
Abstract
Renal artery involvement is commonly seen in Takayasu arteritis (TA) and patients often present with renovascular hypertension resistant to conventional antihypertensive therapy. Early initiation of immunosuppressive therapy with corticosteroids is the mainstay of treatment during active disease. Percutaneous transluminal renal angioplasty has emerged as a preferred mode of revascularization for renal artery stenosis during inactive disease primarily due to its safety, efficacy, and promising long-term outcomes. This report describes a young girl with TA with right atretic renal artery and severe stenosis of the ostial left renal artery who presented with uncontrolled hypertension and was successfully treated with percutaneous angioplasty. The utility of fractional flow reserve in TA-induced renal artery stenosis has also been emphasized.
Keywords
Introduction
Takayasu arteritis (TA) is a systemic vasculitis of the medium and large-sized vessels that frequently involves the renal arteries. 1 The common presentation includes renovascular hypertension and deterioration of renal functions, and percutaneous transluminal renal angioplasty (PTRA) in the absence of disease activity has been reported to have favorable long-term outcomes. 2 We hereby report a case of successful PTRA of the left renal artery in a young girl with TA and uncontrolled hypertension.
Case Report
A 19-year-old girl was brought to the cardiology clinic with complaints of recurrent episodes of occipital headache and significantly elevated blood pressure (BP) recordings for the last 6 months. She had been diagnosed with TA 1 year ago when she presented with complaints of pain in both lower limbs on exertion. Her initial evaluation had revealed high BP and significantly elevated inflammatory biomarkers (erythrocyte sedimentation rate (ESR): 42 mm h-1; C-reactive protein (CRP): 19 mg dl-1). A computed tomography (CT) aortogram revealed diffuse narrowing of the descending thoracic and abdominal aorta (Numano class III) with complete occlusion of the right renal artery at ostium with distal reformation of a diffusely atretic artery and 90% stenosis of the ostial-proximal left renal artery (Figure 1). Hence, she was diagnosed with TA based on the Sharma-modified Ishikawa criteria and had been started on oral prednisolone and methotrexate. Although her lower limb pain subsided, her antihypertensive requirements continued to escalate for the past year. At the current presentation to our center, her BP was uncontrolled even on maximum tolerable doses of five antihypertensive agents (cilnidipine 20 mg, furosemide 40 mg, prazosin 5 mg, clonidine 0.3 mg, and metoprolol 50 mg) orally per day. On physical examination, all peripheral pulses were palpable with BP recordings of 194/120 mm Hg in the right upper limb, 196/122 mm Hg in the left upper limb, 184/110 mm Hg in the right lower limb, and 186/114 mm Hg in the left lower limb. A bruit could be auscultated in the abdomen just above and to the left of the umbilicus, while the rest of her systemic examination was unremarkable. Her electrocardiogram and echocardiogram did not show any evidence of cardiac remodeling, and fundus examination showed no retinal changes.
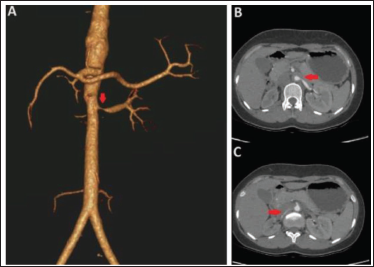
Currently, her inflammatory biomarkers (ESR: 28 mm h-1; CRP: 8 mg l-1) were within the normal ranges, indicating inactive disease. The right kidney was shrunken compared to the left with mildly altered cortico-medullary differentiation suggestive of early chronic kidney disease. Although the patient had normal renal parameters (creatinine: 0.9 mg dl-1), a Tc-99m diethylene-triamine-pentaacetate scan was performed which showed a cumulative glomerular filtration rate of 41 ml min-1 m-2 with a relative functioning of 56% and 44% of the left and right kidneys, respectively. In view of resistant hypertension, the patient was planned for a left renal artery revascularization.
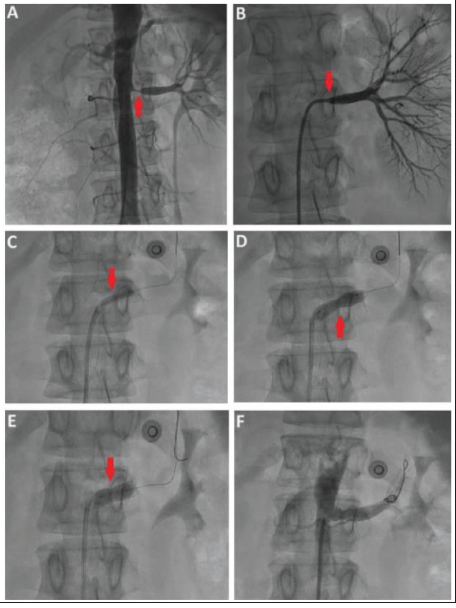
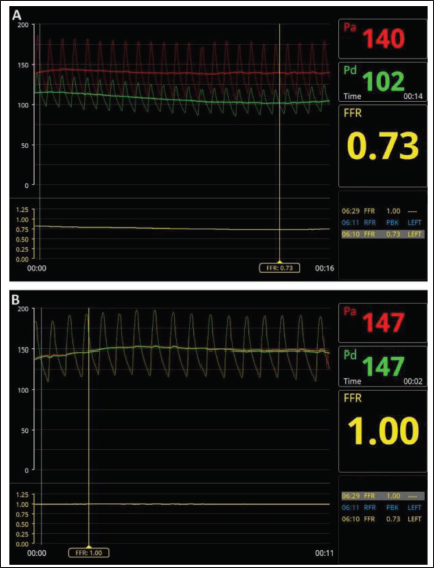
The patient was taken up for percutaneous catheterization using right transfemoral access. A non-selective angiogram using a 6Fr pigtail catheter (Figure 2A) confirmed the CT findings, and a selective angiogram of the left renal artery using a 6Fr Judkins right catheter (Terumo, NJ, USA) showed abrupt pressure dampening and absent contrast reflux suggestive of significant ostial narrowing (Figure 2B). The left renal artery was cannulated using a 6Fr renal double curve catheter (Boston Scientific, MA, USA), and a fractional flow reserve (FFR) study (Abbott Vascular, CA, USA) of the left renal artery (using nitroglycerine as hyperemic agent) was performed that showed a significant pressure drop across the stenotic segment (FFR: 0.73), implying significant stenosis (Figure 3A). PTRA of the left kidney was performed using a 4 × 15 mm non-compliant balloon (Terumo, NJ, USA; Figure 2C) followed by stenting of the diseased segment with a 7 × 18 mm RX Herculink Elite (Abbott Vascular, CA, USA) renal stent (Figure 2D). Post-dilatation of the stent was performed with a 6 × 12 mm non-compliant balloon (Abbott Vascular, CA, USA; Figure 2E) at 18 atm, and good luminal expansion was achieved (Figure 2F). A post-procedural FFR study showed a value of 1.0, indicating procedural success (Figure 3B).
Catheter-based Angiograms. (A) Non-selective Anteroposterior Aortic Angiogram Showing 90% Stenosis of the Ostial-proximal Left Renal Artery (Red Arrow). (B) Selective Angiogram of the Left Renal Artery with Absent Contrast Reflux (Red Arrow) Indicating Significant Ostial Narrowing. (C) Pre-dilatation of the Lesion with a 4 × 15 mm Non-compliant Balloon (Red Arrow). (D) Stenting of the Lesion with a 7 × 18 mm Renal Stent (Red Arrow). (E) Post-dilatation of the Stent with a 6 × 12 mm Non-compliant Balloon (Red Arrow). (F) Final Result After Percutaneous Intervention of the Left Renal Artery.
Fractional Flow Reserve (FFR). (A) Pre-procedural FFR Study of the Left Renal Artery. (B) Post-procedural FFR Study of the Left Renal Artery.
The patient had an uneventful post-procedural period and was discharged on dual antiplatelet therapy (aspirin 75 mg and clopidogrel 75 mg) and 20 mg oral cilnidipine on post-procedural day 1. By 1 week, all the home BP readings were within the normal range (<130/80 mm Hg), and she currently maintains well at 1-month follow-up with BP controlled on a single antihypertensive agent.
Discussion
Renal artery stenosis has been reported in 33%-80% of patients with TA and mostly presents with renovascular hypertension resistant to conventional antihypertensive drug therapy. 3 It is further associated with a significantly higher incidence of stroke, congestive heart failure, myocardial infarction, hypertensive encephalopathy, and renal failure and hence warrants prompt intervention. 2 Immunosuppression plays a key role during active inflammation and corticosteroid therapy has been reported to cause regression of renal artery stenosis (RAS) and reversal of renovascular hypertension. 4 Other drugs like methotrexate, cyclophosphamide, azathioprine, and tocilizumab are used in steroid-refractory cases or those with steroid-induced adverse effects. 1
PTRA has been consistently reported to have excellent results in inactive disease compared to surgical bypass due to its safety, efficacy, and less invasive nature. 5 Also, surgical repair has been associated with higher degrees of graft occlusion and aneurysm formation at the site of graft anastomoses. 6 Hence, PTRA has emerged as the default strategy in patients with TA-induced RAS (TARAS), and surgical therapy is sought only in cases with failed percutaneous repair or unfavorable vascular anatomy. The short- and long-term outcomes of PTRA in TARAS have been examined in multiple studies. Sharma et al. 2 studied 66 patients with TA who underwent PTRA and reported a 95% technical success rate and a 16% restenosis rate after 22 months of follow-up. Kinjo et al. 7 reported a technical success rate of 96.7% in 30 patients who underwent RAS treatment with a restenosis rate of 18.2%, 9%, and 62.5% in surgical, balloon angioplasty, and stenting groups, respectively. The higher restenosis rate with stenting compared to balloon angioplasty alone (odds ratio [OR] = 4.4) has also been emphasized in the meta-analysis by Jeong et al. 8 However, in many of these studies, stenting was performed in cases that had suboptimal results after balloon angioplasty, thereby causing a bias toward restenosis in the stented group. 5 Overall, ostial lesions, bilateral RAS, residual RAS >20% following PTRA, and suboptimal immunosuppression leading to persistent disease activity have been associated with a higher risk of restenosis in the future.3, 5
The utility of renal FFR has been advocated in moderately severe stenosis (50%-70%) of the renal arteries and might not have been indicated in our case with a 90% stenosis. 9 However, renal FFR has mostly been described in atherosclerotic RAS, and we wanted to establish its validity even in TARAS where the hyperemic effect of a vasodilator is retarded due to vessel wall fibrosis.9, 10 Also, such fibrosis may lead to incomplete luminal expansion in some cases despite high-pressure balloon inflations with an elevated risk of vessel wall dissections. In such cases, a demonstration of post-procedural equalization of pressures across the lesion using FFR may indicate procedural success, as was illustrated in our case. Another oddity in our case was the presence of an atretic right renal artery and a shrunken right kidney that initially made us question the therapeutic benefit of stenting the left renal artery for BP control. However, we obtained a significant reduction in BP on revascularizing the left renal artery while salvaging the ipsilateral kidney from ischemic injury. Nonetheless, regular follow-ups to monitor disease activity and adequate immunosuppression during disease flare will be essential to ensure a sustained benefit and prevent future restenosis.
Conclusions
Renal artery stenosis is a common cause of hypertension in young patients with TA, often resistant to conventional antihypertensive therapy. In the absence of disease activity, PTRA with/without stenting can provide excellent results without the toll of an open surgery. FFR can be utilized in determining the hemodynamic significance of borderline lesions and procedural outcomes. Period follow-up to monitor disease activity is key to preventing future restenosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was taken from the patient’s family before submitting this manuscript.