
Abstract
Myocardial bridging of the coronary artery has been increasingly recognized as a cause of angina, myocardial ischemia, and sudden cardiac death owing to the advanced imaging systems being available. It has been most commonly found to occur in the left anterior descending artery as it runs down the interventricular groove between the right and left ventricle. Here we report two cases of isolated right coronary artery bridging with different clinical profiles and their importance in clinical practice. We also discuss the pathophysiology, complications, and management of myocardial bridging in regard to the two cases.
Introduction
Myocardial bridging of the coronary artery occurs due to the encasing of the coronary artery by myocardial fibers rather than the normal course between the epicardium and pericardium. Myocardial bridging was initially referred to as a tunneled artery as per the first description given by Henric Reyman. 1 Although most remain benign or presumed to be benign according to the initial understanding, recent evidence shows the varied manifestations of myocardial bridging from angina and acute coronary syndrome to sudden cardiac death.
The prevalence of myocardial bridging has been reported variedly. On conventional invasive coronary angiogram, the prevalence of bridging is around 5%, while it is around 19%-22% in coronary computed tomography (CT) angiography, and autopsy studies show a much higher prevalence of 33%-40%. 2 Myocardial bridging has been most commonly reported involving the left anterior descending artery as it runs in the ventricular groove between the left ventricle and right ventricular muscle mass. A cardiac CT coronary angiography-based study reported that 67%-98% of bridging occurs in mid-left anterior descending artery (LAD) segment. 3 Myocardial bridging of the right coronary artery (RCA) is a rarity with very few case reports in the literature search. Here we report two cases of RCA myocardial bridging with varied clinical presentations.
Case 1
A 50-year-old female with rheumatic heart disease presented with exertional dyspnea (New York Heart Association [NYHA II]) and fatigue for the past 7 months. On examination, there was loud S1 with a mid-diastolic murmur at the apex. Transthoracic two-dimensional (2D) echocardiography showed a rheumatic mitral valve with severe mitral stenosis and moderate mitral regurgitation. The mitral valve apparatus had anterior mitral leaflet calcification with sub-valvular disease and severe pulmonary artery hypertension (Right ventricular systolic pressure [RVSP]: 92 mmHg). Considering the valve apparatus was not amenable to percutaneous transvenous mitral commissurotomy, the patient was planned for mechanical mitral valve replacement.
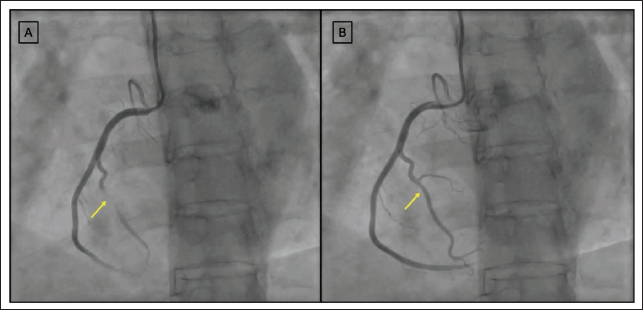
On presurgical coronary angiogram evaluation, the patient was found to have right dominant circulation with normal TIMI III flow in all the vessels. The RCA angiogram done in the left anterior oblique view showed a classical milking appearance in the acute marginal branch of the right ventricle (Figure 1A, B). On reviewing the echocardiogram, the patient was found to have severe right ventricular hypertrophy, possibly explaining the right acute marginal myocardial artery bridging. Considering the patient did not have any symptoms related to RCA marginal artery bridging and no evidence of ischemia, the patient was planned for surgical mitral valve replacement and medical management of myocardial bridging.
Case 2
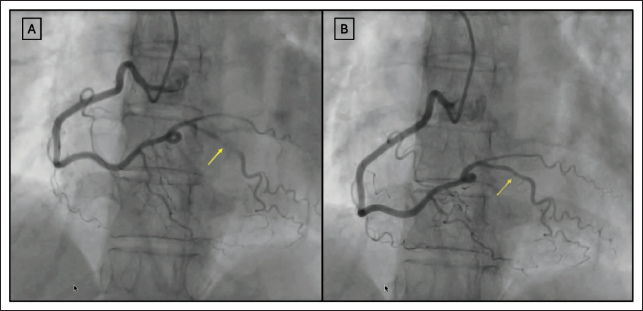
A 48-year-old female presented with exertional angina for 6 months. There was no history of breathlessness, palpitation, or syncope. The patient was on optimal medical therapy, including antianginals, for the past 4 months. A 12-lead electrogram and 2D transthoracic echocardiogram showed normal study. Because of persistent angina, the patient underwent functional testing with a treadmill, which was inconclusive. Hence, patient underwent a coronary angiogram, which showed right dominant circulation and no evidence of atherosclerotic disease with TIMI III flow. The posterior descending branch of the RCA was noted to have myocardial bridging just after its origin from the distal RCA. There was systolic narrowing and diastolic filling of the posterior descending artery (Figure 2A, B). The patient’s antianginals were up-titrated with beta blockers and calcium channel blockers, and nitrates were stopped. At the 3-month follow-up, the patient was symptomatically better with no exertional angina.
Discussion
Myocardial bridging occurs secondary to the intramural course of the epicardial coronary artery. Incidence of myocardial bridging has been found to occur in 5%-12% of patients undergoing angiography, but a higher incidence was seen in autopsy studies. 4
It is most commonly found in the left anterior descending artery. However, RCA myocardial bridges appear to be much less common, and to our knowledge, myocardial bridging of the RCA has been reported only in three cases previously.5–7
The RCA bridging in our patients had a different clinical profile. Case 1 had RCA bridging secondary to severe right ventricular hypertrophy due to pulmonary hypertension, while case 2 had no specific predisposing cause. Patient 2 was symptomatic with angina while patient 1 was asymptomatic for the bridging.
Management of myocardial bridging involves relieving the triggers and risk factor management if the patient is asymptomatic. 8 Hence, first patient was planned to address the primary etiology, which was severe mitral stenosis.
Management of symptomatic patients involves medical management along with percutaneous intervention or surgical intervention depending on the severity of symptoms. Medical management includes beta blockers and calcium channel blockers with avoidance of nitrates and other vasodilators. The second patient was managed on these lines with appropriate beta blockers and stoppage of nitrates, after which the patient improved symptomatically.
Learning Points
Myocardial bridging can have varied clinical manifestations, from being asymptomatic or having angina to sudden cardiac death.
Although rare, one needs to be aware of the possibility of myocardial bridging of the RCA to provide appropriate diagnosis and treatment.
Management of bridging depends on the symptom severity and underlying etiology.
Medical management includes beta blockers and calcium channel blockers and avoiding nitrates.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Appropriate well explained and written patient consent obtained from both the patients.