
Abstract
Postinfective left ventricular pseudoaneurysm is extremely rare, and very few case reports are available in the literature. Ventricular pseudoaneurysm secondary to staphylococcal infection is usually managed through surgical intervention. We are presenting here a rare case of post-varicella disseminated Staphylococcus aureus infection with ventricular pseudoaneurysm and constrictive pericarditis, which was managed successfully through surgical intervention.
Introduction
Postinfective ventricular pseudoaneurysms are extremely rare and require immediate surgical intervention; otherwise, they may be fatal. We present a case of left ventricular pseudoaneurysm with constrictive pericarditis secondary to Staphylococcus aureus infection in a child managed successfully through surgical intervention.
Case Presentation
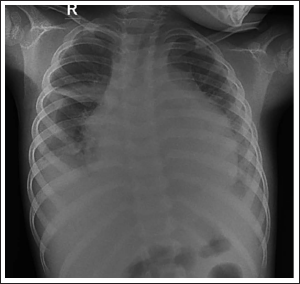
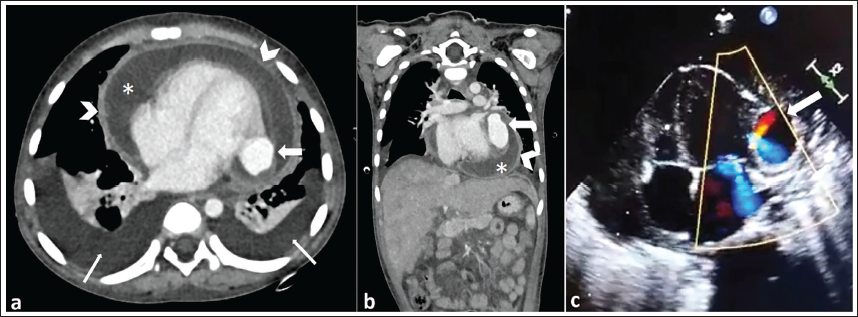
A five-year-old boy presented to our institution in 2023 with a history of high-grade fever, anasarca, and respiratory distress for the last one month. These symptoms were followed by varicella infection. His vital parameters were as follows: pulse rate—110/min, respiratory rate—52/min, and blood pressure—106/66 mm Hg in the right upper limb. Complete blood counts revealed neutrophilic leukocytosis with elevated C-reactive protein and erythrocyte sedimentation rate (ESR). Chest X-ray revealed pericardial and bilateral pleural effusion (Figure 1). On clinical examination, hepatomegaly was noted. Contrast-enhanced computed tomography (CECT) revealed bilateral pleural effusion, moderate pericardial effusion with the thickened pericardium, and features of congestive hepatopathy (Figure 2a and b). There were passive atelectatic changes in the underlying lower lobes of the bilateral lungs. A contrast-filled outpouching of 1.8 × 2.0 × 3.2 cm was seen from the left ventricle in the submitral location, suggesting a pseudoaneurysm. The pseudoaneurysm was seen communicating with the left ventricle through a narrow neck. Echocardiography corroborated the CECT findings and revealed that a ventricular pseudoaneurysm arising from the left ventricle with a narrow neck and sac showed to and fro flow on color Doppler (Figure 2c). Apart from a pseudoaneurysm, he had a thickened pericardium with features suggestive of constrictive pericarditis. With the clinical picture and investigations, varicella complicated by secondary bacterial infection was considered, and empirical antibiotic therapy with ceftriaxone, teicoplanin, and clindamycin was initiated. Blood culture grew methicillin-sensitive Staphylococcus aureus, and antibiotics were changed to intravenous linezolid as intravenous cloxacillin was unavailable. He was given symptomatic treatment with oxygen, diuretics, and albumin infusion. However, anasarca persisted, and respiratory distress worsened, requiring the initiation of noninvasive respiratory support. Hence, the treating team considered cardiac surgical intervention, that is, subtotal pericardiectomy ± ventricular aneurysm repair. Intraoperative transesophageal echocardiography revealed autoseal of pseudoaneurysm with no color flow communication with the left ventricular cavity. As the pseudoaneurysm was autosealed and located in the atrioventricular groove, a danger zone to operate, the treating team decided to continue conservative management for the pseudoaneurysm, and only subtotal pericardiectomy was performed. The child was extubated on postoperative day 1 (POD 1). On POD 2, the child developed fullness over the right side of the neck and right upper limb edema. Doppler ultrasound showed thrombosis in the right internal jugular vein (IJV). There was no trauma or attempt to cannulate the right IJV. This can be attributed to spontaneous thrombosis secondary to the sepsis with a probable underlying hypercoagulable state. Inj. Enoxaparin was started, and the swelling over the right side of the neck and right upper limb subsided over the next 10 days. Repeat Doppler ultrasound showed persistent thrombus in the right IJV; hence, it was planned to continue enoxaparin. He had bilateral intercostal drains and pericardial drains in situ. He had high drain output, that is, 40–60 mL/kg/day during the first seven days, which was gradually reduced. Pericardial and left intercostal drains were removed on POD 15, and the right–left intercostal drain was removed on POD 27. There was no evidence of chylous fluid in the drain. Echocardiography on POD 37 revealed minimal pericardial effusion anteriorly, mild mitral and tricuspid regurgitation with normal biventricular function. Intravenous linezolid was changed to the oral route and continued for a total duration of eight weeks. He was discharged on POD 40 in stable clinical condition. At 12 weeks of discharge, the child was active, hemodynamically stable, and started attending school. Written informed consent was obtained from the patient’s parents.
Chest X-ray Showing Globular Enlargement of the Cardiac Shadow with Enlarged Cardiothoracic Ratio and Bilateral Pleural Effusion.
CECT Axial (a) and Coronal (b) Images Showing the Pseudoaneurysm (Thick White Arrows) Communicating with the Left Ventricle Through a Small Neck. There Are Features of Constrictive Pericarditis in the Form of Bilateral Pleural Effusion (Thin White Arrows), Pericardial Effusion (Asterisk), Thickened Pericardium (White Arrowheads), and Congestive Hepatomegaly. (c) Echocardiography with Color Doppler Showing the Pseudoaneurysm (White Arrow) Arising from the Left Ventricle.
Discussion
The current case report represents a rare case of post-varicella secondary disseminated Staphylococcus aureus infection with ventricular pseudoaneurysm and constrictive pericarditis in a child. A pseudoaneurysm of the vessel or the cardiac chambers occurs when there is a defect in the wall of the arterial or cardiac chamber, and the leaking blood collects in the surrounding tissue. The leaked blood is contained by the adventitia or surrounding soft tissue. There is a handful of cases described in the literature related to postinfective ventricular pseudoaneurysm with pericarditis. We performed a thorough literature search in the Medline database, and only a few cases of postinfective ventricular pseudoaneurysm with pericarditis have been reported in the English literature. Moraes et al published the first case of postinfective ventricular pseudoaneurysm in a child, which was managed successfully through resection of the pericardium, drainage of infective pericardial effusion followed by the closure of the wall defect with autologous pericardium. 1 Boer et al., Gaur et al., Desai et al., and Juneja et al. have described similar cases of postinfective ventricular pseudoaneurysm, which were successfully managed by the closure of the left ventricular defect with a patch.2–5 Vinitha et al. have described a similar case that was successfully managed through the closure of the pseudoaneurysm neck with pledgeted sutures. 6
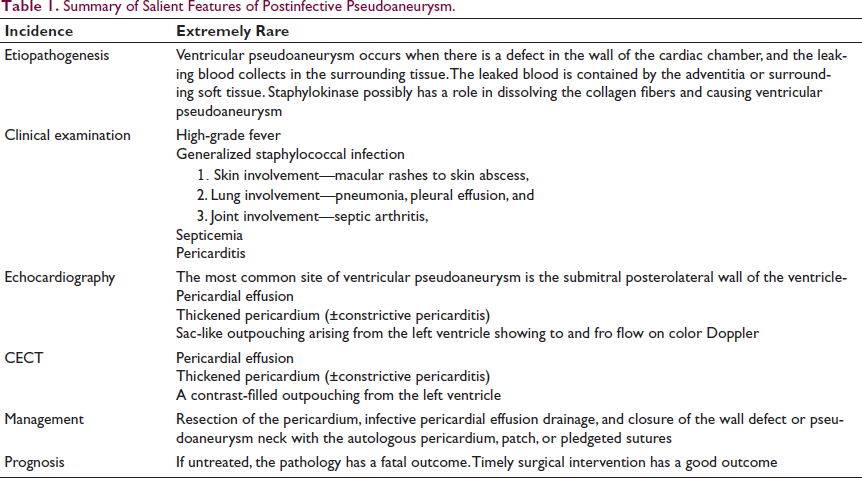
All of them were associated with staphylococcal infection and had a history of skin and joint involvement. The time gap between the onset of fever and the diagnosis of the left ventricular pseudoaneurysm was in the range of two to four weeks. Pericarditis was seen in all of these cases. The salient features of postinfective pseudoaneurysm are summarized in Table 1. The exact cause of ventricular pseudoaneurysm secondary to staphylococcal infection is unknown, but it is believed that staphylokinase has a role. 4 It converts the inactive plasminogen to plasmin, disintegrating collagen fibers. The most common site of ventricular pseudoaneurysm is the submitral posterolateral wall of the ventricle due to congenital weakness of this region. Usually, it takes only a few weeks to develop a postinfective pseudoaneurysm after the onset of septicemia and pericarditis secondary to staphylococcal infection.
Summary of Salient Features of Postinfective Pseudoaneurysm.
Conclusion
Postinfective left ventricular pseudoaneurysm is extremely rare. It can be comfortably diagnosed by CECT or simply by echocardiography. A surgical intervention consisting of closure of the pseudoaneurysm neck with sutures or a patch is the most effective way to achieve a positive outcome.
Footnotes
Authors’ Contribution
Biswajit Sahoo and Krishna Mohan Gulla contributed to conceptualization and writing-original draft.
Satyapriya Mohanty, Manoj Kumar Nayak, and Arunprakash Pitchaimuthu helped in writing-review and editing.
Declaration of Conflicting Interests
The authors declare that they have no financial or nonfinancial conflicts relevant to the article.
Ethical Approval
The case report does not require ethics approval in our institution. The ethics committee of our institution waived ethical approval, and all the procedures being performed were part of the routine care.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient’s guardian in line with COPE guidance.