
Abstract
Truncus arteriosus is an exceedingly rare congenital heart disease involving the conotruncal septum of the developing heart. Clinical presentations vary depending on associated anomalies. Surgical management is extremely challenging and differs with anatomic subtypes. We present a case of truncus arteriosus––Vaan Praagh type A4, quadricuspid truncal valve with moderate truncal stenosis and regurgitation, type B interrupted aortic arch who underwent bilateral pulmonary artery banding.
Background
Truncus arteriosus (TA) is a rare congenital heart defect where failure of conotruncal septum development leads to failure of separation of two great arteries. Neural crest cells fail to migrate to the distal bulbus cordis of the developing heart to form the aorticopulmonary septum (spiral septum). The prevalence of TA is 76 per million live births, representing 1.19% of all congenital heart disease. 1 Prevalence of interrupted aortic arch is about three per million live births. 2 The combination of type B interrupted aortic arch with TA, also classified as Vaan Praagh 3 type A4, is extremely rare consisting of 12% of all cases of TA. However, association with quadricuspid truncal valve in Vaan Praagh type A4 TA is not yet reported in literature.
Case
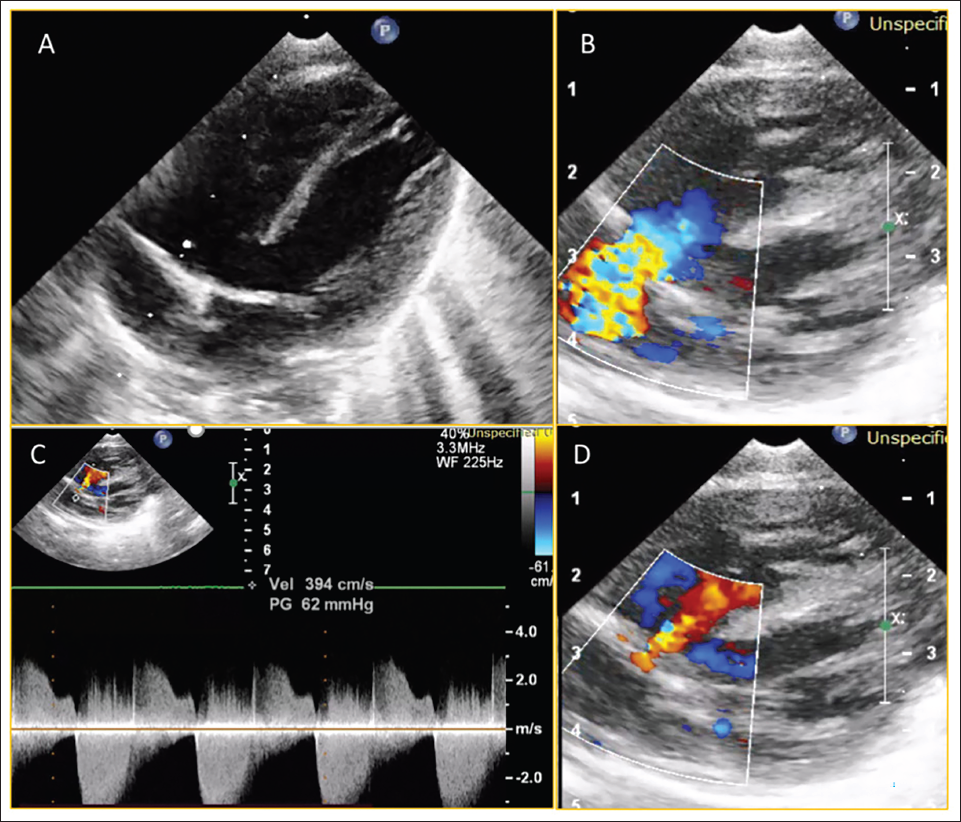
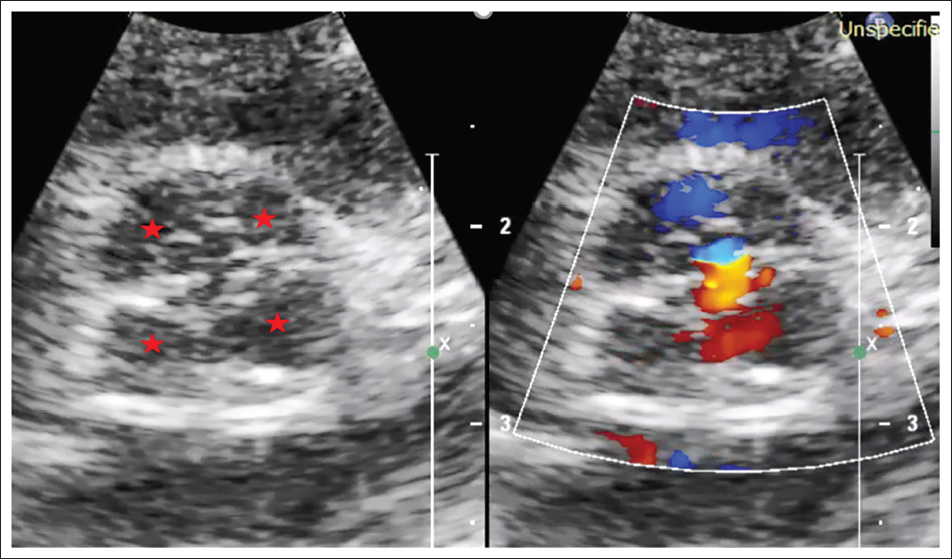
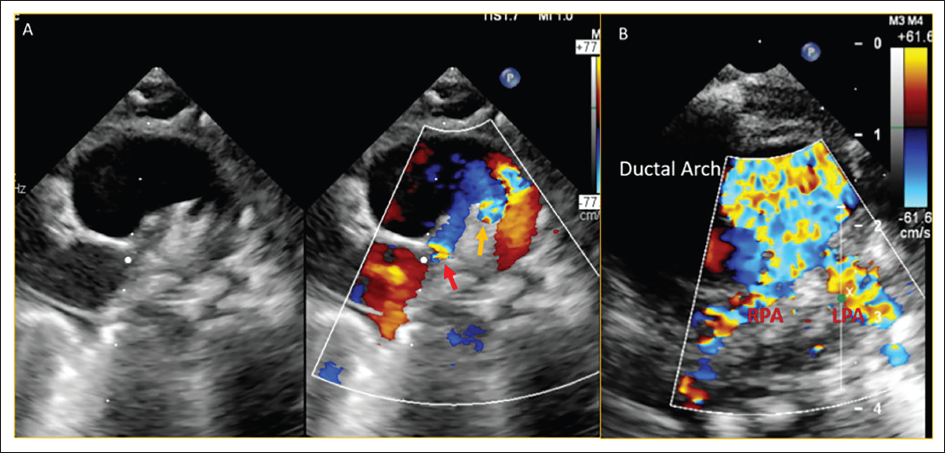
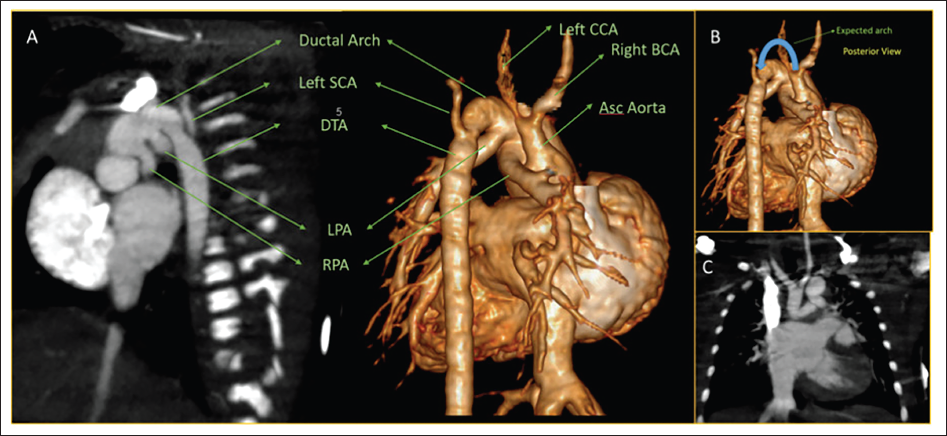
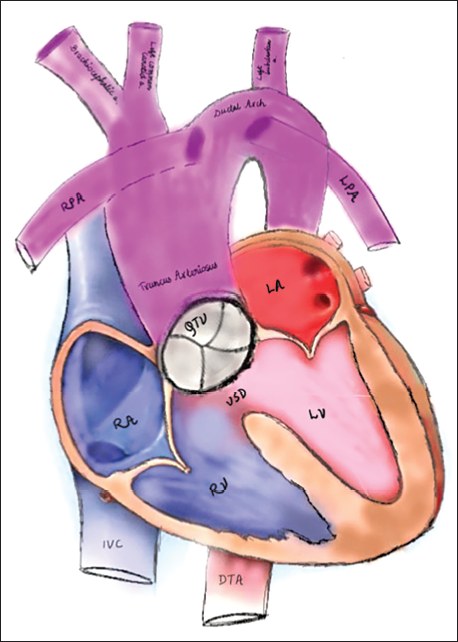
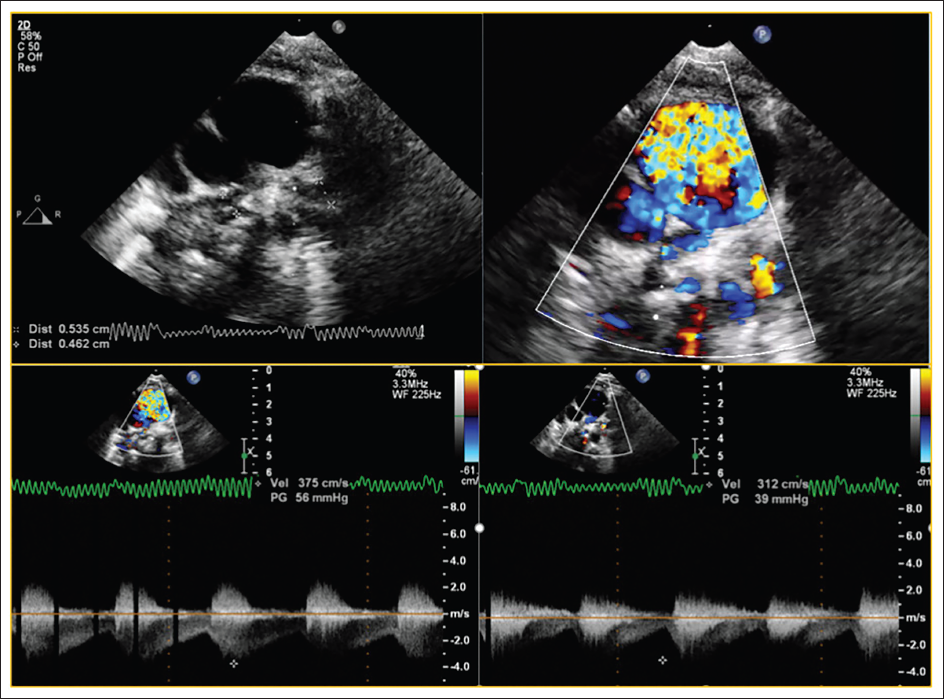
A 4-day-old girl with a history of a positive anomaly scan at seven months of gestation, was delivered at 35 weeks of gestation. After birth, there was no cyanosis, spells, no breathing or feeding difficulty, and no features suggestive of heart failure. Clinical examination showed 93% oxygen saturation in room air with a constant ejection click, grade 3 ejection systolic murmur at the aortic area. Transthoracic echocardiogram showed large subarterial ventricular septal defect (Figure 1A), single outflow with quadricuspid truncal valve (Figure 2) with mild-moderate truncal regurgitation due to non-coaptation of leaflets and moderate truncal stenosis (Figure 1B–D and Figure 2), type B interrupted aortic arch with bilateral pulmonary arteries originating separately from ductal arch (Figure 3A and B). Cardiac CT showed a common trunk continuing as ductal arch after giving right brachiocephalic trunk and left common carotid artery, type B interrupted aortic arch, and both left and right pulmonary arteries originating from the posterior and inferior aspect of ductal arch with no branch pulmonary stenosis (Figure 4A–C). Hence, the diagnosis of TA––Vaan Praagh A4 associated with quadricuspid truncal valve with moderate truncal stenosis and mild-moderate truncal regurgitation was made (schematic depiction in Figure 5). We suggested truncal repair with truncal valve repair for the patient. However, the patient developed hemodynamic instability during surgical repair immediately after anesthesia induction. Hence, bilateral pulmonary artery (PA) banding was done and staged repair of truncus was planned. On follow up, she had failure to thrive and functioning PA band (Figure 6). Cardiac CT was planned to reassess PA growth and planned for definitive repair. However, she was lost to follow-up.
(A) Modified A4C View Showing the Large Subarterial Ventricular Septal Defect; (B) Turbulence in Outflow Tract at Valve Level; (C) Moderate Truncal Stenosis with a Peak Gradient of 62 mm Hg; (D) Mild-moderate Truncal Regurgitation Seen on the Same View.
Schematic Depiction of the Anatomy of the Index Case.
Post Bilateral Pulmonary Artery Banding Showing Significant Gradients with Functioning Pulmonary Artery Band.
Discussion
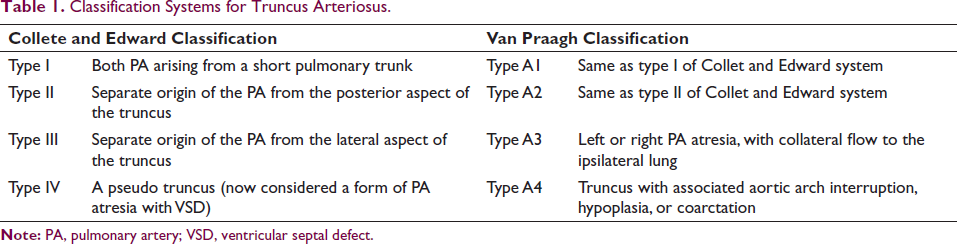
Truncus arteriosus is a conotruncal abnormality where the ascending aorta and pulmonary trunk fail to separate during the development of the fetus, characterized by a single arterial outlet from the heart overriding the ventricular septum and supplying coronary, pulmonary, and systemic circulations. Very often it is associated with valvular abnormality. Most often truncal valve is tricuspid followed by quadricuspid or bicuspid which leads to either stenosis or regurgitation hemodynamically. Almost all patients have a nonrestrictive subarterial ventricular septal defect with the absence of a conal septum. The prevalence of TA is 76 per million live births and represents 1.19% of all congenital heart disease. DiGeorge syndrome and chromosome 22q11 deletion have a well-established relation with the anomaly. 4 The original system by Collett and Edward, 5 divided TA into four types from Type I to IV. This classification was further modified by Van Praagh. 6 Both the classification systems are briefed in Table 1. Our patient falls under Van Praagh Type A4 because of the presence of type B interrupted aortic arch and both pulmonary arteries arising separately from the ductal arch. Our patient additionally had a quadricuspid truncal valve with moderate truncal stenosis with mild-moderate truncal regurgitation. Verma et al. 7 reported three cases of Type A4 TA, none of which had been reported to have a quadricuspid truncal valve. As the presentation is variable at different ages from childhood to adulthood, early diagnosis and surgical repair are crucially important for survival. Corrective surgery for a common arterial trunk with an interrupted aortic arch is challenging and preoperative planning is crucial. In surgical repair, pulmonary arteries are detached from the parent trunk and connected to the right ventricle by a valved homograft. Associated critical anomalies like interrupted aortic arch or obstructive lesions (like a truncal valve) are repaired in the same setting. Conduit stenosis or regurgitation, branch PA stenosis, neoaortic truncal valve insufficiency or stenosis, ventricular septal defect patch leak, and aortic arch obstruction are among repair-related complications. We could not perform definitive surgery due to hemodynamic instability upon induction by anesthetic agents forcing us to do palliative surgery in the form of bilateral PA banding.
Classification Systems for Truncus Arteriosus.
Conclusion
Truncus arteriosus––Vaan Praagh A4 is extremely rare, and its association with quadricuspid truncal valve is even rarer. Managing such patients is extremely challenging, often requiring staged palliative surgery. We possibly report one of the first few cases of TA––Vaan Praagh A4 associated with QTV and suggest more sensitization among cardiologists.
Author Contribution
SM (Conceptualization: Equal; Formal analysis: Lead; Writing – original draft: Lead; Writing – review & editing: Lead); DSK (Conceptualization: Equal; Investigation: Equal; Supervision: Equal)
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Statement
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
The written informed consent was obtained.
Data Availability Statement
No new data were generated or analysed supporting this research.