
Abstract
Introduction
Cardiac conduction disorders can interrupt the normal electrical conduction in the heart and cause a decrease or cessation of pulse generation and a fall in organ perfusion in the body. This can lead to significant morbidity and mortality. This study was conceived to illustrate the clinical profile, presentation, management, and complications of bradyarrhythmia therapy in this population.
Methods
This descriptive cross-sectional study included prospective and retrospective data over a period of 16 years. All patient’s demographic data and data of any complications and adverse outcomes were documented.
Results
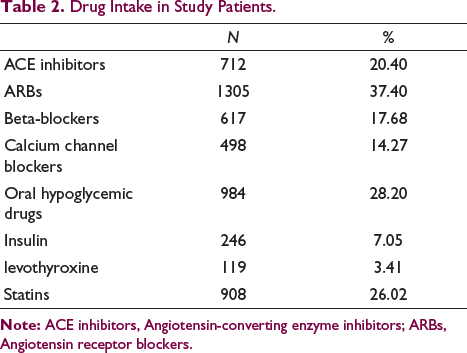
A total of 3489 cases having permanent pacemakers (PPMs) implanted in them were included in this study. There were 2254 (64.6%) men and 1235 (35.4%) were women. Age of the patients ranged from 25 to 100 years with a mean age of 62.9 ± 11.14 years. Mean ejection fraction of patients was 59.3 ± 2.57%. The indication for PPM implantation was complete heart block in 2079 (59.6%), sick sinus syndrome in 422 (12.1%), Mobitz type 2 heart block in 345 (9.9%), symptomatic left bundle branch block in 295 (8.5%), symptomatic bifasicular block in 176 (5.0%), symptomatic trifascicular block in 109 (3.1%), vasovagal syncope with symptomatic sinus bradycardia in 21 (0.6%), left anterior hemiblock with syncope in 3 (0.1%), and atrial fibrillation with heart block in 11 (0.3%) patients. Cardiac syncope was presented in 80%, presyncope in 15%, and 5% presented with features of chronotropic incompetence. No significant seasonal variation was observed in the incidence of PPM implantation. Single-chamber PPM was implanted in 58.8% and dual-chamber PPM in 41.2% of the cases. PPM-related complications were seen in 139 (3.98%) of the cases. Pneumothorax was seen in 21 (0.6%) of the cases, lead displacement in 39 (1.12%), lead replacement in 31 (0.89%), pocket site infection in 20 (0.57%), generator extrusion in 25 (0.70%), and lead extrusion in 3 (0.08%).
Conclusion
Conduction disorders affect men more than women and complete heart block is the most common form of conduction disorder in our population. There has been a significant improvement in bradyarrhythmia detection and its management, leading to wider penetration and safety of device therapy provided to the patient population.
Introduction
Bradyarrhythmia therapy involves the implantation of the permanent pacemaker (PPM) device. PPM is a small implantable electronic device that delivers timed and precise electrical impulses through electrodes in the heart to stimulate the cardiac tissue to maintain or restore a normal heart rate.1, 2
In 1952, Paul Zoll, a Boston cardiologist, described an effective means of supporting patients with conduction diseases by means of an external artificial pacemaker. He is credited for ushering cardiology into the modern era of clinical cardiac pacing. Paul Zoll designed an external tabletop pacemaker called Electrodyne PM-65, which was comprised of an electrocardiograph for cardiac rhythm monitoring and a pulse generator for cardiac pacing. This used transcutaneous pacing with electrodes delivering impulses at a pulse width of 2 ms and 50–150 volts via an alternating current. The electrodes caused skin irritation and the pacing could be maintained for a short period of time only.3, 4 With advancement in technology, miniaturization of electronic devices, development of device implantation techniques, tremendous improvement in the device performance, and ease of implantation, PPM implantation has become the standard therapy for long-term and effective treatment of bradyarrhythmias. Studies have shown a steady growth of 4%–5% in the number of devices implanted yearly worldwide.5, 6
The major indication of implantation of a pacemaker device includes sinus nodal dysfunction, atrioventricular (AV) nodal dysfunction causing heart block, atrial fibrillation with AV block and post-myocardial infarction (MI) heart block, besides other infrequent causes. 7 The incidence of pacemaker implantation increases with age as the incidences of conduction diseases increase with advanced age.8, 9
This study aimed to evaluate the clinical profile, etiology/indication, seasonal variation, device therapy offered and its complications, of patients presenting with symptomatic bradycardia needing PPM implantation.
Methods
A descriptive cross-sectional study included all the patients who had PPMs implanted from the year 2006 to 2021 at this center. This study included retrospective data from October 2018 to January 2006 and prospective data from November 2018 to December 2021, a total of 16 years. The ethical clearance for the conduction and design of the study was sought and granted by the Institutional Ethical Committee (IEC). The pacemaker implantation was performed in a cardiac catheterization laboratory by a team comprising a cardiologist, a cardiac technician, and a nurse. The procedure was performed under local anesthesia using an extrathoracic subclavian or cephalic vein route. All the patients were given an injection of teicoplanin 400 mg 1 hour before the procedure.
Inclusion Criteria
All adults (age >18 years) at the time of PPM implantation were included.
Patients getting a pacemaker implant for symptomatic bradyarrhythmia during the time period of January 2006 to December 2021 were included.
Exclusion Criteria
Congenital heart block.
Post-cardiac surgery conduction disorders.
Pacemaker generator replacements.
Patients getting cardiac resynchronization therapy devices.
Patients getting implantable cardioverter defibrillator (ICD) devices.
All the patient’s clinical history, physical examination, electrocardiogram, Holter recordings, echocardiographic parameters, indication of PPM implantation, and type of pacemaker device implanted were recorded.
Statistical Analysis
Data were expressed as the number of patients and categorical variables compared using the chi-square and Fisher’s exact test. Student’s t-tests was used for continuous variables. In order to avoid the potential influence of a festival or holiday on data analysis, a comparison was made of the seasonal (3 months) distribution of pacemaker implantation instead of the monthly distribution. After obtaining the data in prescribed format, data were fed into MS Excel, and statistical analysis was performed using the SPSS software program for Windows, version 23. A value of P < 0.05 was considered statistically significant.
Results
A total of 3497 cases of PPM implantations were performed in this center during this period of 16 years from January 2006 to December 2021. Among these were six cases of congenital heart block, one case of post-tetralogy of fallot (TOF) surgery, and one case of carotid hypersensitivity syndrome which were excluded from the study. A total of 3489 cases were included in the study and analyzed for various conduction defects and their seasonal distribution and device therapy received. Prevalence of PPM in the valley has increased from 0.1 per 1000 population in 2001 to 0.57 per 1000 population in 2021. Incidence of PPM implantation was calculated at 5.09 per 100000 population per year. Out of 3489 cases enrolled 2254 (64.6%) were men and 1235 (35.4%) were women. The age of cases ranged from 25 to 100 years with a mean age of 62.9 ± 11.14 years (mean age for men = 63.9 ± 11.35 years and women = 62 ± 11.9 years). Demographic profile and associated comorbidities of the study population are given in Table 1.
Demographic Profile and Comorbidities of the Study Population.
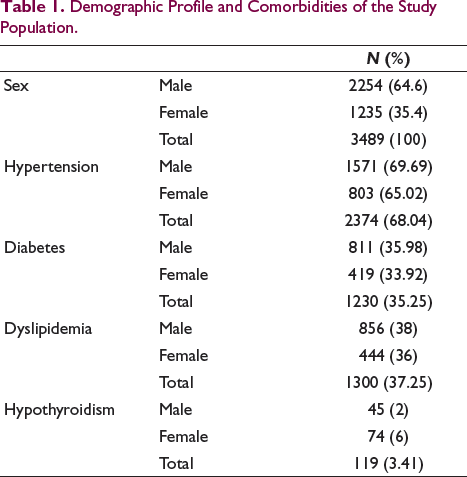
The different medication intake in the study population is given in Table 2.
Drug Intake in Study Patients.
Echocardiography revealed majority of patients having normal ejection fraction with mean EF of 59.3 ± 2.57%.
The etiology and indications of PPM implantation are given in Table 3.
Etiology and Indication of PPM Implantation.
The associated structural heart diseases with these patients include ASD secundum in two patients, pulmonary stenosis in one patient, aortic stenosis in one patient, rheumatic heart disease in three patients, and L-Transposition of Great Arteries (L-TGA) in one patient.
Cardiac syncope was the most common presentation with 80% of the study population having this clinical feature as a presenting symptom. Presyncope presented clinical features in 15% of the cases and 5% of the cases presented with features of chronotropic incompetence.
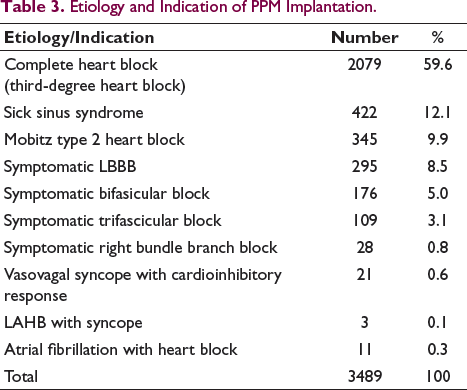
The yearly distribution of pacemaker implantation along with the type of pacemaker (dual vs. single chamber) is given in Figure 1.
Yearly Distribution of Permanent Pacemaker.
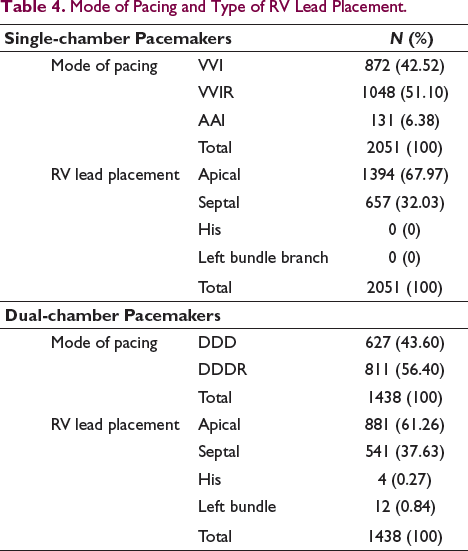
Single-chamber pacemaker implantation (SCPM) was more common, with 2051 (58.78%) cases receiving single-chamber pacemakers while dual-chamber pacemakers (DCPM) were implanted in 1438 (41.22%) cases. However, dual-chamber pacemaker implantation rates progressively increased and were consistently higher than single-chamber pacemakers after 2014. This was mainly driven by the introduction of various healthcare schemes by the Government. All the patients who were given PPM for bradyarrhythmia reported improvement in their symptoms on follow-up. There was no significant seasonal difference between SCPM and DCPM implantation rates. The mode of implanted pacemakers and type of RV lead implantation is given in Table 4.
Mode of Pacing and Type of RV Lead Placement.
Seasonal variation in the pacemaker implantations and associated etiology is given in Table 2. There was no seasonal variation in pacemaker implantation rates, although the number of pacemakers implanted in spring and summer was numerically higher (910 and 909) than in winter and autumn (796 and 874, respectively), the difference was not statistically significant (P = 0.99) as shown in Table 5.
Seasonal Variation in PPM Implantation and Associated Etiology.
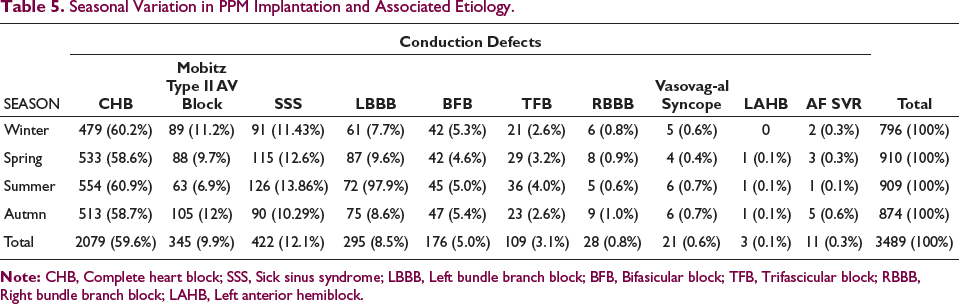
No significant seasonal variation was observed in the occurrence of conduction defects needing pacemaker implantation, However, the incidence of sick sinus syndrome (SSS) was significantly higher in women, 325 (77%) as compared to men, 97 (23%) P < 0.00001. Sixteen (0.45%) patients with CHB had a history of coronary artery disease at presentation. Atrial fibrillation was present in 22 (5.3%) patients of SSS at presentation. Two patients with CHB had associated ASD secundum.
Comprehensive data on pacemaker-related complications were also collected and are given in Table 6.
Pacemaker-Related Complications.
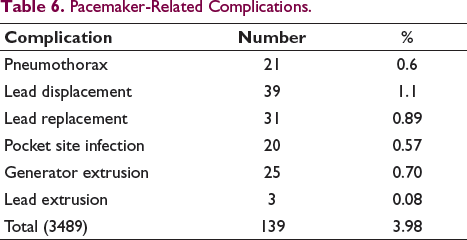
Overall PPM-related complications were seen in 139 (3.98%) cases. Pneumothorax was seen in 21 (0.6%) cases. There were 70 (2.0%) cases of lead-related complications which included 39 (1.11%) cases of lead displacement, which were repositioned and 31 (0.89%) cases of lead replacement. Out of 31 (0.89%) cases of lead replacement, 18 (0.52%) were due to lead fracture and 11 (0.32%) due to insulation break and 2 (0.05%) cases due to lead induced perforation. Pocket site infection was seen in 20 (0.57%) cases for which the pacemaker was removed from the original left sided prepectoral pocket and a new pacemaker implanted in the right sided pocket under the cover of antibiotics. Where old pacemaker generator was placed in the right sided pocket and had got infected, new implantation was done on the left side. Generator extrusion/exteriorization was seen in 25 cases and lead extrusion in 3 cases, respectively. Out of 139 pacemaker-related complication 108 (77.69%) complication occurred in the first 10 years of the study, while the other 31 (22.32%) complication occurred in the last 6 years of the study.
Discussion
This descriptive, cross-sectional observational study was one of the largest studies conducted over a period of 16 years in our population. The study revealed that the prevalence of PPM in the valley has increased from 0.1 per 1000 population in 2001 to 0.57 per 1000 population in 2021. As predicted, prevalence has increased more than twice in the last decade. 10 Incidence of PPM implantation was calculated at 5.09 per 100000 population per year. CIED (cardiac implantable electronic devices) use has registered a remarkable jump world over in the last decade. With an average of 300 implants of CIED per million of the population, North America & Europe has the highest implant rates in the world.11, 12, 13 There is a wide difference in the CIED implantation rates between developed and developing countries. In our country, with the limited data available, the implant rates are a minuscule 25 implants per million of the population and nearly the same rates are seen in other developing countries. The main contributors for low utilization of device therapy include weak healthcare infrastructure, fewer trained cardiologists to implant these devices in far-off places in this vast country, high cost, and lack of health care insurance in most cases. Another factor responsible for low utilization of these therapies includes their use as only life-saving measure and not for quality-of-life improvement. 14
In presence of the limited data on incidence and prevalence of pacemakers in India, this study focuses on the epidemiology of pacemaker implantation, indications and seasonal variation in Kashmir Valley. Kashmir Valley is inhabited by a relatively homogenous population with dietary practices and living conditions that do not differ significantly across the Valley.
In our study, pacemaker recipients were significantly older. Mean age of implantation was 62 ± 11.14 years. These findings are consistent with findings of the study by Lone et al., 15 which was a 10-year review of pacing in north India to analyze the continuous rise in the incidence of pacing in this part of country. In their study, 532 patients implanted with permanent pacemakers were evaluated over a decade. The age of patients ranged from 6 to 85 years with majority of patients belonging to age group of 55–70 years. These number were also comparable to a single center study conducted in the North-West Provinces of Iran by Akberzadeh et al., where mean age of male and female patients were 64.9 ± 12 and 69.5 ± 14 years, respectively. 16
In our study population, among the patients undergoing pacemaker implantation, number of male patients was higher than the female patients (64.6% vs. 35.4%). These findings were similar to the study by Narayan et al., 17 in which majority (773, 73.41%) of the patients were male. Most (715, 67.9%) of the patients were belonging to more than 60 years of age. These findings were also similar to the findings by Lone et al., 15 wherein men and women appeared in the ratio of 2:1. These data were also identical to the 11th world survey for cardiac devices where male population was predominantly higher than the female population (68% vs. 32%). 13 The results were also comparable to a study by Kumar et al., in their study the mean age of the population was 60.1 ± 16.7 years. Of the total population 881 (56.8%) were men. 18
In our investigation, SCPM was more prevalent, accounting for 58.78% of cases, while DCPM represented 41.22% of implants. These results align with the study conducted by Shenthar et al., 14 where single-chamber (VVI) pacemakers constituted 54% of implants. Similar findings were reported by Bhat et al., 19 in their study, where single chamber PPM was more common (62.5%) compared to dual-chamber PPM (28.5%). The higher prevalence of single chamber pacing mode is attributed to its relatively lower cost. However, as indicated in other studies, with increased affordability and availability, there is a growing tendency for PPM with DDDR and VVIR mode implants. It is noteworthy that interstate variation is expected in PPM type and pacing mode, resembling data obtained from earlier reports in other developing countries. 13 This pattern contrasts with trends observed in developed nations, highlighting underlying economic issues in healthcare and the absence of health insurance in developing countries. This suggests that PPMs are predominantly implanted when essential for survival rather than for an improved quality of life, as commonly observed in the general population in India.
There was no significant seasonal variation between single and dual chamber PPM implant rates. However, like other studies that compared trends in PPM, our study also showed that the use of dual-chamber pacemaker has increased progressively over time, reflecting improvement in socioeconomic conditions, decrease in the cost of PPM devices, increased availability of trained cardiologists.
Our study showed that the number of pacemakers implanted in spring and summer were numerically higher (910 and 909) than winter and autumn (796 and 874), respectively; however, the difference was not statistically significant. Our study partly agrees with the study by Akberzadeh et al., 16 which revealed increased rates of implantation in winter and spring in North West Iran, however, the later study is limited by a small sample size. In their study, they showed that incidence of conductive disorders increased during winter and spring. North-West provinces of Iran has cold mountain climate and most of cold temperatures are in winter and early spring. In the subgroup analysis of their study, a rise in the incidence of conductive disorders was observed, specifically linked to the increased presence of women in the population due to seasonal migration. Interestingly, among the male population, the incidence actually decreased. The conclusion drawn from this observation is that, in the context of a demographically homogeneous study population, the elevated incidence of conduction disorders during seasonal variation is unlikely to be attributed to viral infections or myocarditis. Instead, the findings suggest that an unidentified factor may be contributing to this seasonal variation
In our study, the indications for PPM implantation were parallel to that in the New Zealand registry., 20 in terms of order of indication, where degenerative complete heart block was the prime indicator for implantation (59.6% vs. 29%); followed by SSS (11.9% vs. 19%) and second-degree AV block (9.9% vs. 11%). These findings are also consistent with the study by Kumar et al., 18 which revealed degenerative complete heart block, the prime indication for pacemaker implantation, in 68.3% patients; followed by sick sinus syndrome affecting 9.0% patients and 2:1 AV block in 7.8% patients. The findings of our study were also consistent with the study by Lone et al., 15 where indications for pacemaker implantation were complete heart block in 48.12%, SSS 19.17%, symptomatic bifascicular block 12.96%, Mobitz type II 2nd degree heart block in 7.14%. However, the findings in our study were contradictory to Pacemaker registry of Netherlands, 21 which showed Sick Sinus Syndrome as the prime indicator (42.3%) for pacemaker implantation followed by heart block (38.9%). This could be due to more aged population (mean age in men = 72.3 years and women = 75.1 years) with a significant number of women (47.8%) in the Netherland registry. This study also revealed that SSS is significantly higher in women. However, another European registry, the Swedish pacemaker registry. 22 reported AV conduction disorders (38%) as the commonest cause followed by SSS (34%).
Our investigation revealed that there was no notable seasonal fluctuation in the incidence of specific cardiac conduction defects (P = 0.27). Notably, SSS demonstrated a higher frequency in women compared to men, aligning with data already present in this regard. In our study, a substantial statistical contrast was observed between genders among symptomatic SSS cases, with 321 (77%) women and 95 (23%) men, yielding a P-value of <0.00001.
With advances in device technology, implantation techniques, operator experience and progressively increasing number of PPM implantations every year, safety of PPM implantation has improved and complications have decreased. Overall PPM -related complications in our study were seen in 139 (3.98%) cases. These include pneumothorax in 21 (0.6%) cases, which were managed by intercostal tube drainage. Lead perforation cases were managed by first placing and fixing a second permanent pacing lead, retrieval of the perforating lead, followed by drainage of associated pericardial effusion (hemopericardium) by closed pericardiocentesis. Both patients are doing well on follow-up. Generator extrusion occurred in 0.7% cases, lead extrusion in 0.08% and pocket site infection was seen in 0.57%. These findings were comparable to the study by Aggarval RK, Connelly et al., 23 where lead displacement was seen in 1.4%, generator extrusion in 0.5% and pocket infection was seen in 0.9%. CIED infection remains one of the most feared and difficult to treat complication of device implantation with international literature estimating the incidence rate of 0.5%–1% for PPMs. Incidence increases with increases in the complexity of devices like ICDs (1.7%) and resynchronization devices (9.5%). 5 The decreased incidence of infections was probably a result of thorough preoperative skin preparation, the application of a topical antibiotic spray in the pacemaker pocket, administration of injectable antibiotics in the perioperative period, and vigilant postoperative monitoring. The effectiveness of these measures was also supported by the study of Mures et al. 24 who in their study found an apparent benefit with perioperative antibiotics, with seven of nine pocket infections occurring in patients randomized to receive no antibiotics. Their pocket infection rate was 2.1%. Furthermore, Mounsey et al. 25 reported a reduction in reoperation rate for infection, with 12 of 13 pocket infections occurring in patients not receiving antibiotic prophylaxis; however, they found no benefit in the subgroup of patients with the highest risk of infection (those with temporary pacing electrodes).
Majority of the pacemaker-related complication occurred in the initial period of the study, followed by a steady fall in the complication rates in the subsequent period of the study. This is due to improved pacemaker implantation techniques like using an extrathoracic axillary vein puncture instead of subclavian vein puncture for lead placement, which reduces the chances of pneumothorax and hemothorax. 26 Additionally, use of active fixation lead in the later part of the study reduced the incidence of lead displacement. 27
Advances in technique, technology, aging, and prolonged survival have led to a significant increase in the prevalence of PPM devices as bradyarrhythmia therapy worldwide. However, due to financial constraints and inadequate availability of trained cardiologists in the developing world, it continues to remain meager in comparison to the developed world.
Limitation of the Study
The main limitation of this study was that this was a single-center study on a fairly homogeneous study population. Another limitation was that it included a significant amount of data that were analyzed retrospectively.
Conclusions
This study concluded that conduction disorders predominantly affect men than women and complete heart block is the most common cause for receiving PPM in our population. No significant seasonal variation could be demonstrated in incidence of various conduction disorders. Our study demonstrates the positive impact of the tremendous advances made in the field of arrhythmia therapy, especially bradyarrhythmia therapy on patient outcomes. There has been a steady increase in the incidence and detection of various conduction disorders in all the reported literature. This study also demonstrated a significant fall in the complication rate associated with pacemaker implantation and improved longevity of devices, contributed by better implantation techniques and increased operator experience.
List of Abbreviations
PPM, permanent pacemaker; CHB, complete heart block; AV block, atrioventricular block; BFB, bifasicular block; TFB, trifascicular block; SSS, sick sinus syndrome; LBBB, left bundle branch block; RBBB, right bundle branch block; LAHB, left anterior hemiblock; SCPM, single chamber pacemaker; DCPM, double chamber pacemaker.
Footnotes
Acknowledgements
The authors thank the technical staff of Cath-lab SKIMS especially Syed Bilal and others for their immense support during the conduction of this study.
Consent for Publication
Written consent obtained from the patients for publication of this manuscript. The copy is available with the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The study design was cleared and approved the Instructional Ethical Committee (IEC) of SKIMS Soura Srinagar. Informed Written consent was obtained from all the patients before participation in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.