
Abstract
Kounis syndrome is a rare phenomenon wherein cardiovascular symptoms develop after allergic or hypersensitivity reactions. We present the case of a 51-year-old male who developed anaphylactic shock after consuming kiwi fruit juice, followed by acute ST-elevation myocardial infarction (STEMI). Coronary angiography showed normal coronary arteries. This case emphasizes the importance of considering Kounis syndrome in patients with anaphylaxis and acute coronary symptoms.
Introduction
Acute ischemic cardiovascular events, including acute myocardial infarction, are one of the most common medical emergencies and require immediate attention. 1 Quick diagnosis and appropriate treatment can potentially save lives. Kounis syndrome is a rare but potentially serious condition triggered by an allergic reaction or a strong immune response, causing chest pain and other symptoms similar to myocardial infarction. Owing to its rarity, it is frequently misdiagnosed and treated inappropriately. We present the case of a 51-year-old gentleman who developed myocardial infarction after consuming fruit juice.
Case Presentation
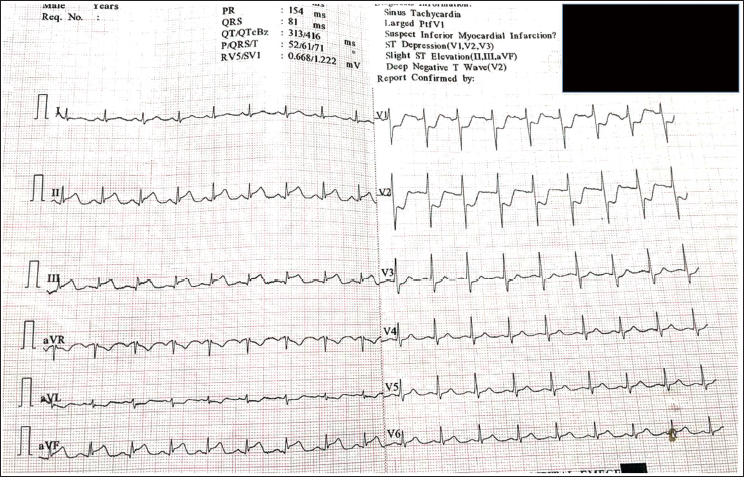
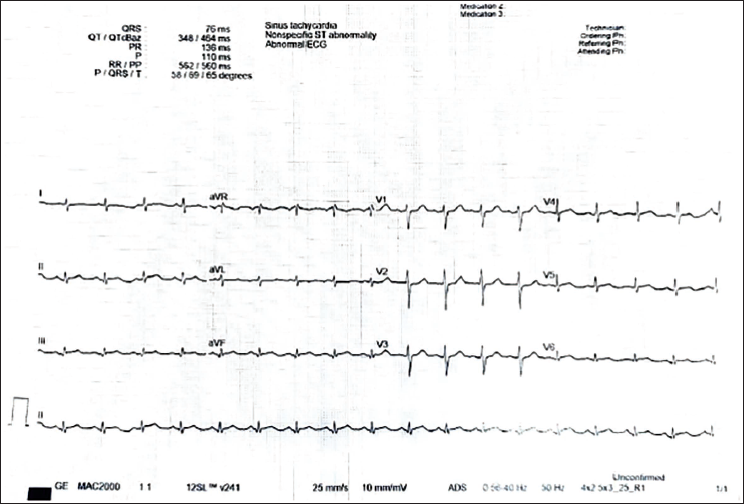
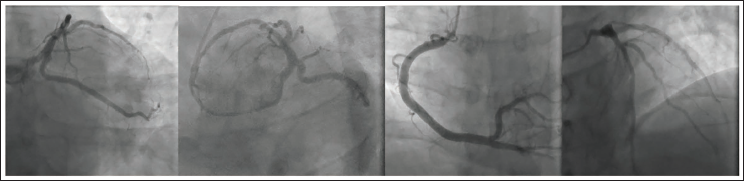
A 51-year-old male known to have systemic hypertension (on regular medications) developed giddiness, breathlessness, profuse sweating, and itching of tongue with lip and tongue swelling after having Kiwi fruit juice at a street side shop in Chennai. He presented to an outside hospital with cold clammy extremities and severe hypotension (SBP 60 mm Hg) and tachycardia at 130 beats/min. He was diagnosed to be having anaphylactic shock and was treated for the same with boluses of IV Normal Saline, Injection Adrenaline and Hydrocortisone, and anti-histamines, including Inj. Ranitidine. There was no improvement in the hemodynamics, but lip and tongue swelling reduced. Electrocardiogram (ECG) performed at the outside hospital showed gross ST-segment changes (ST elevation in leads II, III and avF, ST depression in leads V1-V3) suggestive of inferior and posterior ST-elevation myocardial infarction (STEMI) (Figure 1). Echocardiography showed inferoposterior hypokinesia of left ventricle (LV) with ejection fraction (LVEF) of 43%. The patient was given a loading dose of anti-platelets (Clopidogrel 300 mg, Aspirin 325 mg, Atorvastatin 80 mg) and was thrombolyzed with Inj. Streptokinase in the usual regime, prior to shifting to our hospital. On arrival at the emergency room, the patient was conscious, oriented, with a blood pressure of 90/60 mm Hg on vasopressor support (Noradrenaline) and oxygen saturation of 94% on 2 L of oxygen. Arterial blood gas analysis showed metabolic and lactic acidosis. ECG showed sinus tachycardia with settled ST-segment changes (Figure 2). Echocardiography showed normal sized LV with mildly hypokinetic basal inferior wall and LVEF of 60%, normal right atrium and right ventricle, normal filling pressures, trivial mitral regurgitation, and no mechanical complications like ventricular septal rupture. Baseline investigation revealed leukocytosis, increased serum creatinine level (2.4 mg/dL). The patient was continued on vasopressors, O2 support, anti-platelet agents, and statins managed conservatively. He improved clinically over the next 2 days with serum creatinine dropping to 1.7 mg/dL. Coronary angiogram was performed on day 3 using a minimum amount of Visipaque contrast. This showed right dominant system with normal epicardial coronary arteries without any evidence of spontaneous dissection, thrombus, luminal narrowing, and spasm (Figure 3). The patient remained clinically stable and was discharged from the hospital on day 4 with advice to continue oral nitrates and avoid repeat exposure to the allergen.
Electrocardiogram Done Then Showed Gross ST-Segment Changes, Suggestive of Inferior and Posterior ST-Elevation Myocardial Infarction (STEMI).
Electrocardiogram Post-Lysis Showing Sinus Tachycardia and Settled ST Segment Changes.
Coronary Angiogram Showing Normal Coronary Arteries with no Evidence of Residual Thrombus or Dissection Flaps.
Discussion
Kounis syndrome (KS) presents a fascinating and under-recognized entity within the realm of acute coronary syndromes (ACS). It is named after Kounis, who first described it in 1991 as chest pain occurring alongside allergic reactions, with clinical and laboratory findings mirroring classic angina pectoris. 2 The clinical presentation of KS mimics typical ACS, with patients experiencing chest pain, shortness of breath, and diaphoresis. 3 Diagnosing KS can be challenging due to the lack of specific biomarkers and the overlapping clinical picture with other forms of ACS. By carefully reviewing the patient’s medical history, a close temporal relationship with a potential allergic trigger can often be identified shortly preceding the onset of symptoms. Additionally, patients may report concomitant allergic manifestations, such as urticaria or angioedema, which are not seen in patients with non-allergic ACS. Electrocardiogram (ECG) findings may be unremarkable or show ischemic changes. Coronary angiography can be particularly valuable in diagnosing Kounis syndrome. When it reveals normal or near-normal coronary arteries despite ACS symptoms, it strongly suggests vasospasm as the underlying cause.
The precise pathogenesis of KS remains under investigation, but it is believed to be centered around mast cell activation and the subsequent release of inflammatory mediators.3, 4 These inflammatory mediators, such as histamine, chymase, tryptase, cathepsin D, leukotrienes, thromboxane and platelet activating factor, are thought to induce coronary artery vasospasm, leading to reduced blood flow to the heart and potential myocardial injury. 1 The triggers for mast cell activation can be diverse, encompassing medications (particularly antibiotics), insect stings, food allergies, and environmental exposures. 2 Abdelghany et al. 5 proposed a classification system for Kounis syndrome (KS), dividing it into three types (I-III). Type I occurs in patients with normal coronary arteries and no cardiovascular risk factors. In this type, an allergic reaction causes coronary artery spasm. Type II occurs in patients with pre-existing coronary artery disease wherein the allergic reaction leads to plaque erosion or rupture. Type III KS involves allergic reactions causing stent thrombosis in patients with pre-existing coronary stents. Our patient had Type 1 KS. The management of KS involves a two-pronged approach: addressing the acute coronary event and preventing future episodes. Standard ACS therapies, including antiplatelet medications, nitrates, and possibly even percutaneous coronary intervention, may be necessary depending on the severity of the presentation. These therapies may not be beneficial in patients having ACS due to pure coronary spasm (Type I KS) like in our case. Additionally, medications that target mast cell degranulation, such as histamine receptor antagonists, are beneficial in preventing recurrent episodes. 6
Thrombolysis is only effective for true STEMI ACS caused by a blocked epicardial coronary artery, especially due to plaque rupture or erosion or spontaneous dissection and thrombosis. Thrombolysis in Kounis syndrome could worsen the vasospasm and can lead to complications. Coronary angiography helps differentiate between non-allergic ACS and Kounis syndrome. In our patient, performing an angiogram before thrombolysis would have been ideal and thrombolysis could have been avoided. This case emphasizes the importance of a comprehensive workup, including a detailed history, comprehensive evaluation, and exploration of differential diagnoses, before initiating therapy in suspected ACS. This not only avoids unnecessary interventions but also allows for tailored treatment strategies.
Several reports of Kounis syndrome from Indian populations exist, some secondary to anaphylaxis, caused by the consumption of specific medications such as ceftriaxone, 7 diclofenac, 8 or nimesulide, 9 and some because of bee sting.10–12 Jariwala et al. 13 in 2022 reported the case of a 67-year-old gentleman with a history of coronary artery bypass surgery and percutaneous coronary intervention developing very late stent thrombosis because of an allergic response to mushrooms. Kiwi is a known allergen capable of causing severe allergic reactions in susceptible individuals. We report the first such instance following the consumption of this exotic fruit juice. Clinicians must recommend avoiding food, medications, and environment exposures that may trigger allergic reaction.
Conclusions
Clinical suspicion of KS should prompt immediate coronary angiography to delineate the type of pathology involved (dissection or plaque rupture with thrombus vs coronary spasm only). Thrombolytic strategies can be avoided in patients having KS with pure coronary spasm. Awareness of KS presenting with ACS helps in a tailored approach to secondary prevention strategies.
Footnotes
Author’s Contributions
Conceptualization, Y.V.C; methodology, J.S, A.W, A.M.K; data curation, A.W, A.M.K; writing—original draft preparation, A.M.K.; writing—review and editing, A.M.K, A.W, J.S.; supervision, Y.V.C. All authors have read and agreed to the published version of the manuscript.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study is a case report and ethical approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Individual patient consent was obtained for the use of patient related information and images for publication.
Statement of Human and Animal Rights
The study was conducted according to the guidelines of the Declaration of Helsinki.