caucasians.26, 27 An Indian research study, the Chennai Urban Rural Epidemiology Study (CURES), showed that CVD prevalence was over 20% higher in patients with diabetes compared to those without, and that myocardial infarction occurred at a younger age and was associated with premature coronary artery disease (CAD) mortality in SAs.28–30 As an outcome of this study, an approach to diabetes management that involves controlling HgbA1C, blood pressure, LDL cholesterol, and maintaining discipline with diet, exercise, smoking, stress, and well-checkups was recommended.
Professor of Global Health from Toronto focused on the burden of hypertension in SAs and highlighted the suboptimal blood pressure control and minimal use of evidence-based preventive measures to treat CVD caused by hypertension. He stressed the need to reduce sodium in processed foods and promote access to fresh fruits and vegetables, reduce saturated and trans fats in the diet, minimize sugar-sweetened food and drinks, and create opportunities for physical activity. 31
The Need for Data to Develop Prevention and Treatment Strategies
During a presentation on “Use of Big Data and CVD Prevention in SAs,” it was emphasized that there is insufficient data available for the SA population. The researcher highlighted the differences in CVD data among various Asian subgroups and demonstrated how electronic medical records data can be used to understand these differences. 32 It was suggested that the UK Biobank, a large, population-based prospective study, which has been established to allow detailed investigations of the genetic and nongenetic determinants of the diseases of middle and old age, can be used as a model to collect large amounts of data for the SA population. 33 It was pointed out that although Asians comprise 60% of the world’s population, they are underrepresented in research trials by one in five, and the small numbers are grouped together, leading to inaccurate reporting of disease prevalence. 7 For example, while cancer was reported as the leading cause of death for Asians in a research analysis, disaggregating the data showed that CVD was the leading cause of death for SAs. Therefore, it is critical to disaggregate data to accurately understand the incidence of disease and how external or internal factors may impact the management of that disease in a specific population. Future research should allocate more funds to study Asians and their various subgroups to identify strategies for risk mitigation and address health disparities.
Lessons Learned and Recommendations for the Next Steps
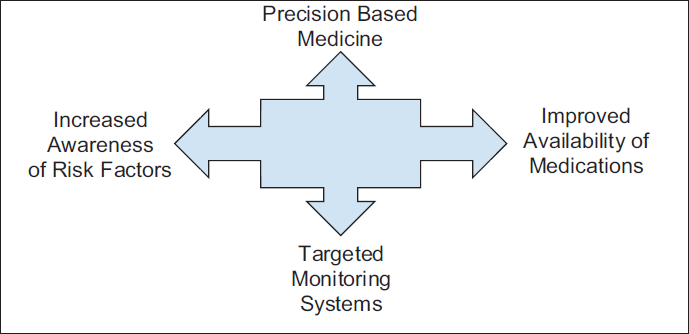
The various discussions and dialogues among the international experts and colleagues confirmed that SAs face a higher risk of developing CVD compared to other ethnic groups. This heightened risk is attributed to genetic predisposition, high rates of overweight and obesity, insufficient physical activity, and lower intake of fruits and vegetables, despite a predominantly vegetarian diet. Drawing from international best practices, it was concluded that a systems-based approach is essential to address these issues and to implement both primary and secondary prevention measures. This approach would involve restructuring the healthcare system to include awareness-raising of risk factors, targeted monitoring systems, improved availability of medications, and precision medicine-based treatments. Implementing comprehensive prevention and management strategies is crucial for reducing the burden of CVD and improving health outcomes for millions in the SA community (Figure 3).
Restructuring of the Healthcare System to Improve Cardiovascular Disease (CVD) Prevention and Management.
To generate a Call to Action for improving health outcomes and reducing health disparities in SAs, the following next steps and recommendations emerged from discussions and presentations at the first International SA CV Health Conference:
Increase awareness of health disparities and disease in the SA community and providers: a. Create and disseminate knowledge about proper navigation to appropriate health services and institutions, and the reduction of risk factors through lifestyle behavior changes to improve health and reduce the disease burden. b. Educate providers on cultural factors and other SDOH that may impact the care of SAs. Develop collaborative partnerships with other organizations, institutions, policymakers, and stakeholders for collective impact: a. Encourage policymakers to implement system-wide changes at healthcare facilities, insurance companies, and other institutions to reduce the economic burden by improving the health of SAs. b. Develop partnerships with other stakeholders to work collaboratively to increase and amplify the impact of the work being done, and to develop newer initiatives to focus on improving CVD health among SAs. Improve data collection and promote research on SAs: a. Encourage the disaggregation of data collection at national and state levels to better understand the true incidence and outcomes of disease in SAs. b. Develop research initiatives and requests for proposals (RFPs) that encourage institutions to participate in and initiate research focused on SAs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval and Patient Consent
Patient consent along with ethical approval from the Institutional Review Board was not applicable to this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.