
Abstract
Chronic total occlusion (CTO) percutaneous coronary interventions have more complications due to intrinsic complexity of procedure which is further compounded by ambiguity of proximal cap. If the ambiguous proximal cap CTO is at ostial left anterior descending artery (LAD), impact of complications is huge as the area of myocardium at risk is significant. Hence, while treating ambiguous proximal cap CTO at ostial LAD or left circumflex artery (LCX), special attention must be given to prevent or minimize inflow injuries like dissection or intramural hematoma (IMH) of left main coronary artery (LMCA) and its branches. In order to prevent such complications, all the available CTO techniques need to be understood in this context and executed to keep procedural outcomes as predictable as possible. Intravascular ultrasound (IVUS) imaging is the passkey in wiring and detecting inflow injury to prevent intraprocedural catastrophes. This article explores the refinement and modification of existing techniques of CTO PCI and the use of imaging in the context of ostial LAD CTO PCI.
Introduction
Ostial left anterior descending artery (LAD) is part of the most significant bifurcation of coronary tree, and any intervention at ostial LAD or ostial left circumflex artery (LCX) has potential to endanger significant myocardial tissue leading to major hemodynamic deterioration or catastrophe. 1 A chronic total occlusion (CTO) in this zone can further increase procedure complexity and complications leading to undesired outcomes. Hence, wiring of ostial LAD (or) ostial LCX CTO needs special attention and careful recalibration of usual CTO wiring techniques to prevent inflow injuries for a predictable procedural outcome. 2 This review describes certain essentials of wiring of ambiguous cap ostial LAD CTO which can also be used for similar lesions in other bifurcations of coronary tree.
Essentials of Antegrade Wiring in Ostial LAD CTO
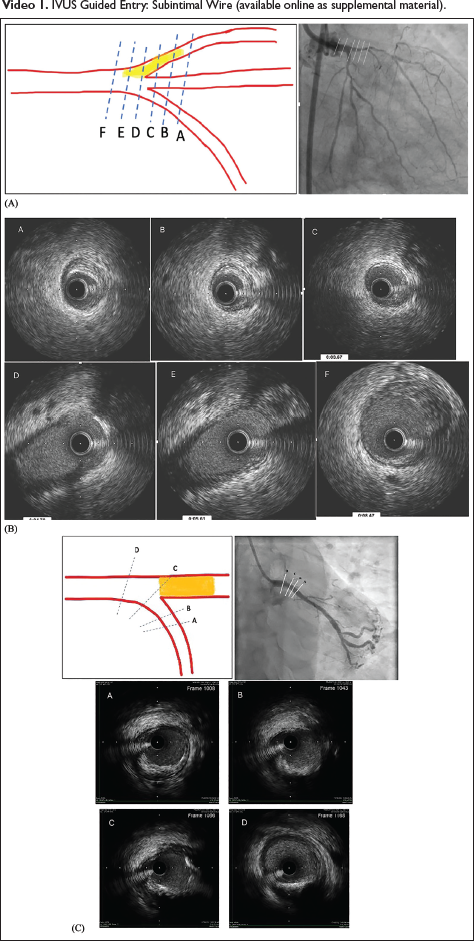
As already mentioned, prevention of inflow injury is pivotal while attempting antegrade wiring of ambiguous cap ostial LAD CTO. For this, complete Intravascular ultrasound (IVUS) guided antegrade cap puncture is essential. Imaging must be performed from the closest side branch, that is, ramus intermedius. If present, it is less angulated and provides good images for proximal cap identification and wire entry. Among ambiguous cap CTOs, even IVUS failed to clear the cap ambiguity in 30% of ostial LAD CTOs. 3 Absence of trifurcation and obtuse angle of LCX is unfavorable for IVUS-guided proximal cap puncture (Figure 1A-C). Complete IVUS-guided cap puncture includes identification of proximal cap with IVUS, Cap penetration under live IVUS followed by confirmation of appropriateness of cap puncture (Figures 2, 3, and Video 1).
(A) IVUS from RAMUS in Ostial LAD CTO. Favorable Angulation Gives Good Images (A to F) for Proximal Cap Identification. (B) IVUS Images of Proximal Cap in RAMUS Pullback. Gradual Appearance and Joining of Vessel in Image Transition from A to E (Correlation with Fluoroscopy Position Makes Cap Identification and Wiring Easy). (C) IVUS from Near 90 Degrees to Obtuse LCX in the Absence of RAMUS – Abrupt Transition at Confluence (from C ↓ D) May Not Uncover Ambiguity of Cap.
Appropriate Proximal Cap Entry. Wire, Proximal Cap, Wire Position Relative to Media of CTO Segment Clearly Visualized from B to E. Arrow Indicates Wire and the Orange Line Represents Media Location.

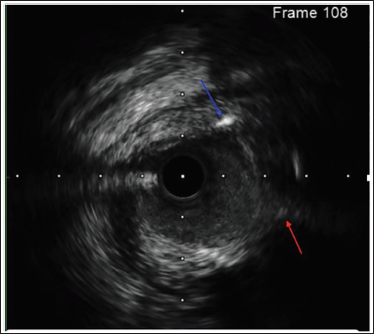
Red Arrow Indicates Proximal Cap and Blue Arrow Indicates Subintimal Wire Entry at Proximal Cap.
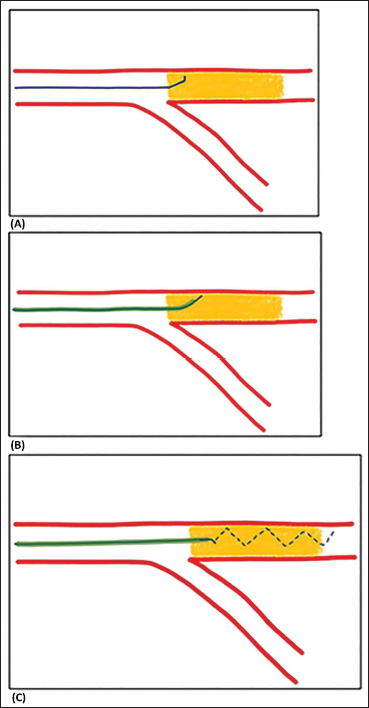
After a successful cap puncture, wire position is consolidated by advancing microcatheter into cap followed by further CTO segment crossing with de-escalated wire (Figure 4A-4C). If the wire reaches distal true lumen, confirmed by two orthogonal angiographic views, wire can be advanced further to move on to the subsequent steps. However, if the wire is subintimal after the distal cap, wire can be redirected in two orthogonal angiographic views (or) switched to parallel wire technique.
Wire De-escalation Technique After Cap Puncture. (A) Cap Puncture Wire Advanced up to Secondary Curve. (B) Microcatheter Advanced into CTO Beyond Proximal Cap. (C) Wire De-escalation to 1 mm Tip Wire.
Parallel Wire After IVUS Guided Cap Puncture
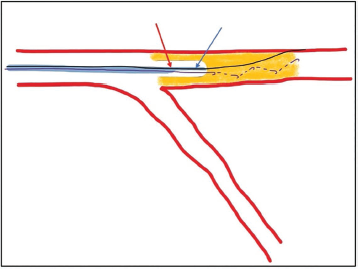
IVUS-guided cap puncture ensures appropriate entry into the CTO but does not guarantee the exit into the distal true lumen. Angulation within the lesion, long CTO segment, calcium within the lesion or hard distal cap can drive the antegrade wire into subintima. This leads to subintimal antegrade wire beyond the distal cap. Parallel wire (or) stingray re-entry if no bifurcation at distal cap can circumvent the situation. In parallel wire technique ensuring the second wire entry is through that of the first wire is crucial and can be done by advancing the double-lumen catheter into CTO segment till the OTW (over-the-wire) exit is beyond the ostium of LAD (Figure 5). In case of difficulty, space can be created by pre-dilatation with 1.25 (or) 1.5 balloons to facilitate the double-lumen catheter advancement. Parallel wire, a higher tip load wire than the first wire is introduced through the OTW lumen of double lumen catheter and advanced into distal true lumen using the first wire as a marker.4, 5 In the event of failure to reach distal true lumen, retrograde wiring with reverse CART for connecting spaces can be used.
Positioning of Double-lumen Catheter for Parallel Wire. OTW Exit (Red Arrow) Must Be Beyond Ostial LAD Before Parallel Wire Introduction.
Reverse CART in Ostial LAD CTO
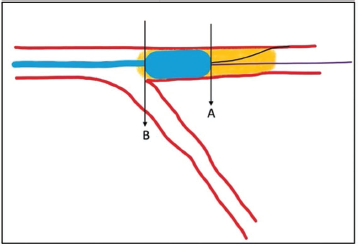
Failure to reach distal true lumen with antegrade wire, presence of good interventional collateral mandates retrograde wiring for successful recanalization of ostial LAD CTO. Reverse CART is the safest and most common strategy to bring the retrograde wire into the antegrade space. However, certain precautions are necessary to prevent inflow injuries (or) subintimal hematoma of left main coronary artery (LMCA). Directed reverse CART beyond the ostium of LAD with end balloon technique (retrograde wire directed to the distal end of an inflated balloon) and keeping the retrograde wire well away from the ostial LAD would minimize the inflow injuries (Figure 6). Guide extension assisted reverse CART with guide extension tip positioned well beyond ostial LAD would ensure retrograde wire course through the same entry of proximal cap confirmed by IVUS. Presumably, if guide extension is not used, it is safer to confirm retrograde wire course through ostial LAD with IVUS run from RAMUS (or) LCX before externalization and predilation.6–8
Reverse CART After IVUS-guided Ostial LAD Cap Puncture. Retrograde Wire Should Come to Antegrade Space or Guide Extension Around Point A.
Stenting Strategy
After successful wiring and predilation, IVUS from LAD & LCX is recommended to define inflow injuries before deciding on single or two stent strategies, and proximal landing zone.
IVUS in Ostial LAD CTO Intervention
In addition to antegrade proximal cap puncture and retrograde wire course through ostial LAD, IVUS is also useful to understand inflow lesions injuries before embarking on a stenting strategy. Presence of inflow lesions (or) intramural hematoma (IMH) in LMCA, which can be missed in angiography, mandates stent placement from LMCA to LAD, preferably, from ostial LMCA. IVUS interrogation of ostial LCX before and after stent placement. In provisional technique is key in guiding placement of the second stent.6, 9
Conclusion
Ostial LAD CTO PCI needs special attention during procedural planning to prevent or minimize inflow injuries and their catastrophic effects on outcomes. Apart from IVUS-guided antegrade cap puncture further refinement of existing techniques (Parallel wiring, Reverse CART) is needed to prevent inflow injuries of LMCA and its bifurcation. IVUS is an essential tool not only for antegrade preparation but also for detecting inflow injuries and defining a stenting strategy to prevent on-table catastrophes.
Footnotes
Abbreviations
CTO: Chronic total occlusion
LAD: Left anterior descending artery
LCX: Left circumflex artery
LMCA: Left main coronary artery
IMH: Intramural Hematoma
MLA: Minimum lumen area
OTW: Over-the-wire
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical permission was not applicable for this article, as this is a review article drafted from various research articles and not from patients directly.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Consent was not applicable, as this is a review article compiled from various research articles and guidelines and not from patients directly.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.