
Abstract
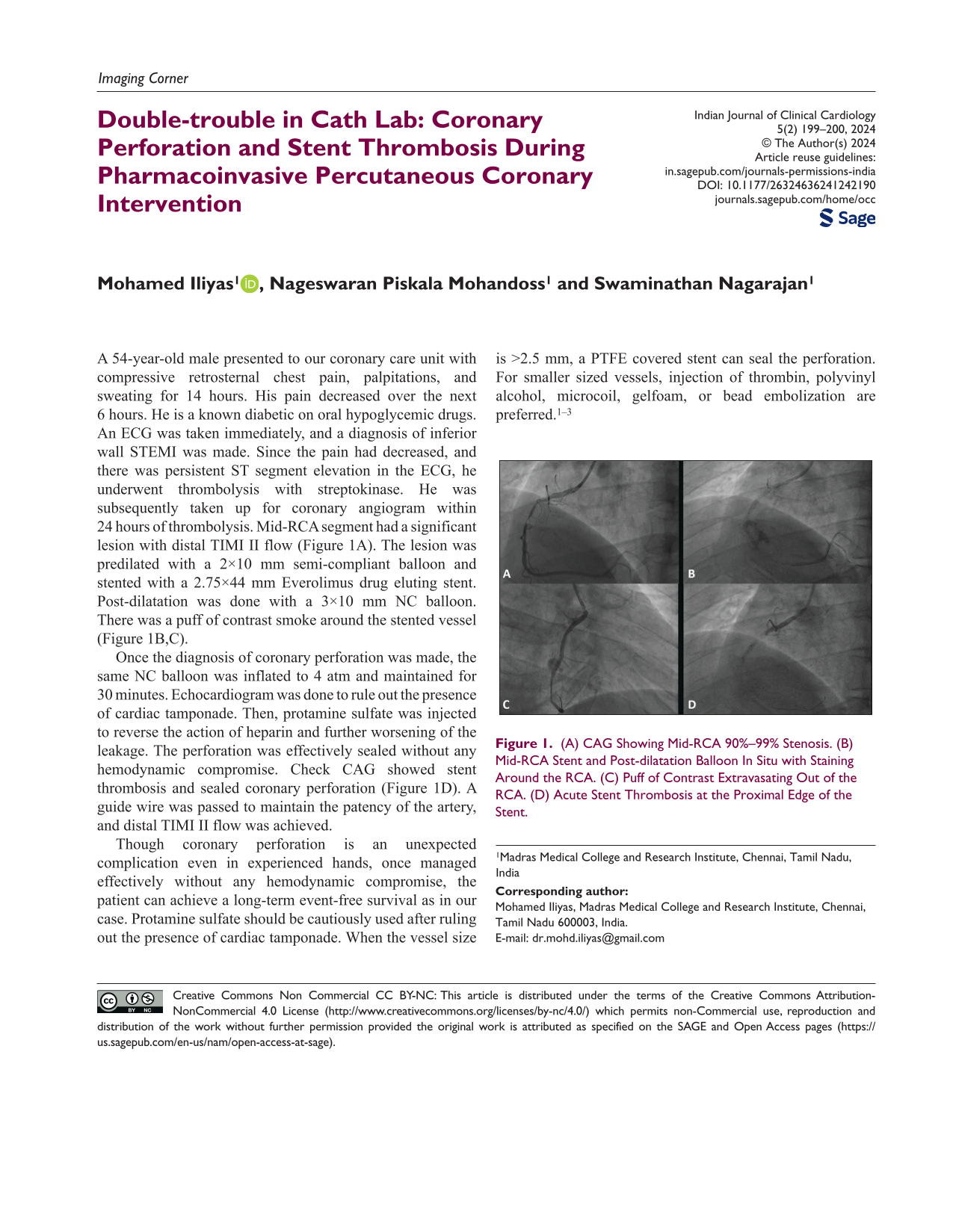
A 54-year-old male presented to our coronary care unit with compressive retrosternal chest pain, palpitations, and sweating for 14 hours. His pain decreased over the next 6 hours. He is a known diabetic on oral hypoglycemic drugs. An ECG was taken immediately, and a diagnosis of inferior wall STEMI was made. Since the pain had decreased, and there was persistent ST segment elevation in the ECG, he underwent thrombolysis with streptokinase. He was subsequently taken up for coronary angiogram within 24 hours of thrombolysis. Mid-RCA segment had a significant lesion with distal TIMI II flow (Figure 1A). The lesion was predilated with a 2×10 mm semi-compliant balloon and stented with a 2.75×44 mm Everolimus drug eluting stent. Post-dilatation was done with a 3×10 mm NC balloon. There was a puff of contrast smoke around the stented vessel (Figure 1B,C).
(A) CAG Showing Mid-RCA 90%–99% Stenosis. (B) Mid-RCA Stent and Post-dilatation Balloon In Situ with Staining Around the RCA. (C) Puff of Contrast Extravasating Out of the RCA. (D) Acute Stent Thrombosis at the Proximal Edge of the Stent.
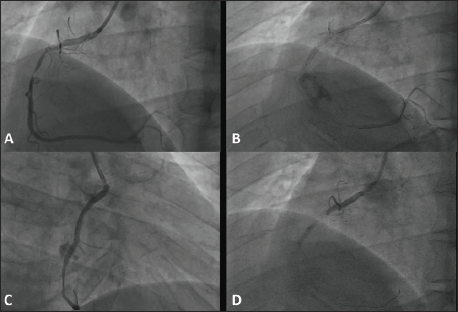
Once the diagnosis of coronary perforation was made, the same NC balloon was inflated to 4 atm and maintained for 30 minutes. Echocardiogram was done to rule out the presence of cardiac tamponade. Then, protamine sulfate was injected to reverse the action of heparin and further worsening of the leakage. The perforation was effectively sealed without any hemodynamic compromise. Check CAG showed stent thrombosis and sealed coronary perforation (Figure 1D). A guide wire was passed to maintain the patency of the artery, and distal TIMI II flow was achieved.
Though coronary perforation is an unexpected complication even in experienced hands, once managed effectively without any hemodynamic compromise, the patient can achieve a long-term event-free survival as in our case. Protamine sulfate should be cautiously used after ruling out the presence of cardiac tamponade. When the vessel size is >2.5 mm, a PTFE covered stent can seal the perforation. For smaller sized vessels, injection of thrombin, polyvinyl alcohol, microcoil, gelfoam, or bead embolization are preferred.1–3
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.