
Abstract
Coronary stent infection leading to Acute bacterial pericarditis is a rare but critical condition associated with significant mortality and morbidity, often complicated by the development of pericardial effusion and cardiac tamponade. 1 In this case report, we present the case of a 30-year-old male patient with a history of diabetes, who experienced an acute inferior wall myocardial infarction and subsequently underwent primary percutaneous coronary intervention (PCI) to the right coronary artery (RCA). Approximately two weeks after the PCI, the patient developed pericardial effusion with impending cardiac tamponade, requiring a pericardiocentesis procedure that resulted in the aspiration of 200 mL of fluid. Analysis of the pericardial fluid revealed the presence of pus cells, low glucose, and growth of Pseudomonas aeruginosa in culture. Further evaluation, including FDG PET imaging, demonstrated increased tracer uptake in the area corresponding to the RCA stent, while coronary angiography revealed the presence of an RCA aneurysm. The patient received appropriate antibiotic therapy followed by resection of aneurysm. This case underscores the importance of recognizing and promptly managing coronary stent infection-related complications to optimize patient outcomes.
Introduction
Mycotic coronary artery aneurysm represents a rare yet severe complication that can arise following percutaneous coronary intervention (PCI), carrying significant risks of mortality and morbidity. A comprehensive review conducted by Baker et al. 2 encompassing 97 published cases revealed a notable short-term mortality rate of 42.6% among affected individuals. Concurrently, the occurrence of infected pericardial effusion in association with mycotic coronary artery aneurysm is an exceptionally rare phenomenon, with only a limited number of documented case reports available. 3 Given the scarcity of reported instances, there exists a critical need for heightened awareness and understanding of these unique clinical presentations to facilitate prompt diagnosis and effective management.
Case Summary
We present the case of a 30-year-old man, known to have diabetes mellitus and systemic hypertension with past history of pulmonary tuberculosis, who initially sought medical attention at a local hospital due to angina lasting for a duration of two hours. Subsequent diagnosis revealed an acute inferior wall myocardial infarction (IWMI), leading to the administration of thrombolytic therapy using 1.5 lakh units of streptokinase. Transthoracic echocardiography demonstrated moderate left ventricular dysfunction. Two days following the initial presentation, a coronary angiogram revealed the presence of double-vessel disease. Percutaneous transluminal coronary angioplasty (PTCA) was successfully performed on the proximal and distal segments of the right coronary artery (RCA).
However, two weeks after the PCI, the patient experienced progressive shortness of breath accompanied by a nonproductive cough. Upon presentation to our hospital, a 2D echocardiogram revealed the presence of pericardial effusion with impending cardiac tamponade. Urgent pericardiocentesis was performed, resulting in the drainage of 200ml of straw-colored fluid.
A pigtail catheter was subsequently left in place for 48 hours. Ceftriaxone was initiated as empirical antibiotic therapy. Serial bedside echocardiograms demonstrated no recurrence of pericardial effusion over the following 48 hours, leading to the removal of the pigtail catheter. Analysis of the pericardial fluid revealed the presence of pus cells and low glucose. Bacterial culture grew multidrug resistant Pseudomonas aeruginosa, sensitive to ceftazidime avibactam with aztreonam combination and moderate sensitivity to colistin and polymyxin. Given the persistent cough and confirmed acute bacterial pericarditis and sterile blood cultures, a synpneumonic effusion was suspected, prompting a high-resolution computed tomography (HRCT) scan of the chest, which ruled out consolidation. To confirm stent related infection, a fluorodeoxyglucose positron emission tomography (FDG PET) scan was conducted, demonstrating uptake, suggestive of stent infection. A subsequent coronary angiogram confirmed the presence of a right coronary artery (RCA) aneurysm.
He was treated with ceftazidime-avibactam and aztreonam combination as it is a preferred treatment option over polymyxins for MDR gram negative infections. Polymyxins were also avoided in view of mild AKI (acute kidney injury) the patient had initially. After starting appropriate antibiotics, he improved symptomatically and clinically. Following two weeks of antibiotic treatment, the patient underwent coronary artery bypass grafting (CABG). During the surgical procedure, the RCA aneurysm was surgically opened, and the stent was removed via endarterectomy. The surgical team also performed left internal mammary artery (LIMA) grafting to the left anterior descending artery (LAD), and saphenous vein grafts (SVG) to the first diagonal branch (D1), obtuse marginal artery 1 (OM1), and distal RCA. The tissue culture sent intra-operatively did not grow any bacteria, most likely due to prior effective antibiotic treatment. Patient exhibited a satisfactory postoperative course and was discharged while continuing the antibiotics for 3 weeks after surgery and 5 weeks totally.
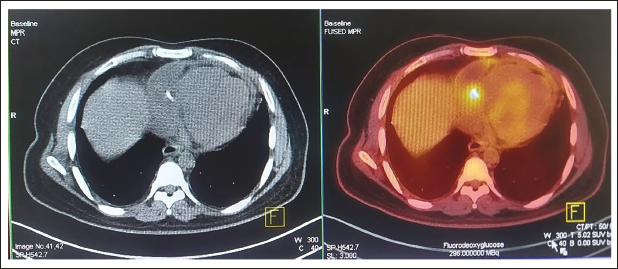
FDG PET showing hypermetabolic focus in the region of RCA stent.
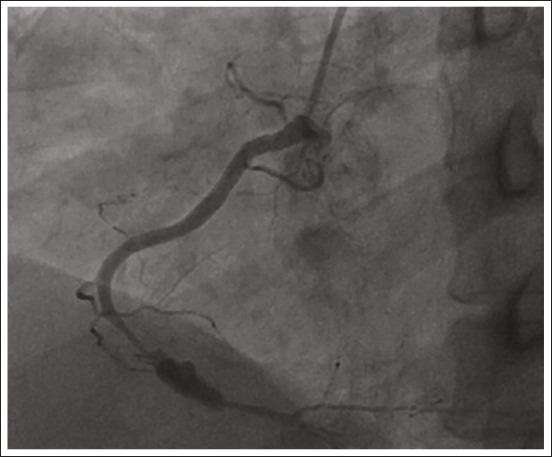
CAG showing distal RCA aneurysm.
Discussion
Infected coronary artery aneurysm (ICAA) is a relatively uncommon complication, often observed following percutaneous coronary intervention (PCI), with an incidence rate of less than 1%. Mortality rates associated with ICAA have been reported to be approximately 40%-60%. While spontaneous occurrence can be observed in immunocompromised individuals, it is more frequently reported in patients who have undergone PCI. Coagulase-negative staphylococcus is the most common pathogen implicated in ICAA, with an incidence of bacteremia less than 1%. 4 Streptococcus and Pseudomonas are the second and third most frequently identified pathogens causing mycotic aneurysms of the coronary artery. The right coronary artery (RCA) is the most commonly affected vessel, followed by the left anterior descending artery (LAD), left circumflex artery (LCX), and left main coronary artery (LMCA), which aligns with non-infected coronary artery aneurysms. 5 Drug-eluting stents pose a higher risk of infection compared to bare metal stents due to their immunomodulation properties. 6
The Two-Hit Hypothesis explains the pathogenesis of ICAA, involving an initial insult that leads to arterial wall damage and predisposes to aneurysm formation. The initial insult may be attributed to atherosclerosis, Kawasaki disease, systemic lupus erythematosus (SLE), and other connective tissue disorders. 7 The second hit occurs when infectious material directly spreads, hematogenously disseminates, or embolizes, promoting aneurysmal infection.
Several factors associated with PCI contribute to the development of mycotic aneurysms, including difficult vascular access, re-puncture, prolonged procedure duration, delayed sheath removal, laser angioplasty, oversized balloon and stents, and high-pressure balloon inflations. 8
Clinical features of ICAA include systemic symptoms such as fever, malaise, and nausea, often accompanied by chest pain and shortness of breath approximately 4-6 weeks after PCI, warranting suspicion of infected CAA in the absence of alternative diagnoses. Complications may include myocardial infarction, purulent pericardial effusion, aneurysm rupture, fistula formation into cardiac chambers, and sinus node dysfunction. 9
The diagnosis of ICAA was historically achieved postmortem until the late twentieth century. While coronary angiography is commonly utilized for diagnosis, CT imaging has emerged as a valuable diagnostic tool. Other diagnostic modalities employed include transesophageal echocardiography, PET-CT, and cardiac MRI. Positive blood cultures and evidence of purulent pericardial effusion on microbiology should raise a strong suspicion of ICAA in patients who recently underwent PCI. Coronary stent related infection was suspected as multidrug resistant pseudomonas was the causative pathogen, which commonly causes healthcare associated infections and device related infections. It also highlights the importance of detailed analysis of any sample/body fluid that is aspirated, as pericardial fluid in our case.
In low resource settings, delivering quality patient care in a cost-effective manner is important and reuse of cardiovascular catheters is common. However, high level disinfection with ethylene oxide sterilization is preferred over glutaraldehyde (cidex), although the latter is most commonly used in the majority of settings.
Currently, no established guidelines exist for the management of mycotic coronary artery aneurysms, and treatment approaches should be tailored to individual patients. For aneurysms smaller than 1cm in diameter, specific antibiotic therapy targeting the isolated organism is typically sufficient. 10 For aneurysms larger than 1cm, surgical intervention alongside medical therapy is recommended. Surgical resection of the aneurysm with endarterectomy, followed by revascularization via coronary artery bypass grafting (CABG), is the preferred surgical intervention. 11 Parenteral antibiotics for a minimum of 4 weeks are recommended. 12 In cases where patients are poor surgical candidates, the use of covered stents may be considered, although the potential risk of rupture exists. 13
In conclusion, infected coronary artery aneurysm (ICAA) following PCI is a relatively rare complication, with an incidence rate of less than 1%.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This is a case report and the patient was not subjected to any newer and unapproved pharmacological or interventional procedure, so ethical committee approval is not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.