
Abstract
Background
Thyroid diseases are common in India. Both insufficient and excess thyroid hormones cause adverse cardiovascular events. Subclinical hypothyroidism and hyperthyroidism while undiagnosed can lead to derangement of cardiac functions. This study aimed to explore thyroid function abnormalities among heart failure patients of different severity (NYHA class).
Methodology
A descriptive, cross-sectional study was undertaken on 492 heart failure patients (246 males and 246 females) of age greater than 18 years. Patients were classified according to NYHA. Serum TSH and FT4 were investigated. Data were analyzed by standard statistical software.
Results
The mean age of participants was 54.2 ± 13.1 years. Mean FT4 and TSH were 1.36 ± 0.39 ng/dL and 2.89 ± 1.15 mIU/L, respectively. Patients belonged to NYHA class II (35.4%), III (52.4%) and IV (12.2%). Comorbidities included Hypertension (38%), Diabetes Mellitus (29%) and Dyslipidemia (52%). Hypothyroidism and hyperthyroidism were present in 27% and 5% patients respectively in overt or subclinical forms. The prevalence of thyroid disorders among NYHA class II, III and IV patients were 17%, 37%, and 50%, respectively.
Conclusion
Thyroid disorders were present in about one-third of the patients with heart failure. The prevalence of hypothyroidism was almost five times that of hyperthyroidism. The prevalence of thyroid disorders increased with the severity of heart failure.
Introduction
Heart failure (HF) is one of the prominent causes of morbidity and mortality worldwide. 1 The current American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) guidelines define HF as a complex clinical syndrome that results from structural or functional impairment of ventricular filling or ejection of blood, which in turn leads to the cardinal clinical symptoms of dyspnea and fatigue and signs of edema and rales. 2 More than 64 million people worldwide are affected with HF. 3 In India, the latest reported prevalence of HF was about 1% of the total population equaling about 8-10 million cases. 1 In India, there is a significant burden of thyroid diseases. Prevalence of around 21% was reported. 4 Thyroid hormones have a significant effect on cardiac structure and function. 5 Thyroid dysfunction is associated with adverse cardiovascular events leading to increased risk of premature morbidity and mortality. 6 There has been a lack of study findings on thyroid dysfunction among patients with HF in India. The main purpose of this study is to investigate the prevalence of thyroid dysfunctions among HF patients of different severity at a tertiary care hospital in Eastern India.
Methodology
Study Design
This was a descriptive, cross-sectional study conducted at the Department of Cardiology and Department of Biochemistry of a Tertiary Care Hospital of Kolkata, India between March 2021 and December 2022.
Study Population
The study was conducted on 492 clinically diagnosed patients of HF (246 males and 246 females) who attended Cardiology Outpatient Department (OPD) of this hospital during the period of data collection for the study. Patients of age more than 18 years were included in the study. Patients suffering from Chronic kidney disease, Chronic liver disease and Chronic lung disease and patients on medications affecting thyroid function were excluded.
Data Collection
The collected data included age, sex, type of HF based on ejection fraction (EF) and NYHA class. Data were collected through clinical records and a predesigned questionnaire. The types of HF are HF with reduced ejection fraction (HFrEF) where EF is below 40%, HF with midrange ejection fraction (HFmrEF) where EF is between 40% and 49% and HF with preserved ejection fraction (HFpEF) where EF is greater than 49%. 7 The NYHA class reflects the severity of HF and is based on clinical manifestations; NYHA class I is mildest and class IV is most severe.
Laboratory Investigations
Fasting venous blood samples were collected from the study participants and centrifuged to obtain serum. TSH, FT4, and TT3 were estimated by chemiluminescent immunoassay using ADVIA Centaur CP Immunoassay analyzer (Siemens) in the Department of Biochemistry. The reference intervals in our laboratory for serum TSH are 0.4-4.2 mIU/L, FT4 is 0.8-2.0 ng/dL and TT3 is 50.0-180.0 ng/dL. Different categories of thyroid function were defined as: Euthyroid (FT4 = 0.8-2.0 ng/dL, TT3 = 50-180 ng/dL & TSH = 0.4-4.2 mIU/L), overt hyperthyroidism (TSH < 0.4 mIU/L, FT4 > 2.0 ng/dL or/& TT3 >180 ng/dL), subclinical hyperthyroidism (TSH < 0.4 mIU/L, FT4 = 0.8-2.0 ng/dL & TT3 = 50-180 ng/dL), overt hypothyroidism (TSH > 4.2 mIU/L with FT4 < 0.8 ng/dL or TSH > 10 mIU/L), subclinical hypothyroidism (TSH = 4.2-10 mIU/L, FT4 = 0.8-2.0 ng/dL & TT3 = 50-180 ng/dL).
Statistical Analysis
The data were recorded in Microsoft Excel and were analyzed using Statistical Package for Social Sciences (SPSS) software version 20 (IBM, 2011). Descriptive data analysis was used.
Results
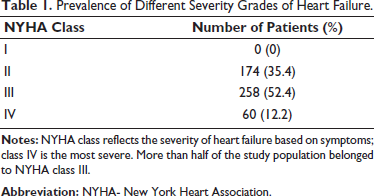
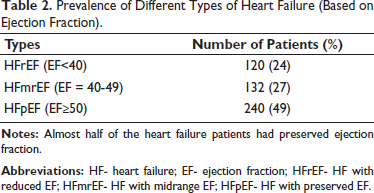
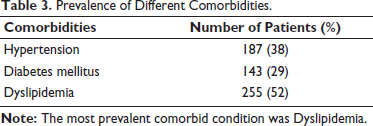
A total of 492 HF patients (246 males and 246 females) were recruited in the study. The mean age of the study population was 54.2 ± 13.1 years. The patients were classified according to both clinical and echocardiographic findings. Based on clinical presentation, 35.4% were NYHA class II (slight limitation of physical activity), 52.4% NYHA class III (marked limitation of physical activity) and 12.2% NYHA class IV (inability to carry on any physical activity without discomfort. No case had NYHA class I symptoms (Table 1). Based on EF, 24% had HF with reduced EF (<40) (HFrEF), 27% had HF with midrange EF (40-49) (HFmrEF) and 49% had HF with preserved EF (≥50) (HFpEF) (Table 2). Comorbidities included Hypertension (38%), Diabetes Mellitus (29%), and Dyslipidemia (52%) (Table 3), and 118 patients (24%) had Ischemic Heart Disease.
Prevalence of Different Severity Grades of Heart Failure.
Prevalence of Different Types of Heart Failure (Based on Ejection Fraction).
Prevalence of Different Comorbidities.
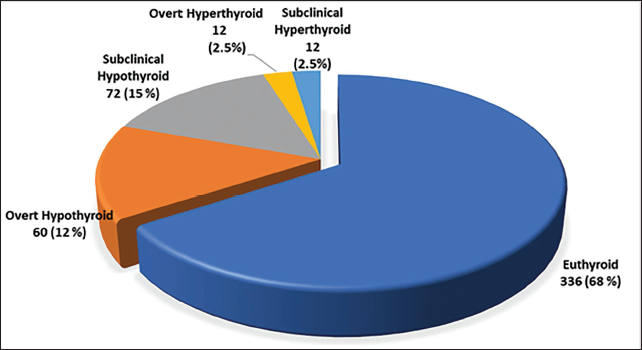
The mean FT4 level was 1.36 ± 0.39 ng/dL and the mean TSH level was 2.89 ± 1.15 mIU/L; 68% patients were euthyroid. Patients with thyroid dysfunction belonged to four categories −12% cases had overt hypothyroidism, 2.5% cases had overt hyperthyroidism, 15% cases had subclinical hypothyroidism and 2.5% cases had subclinical hyperthyroidism (Figure 1).
Prevalence of Different Thyroid Function Status Among the Heart Failure Patients.
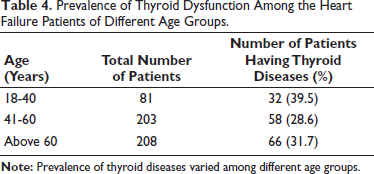
Considering the age of the patients, prevalence of thyroid dysfunction was highest (39.5%) in patients aged between 18 and 40 years followed by a prevalence of 31.7% in patients aged above 60 years. In patients aged between 41 and 60 years, prevalence of thyroid dysfunction was 28.6% (Table 4).
Prevalence of Thyroid Dysfunction Among the Heart Failure Patients of Different Age Groups.
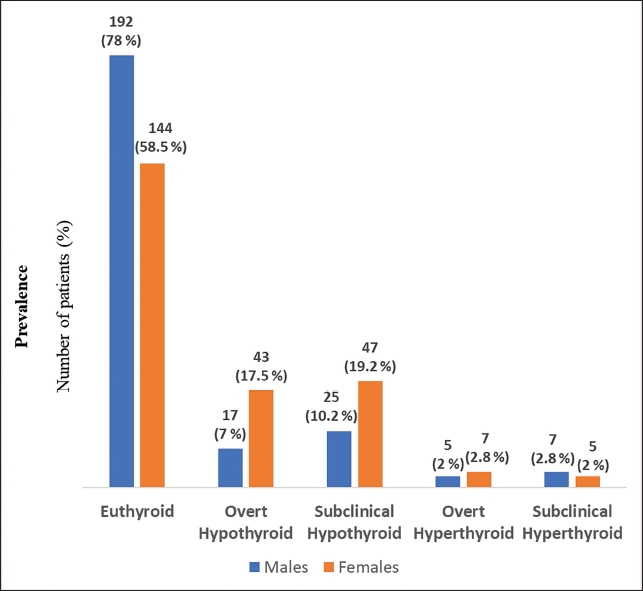
Of the total, 58.5% female patients and 78% male patients were euthyroid respectively; 17.5% females and 7% males were overt hypothyroid respectively, whereas 19.2% females and 10.2% males were subclinical hypothyroid respectively. Overt hyperthyroidism was present in 2% male and 2.8% female patients. Subclinical hyperthyroidism was present in 2.8% male and 2% female patients (Figure 2).
Prevalence of Different Thyroid Function Status Among the Heart Failure Patients of Both Sex.
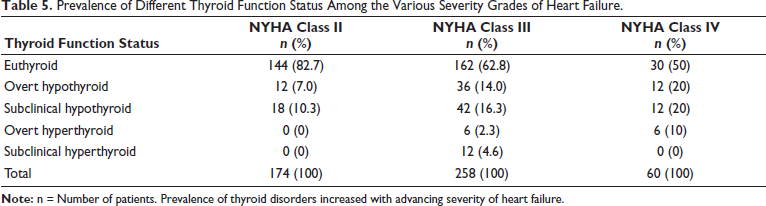
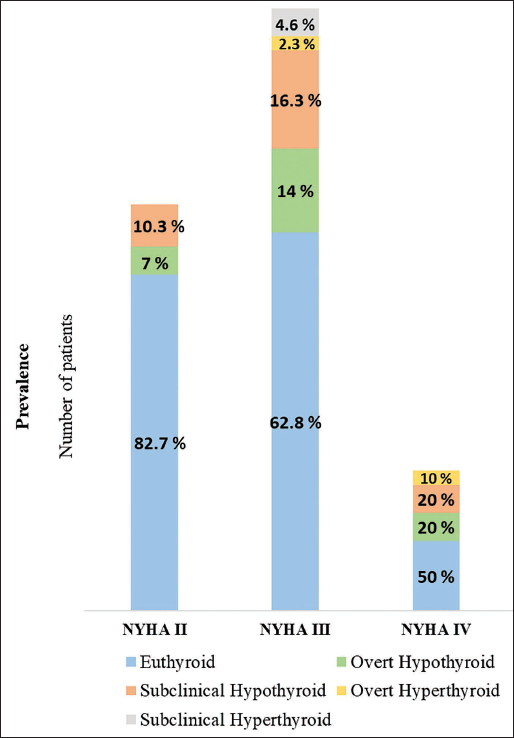
Prevalence of thyroid disorders showed an increase with advancing severity of HF. 30 patients (17.3%) among NYHA class II patients, 96 (37.2%) among NYHA class III patients, and 30 (50%) among NYHA class IV patients (Table 5 & Figure 3).
Prevalence of Different Thyroid Function Status Among the Various Severity Grades of Heart Failure.
Prevalence of Different Thyroid Function Status Among the Various Grades of Heart Failure.
Discussion
HF has high morbidity and mortality rates worldwide. 1 It is more common in the elderly. 8 Thyroid diseases are common in the Indian population. About 42 million people in India were reported to suffer from thyroid diseases in 2011. 9 Receptors of thyroid hormones are present in the myocardium. 10 Thyroid hormones affect cardiac function significantly, mediated by genomic and non-genomic actions. 9 Thyroid hormones cause regulation of genes for α-myosin heavy chain, β−myosin heavy chain, SERCA and phospholamban. 11 Non-genomic actions include the regulation of several ion channels like Ca2+ channels of cardiac myocytes.12, 13
Both insufficient thyroid hormones and excess thyroid hormones can cause HF- generally reversible with treatment of the underlying thyroid condition. Thyroid hormone deficiency causes decreased contractility, increased systemic vascular resistance, and bradycardia, while thyroid hormone excess causes increased contractility, increased blood volume from activation of the renin-angiotensin-aldosterone axis, and tachycardia.14, 15
The present study was undertaken with the objective of determining the burden of thyroid disorders among HF patients in a Tertiary Care Hospital in Kolkata. Findings indicate that 68% patients were euthyroid. Hypothyroidism was present in 27% patients (12% overt and 15% subclinical). Hyperthyroidism was present in 5% patients (2.5% overt and 2.5% subclinical). The prevalence of these thyroid disorders in the study population was higher compared to the reported prevalence in the general population of India according to a study by Unnikrishnan (10.95% overt hypothyroid, 0.67% overt hyperthyroid, 8.02% subclinical hypothyroid and 1.27% subclinical hyperthyroid). 4 A similar study was done by Kannan et al on HF patients in the USA in which majority of patients had NYHA class II (45%) or III (32%) symptoms. In that study, 74% of the HF patients were euthyroid, 5% had subclinical hypothyroidism, 5% had subclinical hyperthyroidism, 1% had overt hyperthyroidism and less than 1% had overt hypothyroidism. 14 Overall higher prevalence of thyroid disorders in the Indian population may have been reflected in our findings. 16
In our study, hypothyroidism was more prevalent among female HF patients (36.7%) compared to males (17.2%). There was an equal prevalence of hyperthyroidism in both sexes (4.8%). Both overt hypothyroid as well as subclinical hypothyroid cases were more common among females. Age of the patients is also an important factor. Prevalence of thyroid disorders was found to vary among patients of different age groups with the highest prevalence in patients aged between 18 and 40 years (39.5%).
Thyroid dysfunction may have a role in the progression of HF. Thyroid dysfunction triggers an inflammatory cascade. Proinflammatory cytokines (IL-6, IL-1β, and TNF-α) are cardio-depressants and lead to cardiac remodeling. C-reactive protein (CRP) is mainly produced in response to IL-6 and is involved in pathogenesis of HF with a direct relation to NYHA severity grade and cardiac performance. 17
In our study, the prevalence of thyroid disorders was found to increase with advancing severity of HF. Thyroid dysfunction was found in 17.3% NYHA II, 37.2% NYHA III and 50% NYHA IV patients. The prevalence of overt hypothyroidism among NYHA II, NYHA III and NYHA IV was 7%, 14%, and 20%, respectively whereas the prevalence of subclinical hypothyroidism among NYHA II, NYHA III and NYHA IV was 10.3%, 16.3%, and 20%, respectively. There were no previous studies done in the Indian population on the prevalence of different thyroid disorders in the different severity grades (NYHA class) of HF.
Our study has a few limitations. It was a cross-sectional study. Hence the risk posed by thyroid disorders toward the development of HF could not be ascertained. The study subjects were selected from the patients attending this hospital, so the results might not be generalized. The study design being descriptive the major aim was to find the prevalence of various thyroid dysfunctions where the significance of other comorbidities in the causation and progression of HF was not explored.
Conclusion
Thyroid disorders were present in about one-third of the patients with HF. Overall, the prevalence of hypothyroidism among the patients was almost 5 times compared to hyperthyroidism. Among NYHA class II HF patients, only hypothyroidism was found with subclinical cases being more common than overt cases. Both hypothyroid and hyperthyroid cases were found among NYHA class III and IV patients. Hypothyroidism was more common among patients of both classes. Among NYHA class III patients, subclinical thyroid dysfunction was more prevalent than overt cases. Among NYHA class IV patients, no subclinical hyperthyroid cases were found and prevalence of subclinical and overt hypothyroidism was the same. The prevalence of thyroid disorders increased with the advancing severity of HF. Hence thyroid function must be always evaluated in patients with suspected HF.
Since thyroid hormone imbalances have a profound effect on cardiac structure and function, early diagnosis and management of thyroid disorders may lead to reduction of morbidity and mortality due to HF. The outcome of the HF patients after correction of thyroid dysfunction needs to be evaluated.
Footnotes
Acknowledgements
We thank assistance of the lab technologists of Department of Biochemistry, IPGME&R and SSKM Hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee of IPGME&R and SSKM Hospital, Kolkata. The study was conducted in line with the Declarations of Helsinki.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Informed consent was obtained verbally from each patient before participation.