
Abstract

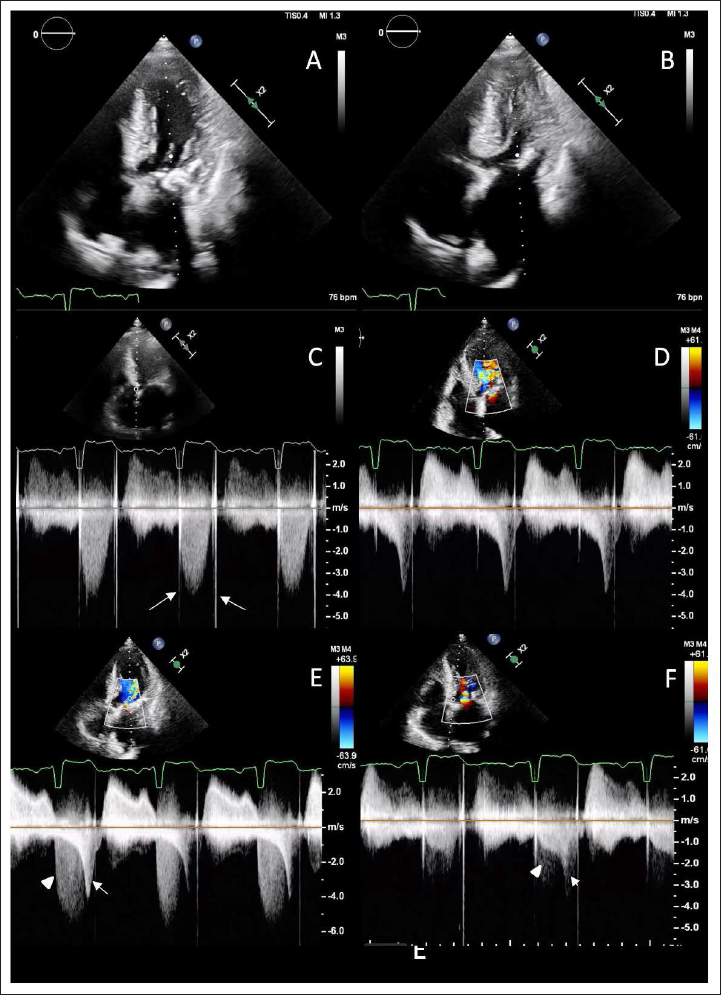
A 62-year-old hypertensive man with severe aortic stenosis (AS) secondary to rheumatic heart disease (RHD), who underwent aortic valve replacement (AVR) 38 years prior, presented with dyspnea on exertion. Echocardiography showed severe left ventricular hypertrophy (Figure 1A and B) and a severely elevated aortic valve gradient (mean 49 mmHg) (Figure 1C). A continuous wave Doppler interrogation of the left ventricular outflow tract (LVOT) revealed an additional dagger-shaped gradient across the LVOT, indicating a dynamic LVOT obstruction (Figure 1D–F). Echocardiographic interrogation revealed the presence of another symmetric and dense jet of mitral regurgitation. This finding, coupled with the observation of LVOT and aortic obstruction, presented a significant diagnostic challenge (Figure 1E). The patient’s medical history revealed a chronically elevated prosthetic valve gradient due to pannus, with documented evidence of progressive increase over time. Currently, he is awaiting AVR with septal myectomy.
Apical 5-chamber view showing significant left ventricular hypertrophy with a sigmoid-shaped septum in diastole (A) and near-total obliteration (B) of the left ventricular cavity during systole. Continuous wave Doppler interrogation across the aortic valve showing a symmetrical high-velocity (C) Doppler tracing indicating prosthetic valve dysfunction (note the opening and closing artifacts of metallic prosthetic valve: arrows). Another dagger-shaped Doppler (D) tracing was also seen with a maximum velocity of 4 meters/second indicating severe LVOT obstruction. Mitral valve inflow Doppler showing a combined jet (E) of dense mitral regurgitation (arrowhead) and dynamic LVOT obstruction (arrow); note the absence of prosthetic valve artifact on the tracing and there is a striking difference of shape and velocity between mitral regurgitation (E) and aortic Doppler tracing (C). Continuous wave Doppler across LVOT showing concomitant (F) fixed obstruction of prosthetic valve dysfunction (arrowhead) and dynamic LVOT obstruction (arrow) but in different planes. LVOT – left ventricular outflow tract.
LVOT obstruction has been documented in patients with severe AS due to the associated left ventricular hypertrophy. However, the increased afterload in severe AS causes a splinting effect on LVOT walls, masking this obstruction. When the fixed obstruction gets corrected by AVR, causing a reduction in LV end-systolic pressures, the dynamic obstruction gets unmasked.
Such abnormal intraventricular flow velocities are seen in 14% of patients after AVR (more commonly at the mid-cavitary level than LVOT); however, it remains an under-recognized entity. 1 The predisposing factors are AS being the underlying etiology, concentric hypertrophy, sigmoid septum, elongated and redundant mitral valve apparatus or calcified mitral annulus causing systolic anterior motion (SAM), hypovolemia and vasodilation, use of inotropes or IABP in the peri-operative period, smaller body surface area and smaller LV cavity. 2 It emphasizes the evaluation of an additional LVOT or mid-cavitary gradient in a patient with elevated aortic prosthetic valve gradient, where opting for isolated valve replacement alone may not suffice in providing relief from symptoms, and additional surgical myectomy may be necessary.
Author Contribution
SSK (Conceptualization: Equal; Formal analysis: Lead; Writing – original draft: Lead; Writing – review & editing: Lead); SM (Conceptualization: Equal; Investigation: Equal; Supervision: Equal); VK (Conceptualization: Equal; Formal analysis: Lead; Writing – review & editing: Lead); SKG (Conceptualization: Equal; Formal analysis: Lead; Writing – review & editing: Lead).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Considerations
The study was conducted by the ethical standards in the 1964 Declaration of Helsinki and its amendments. Informed written consent was taken from the patient concerned. No patient identity particulars have been disclosed.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent for Publication
Necessary patient consent for publication was obtained.