
Abstract
Background
Spontaneous coronary artery dissection (SCAD) often impacts young women who lack traditional risk factors. Diagnosing SCAD can be challenging due to its diverse angiographic presentations and resemblance to other conditions, such as organized thrombus.
Case Summary
We present two cases involving middle-aged male smokers, each experiencing chest pain lasting over 12 hours. Both patients exhibited ST-segment elevation in the anterior leads on ECG, anterior wall hypokinesia, and an LVEF of 40% on 2D echocardiography. Immediate coronary angiography revealed dye staining and multiple radiolucent lumens in the LAD, indicative of SCAD. Optical coherence tomography (OCT) identified an organized thrombus with a distinctive “Swiss cheese” pattern, differing from the usual radiolucent false lumen associated with SCAD. Both patients were successfully treated with PCI, including thrombus aspiration and stent placement.
Take-home message
Relying solely on angiography for SCAD diagnosis may overlook organized thrombus. Redefining SCAD criteria and utilizing multimodal imaging like OCT in all cases is essential.
Keywords
Case Presentation
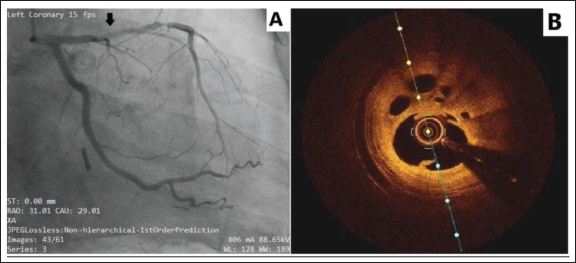
Two unrelated middle-aged male smokers each presented with chest pain lasting more than 12 hours. Upon examination, both patients were hemodynamically stable, with clear lung sounds and an unremarkable cardiovascular assessment. Laboratory tests showed elevated Troponin I levels in both cases. Electrocardiography revealed ST-segment elevation in the anterior leads, while 2D echocardiography showed anterior wall hypokinesia and a left ventricular ejection fraction of 40%. Urgent coronary angiography revealed a long segment of contrast dye staining along the arterial wall in the left anterior descending artery (LAD), with multiple radiolucent lumens and Thrombolysis in Myocardial Infarction (TIMI) flow grade 2 distal to it, suggestive of possible spontaneous coronary artery dissection (SCAD) (Figures 1A and 2A).
(A) Conventional Coronary Angiography Image Showing a Long Segment of Contrast Dye Staining of the Arterial Wall With Radiolucent, Smooth-Walled Intraluminal Filling Defects in the Proximal Left Anterior Descending Artery. (B) OCT Image of the Same Patient Showing a Swiss-cheese Appearance Due to the Presence of Multiple Intraluminal Channels Within the Thrombus.
(A) A Conventional Coronary Angiography Image Reveals a Long Segment of Contrast Dye Staining Along the Arterial Wall, With Multiple Radiolucent Lumens in the Proximal Left Anterior Descending Artery. (B) The OCT Image of the Same Patient Displays a “Honeycomb” Pattern Within the Lumen, With Multiple Interconnected Intraluminal Channels Separated by High-Signal-Intensity Septa, Indicative of a Recanalized Thrombus.
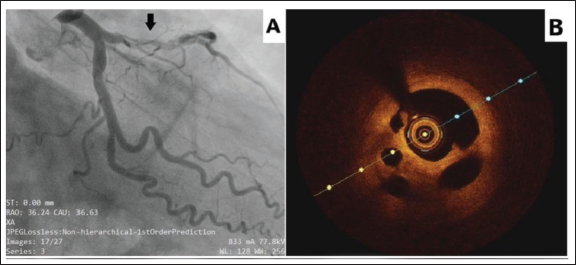
Even though the angiographic findings suggested a possible diagnosis of SCAD, the unusual occurrence of SCAD in middle-aged men with conventional risk factors prompted suspicion regarding the underlying etiology. To confirm the diagnosis, both patients underwent intravascular imaging using optical coherence tomography (OCT), which demonstrated multiple diaphragm-like membranes dividing the lumen into multiple small channels with a “lotus root” or “Swiss cheese” appearance (Figures 1B and 2B), consistent with organized thrombus rather than the typical radiolucent false lumen of SCAD.
Since both patients had evidence of ongoing ischemia and TIMI flow grade 2 in the LAD on angiography, they underwent successful percutaneous coronary intervention (PCI), including thrombus aspiration and stent placement, leading to symptom resolution and evidence of myocardial reperfusion. Both patients remained well on follow-up.
Discussion
Organized thrombus within the coronary artery can pose a significant diagnostic challenge, particularly because its clinical and angiographic features often resemble those of SCAD. Thrombus organization begins within one to two days of formation, involving the accumulation of fibrin, platelets, inflammatory cells, and collagen, and may continue for weeks to months, eventually forming a stable, fibrotic structure. 1 In the context of acute MI with STEMI, a fresh thrombus is typically expected. However, an organized thrombus may occur in association with non-culprit lesions causing chronic ischemia, silent ischemic events where thrombus organization begins before acute presentation, or recurrent thrombosis over a pre-existing plaque.
SCAD is classified into three types based on angiographic appearance. Type 1 shows the classic double lumen with an intimal flap. Type 2 manifests as diffuse long narrowing, with Type 2A returning to normal size distally and Type 2B extending to the distal tip without returning to normal. Type 3 mimics atherosclerosis with focal narrowing and often requires IVUS or OCT for confirmation. 2 These classifications are crucial for guiding appropriate patient management.
On angiography, SCAD and organized thrombus can share overlapping features, The presence of multiple channels within the thrombus can closely mimic the characteristics of a dissection associated with SCAD. This challenge is compounded by the low spatial resolution of angiography, which may not clearly distinguish between these entities, often leading to misdiagnosis or underdiagnosis, especially in cases of atypical presentations. SCAD involves a spontaneous dissection of the artery wall, creating a false lumen that compromises blood flow. In contrast, an organized thrombus manifests as a structured clot within the vessel, potentially causing obstruction but without the arterial wall dissection characteristic of SCAD. 3 Given the difficulty in distinguishing these conditions angiographically, advanced imaging techniques, such as OCT and intravascular ultrasound (IVUS), play a key role in guiding appropriate management.
OCT provides critical insights into differentiating SCAD from organized thrombus. In cases of SCAD, OCT typically reveals a double lumen or intramural hematoma, sometimes with an intimal tear, whereas an organized thrombus appears as a homogeneous or layered mass, often with a “lotus root” or “Swiss cheese” appearance due to microchannel formation. Unlike SCAD, these thrombi do not penetrate the arterial wall or form a false lumen. Additionally, thrombus-induced shadowing or signal attenuation can obscure deeper structures, another differentiating feature from SCAD. The precise imaging OCT offers is crucial for guiding therapeutic decisions.4, 5
The importance of accurate diagnosis in these conditions cannot be emphasized enough. Both SCAD and organized thrombus can manifest as acute coronary syndrome (ACS) and myocardial ischemia, but their treatment approaches are quite different. The management of SCAD typically aligns with the protocols for treating ACS, where antiplatelet agents and beta-blockers are frequently the first line of treatment. 6 However, employing strong antithrombotic therapies in SCAD presents a dual challenge: while it may reduce thrombus formation in the false lumen, improving blood flow in the true lumen, it can also heighten the risk of bleeding in the false lumen, potentially enlarging the intramural hematoma and reducing flow in the true lumen. 7
In general, a conservative management strategy is preferred for SCAD, unless there are signs of persistent ischemia, recurrent chest pain, hemodynamic instability, or left main dissection. 8 Conversely, organized thrombus typically calls for anticoagulant treatment to inhibit further thrombus growth, often combined with additional interventions like PCI or thrombectomy. 9
Several other conditions can mimic SCAD on imaging, complicating diagnosis. Atherosclerotic plaque rupture can resemble SCAD but typically occurs in older patients with risk factors and shows more diffuse calcifications on imaging. Coronary artery spasm causes transient narrowing that resolves with vasodilators and lacks an intimal tear. Coronary embolism leads to sudden occlusion, often from an embolic source such as atrial fibrillation, and may affect multiple coronary territories. Other mimics include iatrogenic dissection during catheterization or PCI, and vasculitis, which causes vessel wall thickening and narrowing alongside systemic inflammation. Recognizing these mimics ensures proper diagnosis and management of SCAD.
The prognosis of patients with SCAD and organized thrombus can vary depending on various factors, including the extent of coronary involvement, the presence of comorbidities, and the promptness of diagnosis and intervention. Long-term follow-up is essential to monitor for recurrent ischemic events, evaluate vessel healing, and assess the need for secondary prevention measures.
Conclusion
Clinicians should remain vigilant for close mimics of SCAD, such as organized thrombus, especially in atypical cases. A low threshold for advanced imaging, including OCT or IVUS, is critical to ensure accurate diagnosis and appropriate management, ultimately improving patient outcomes.
Consent
The authors confirm that written consent for the submission and publication of this case report, including images and associated text, was obtained from the patient per COPE guidelines.
Data Availability
The data underlying this article cannot be shared publicly to protect the privacy of the individuals involved. However, data will be made available upon reasonable request to the corresponding author.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study did not require ethical approval as it did not involve identifiable images or information.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.