
Abstract
Background
Cardiorenal syndrome is a disorder in which renal function is affected by heart failure (HF) or vice versa. It occurs in 20% of HF patients. The most common reason for hospitalization is acute decompensation (ADHF). Diuretics and inodilators are the standard of treatment in the management. Our objective was to demonstrate that levosimendan is more effective than dobutamine in improving the outcome of ADHF patients with a low ejection fraction (EF) and impaired kidney function.
Material and methods
The study was carried out between January to December 2022. Patients with ADHF, a low EF (<40%) on echocardiography, and decreased renal function (estimated glomerular filtration rate [eGFR] >15 and <60 mL/min/m2) were included. All patients have given consent. The study was approved by the institutional ethical committee. The estimated study sample size was 18 in each group, and as the study continued, we enrolled 60 patients, who were divided into two equal groups (30 in each). The patients were assigned either levosimendan or dobutamine based on preassigned numbers in the software. The clinical characteristics (serum creatinine, eGFR, EF, cardiac output, and cardiac index) were measured on the first, seventh, and at one month (30 days).
Results
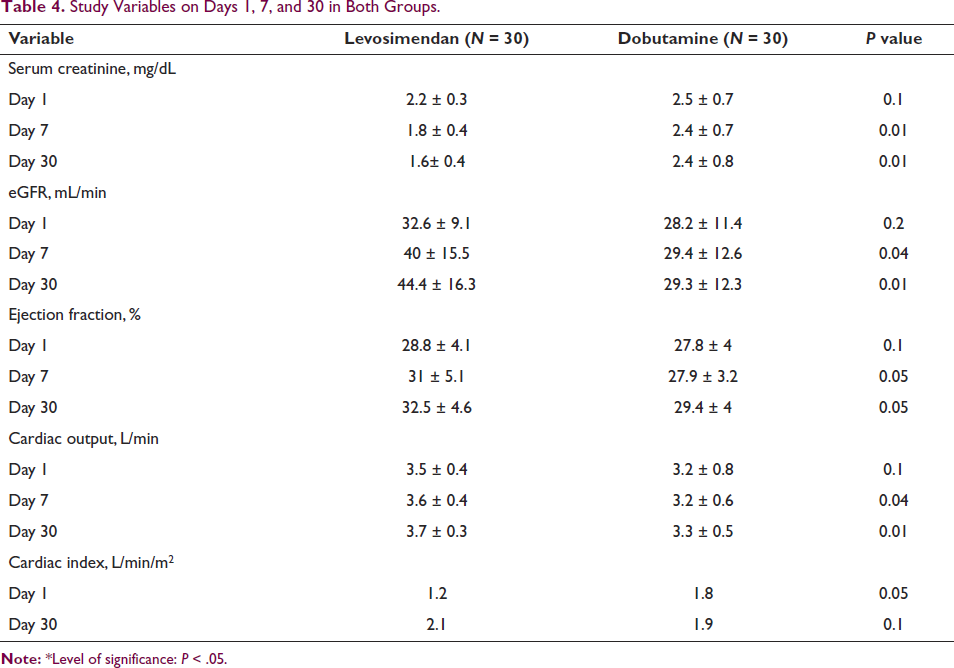
Of the 60 patients, 40 were men and 20 were women. The mean age was (50 ± 8.9 vs 50.8 ± 11.2) years. Of the comorbidities, hypertension was seen in 83.3% followed by diabetes (56.7%). Serum creatinine levels in both groups at admission and 30 days were (2.2 ± 0.3 vs. 2.5 ± 0.7, P = 0.1) and (1.6 ± 0.4 vs. 2.4 ± 0.8, P = 0.05). The eGFR of both groups at admission and 30 days follow up was (32.6 ± 9.1 vs. 28.2 ± 11.4, P = 0.2) and (40 ± 15.5 vs. 29.4 ± 12.6, P = 0.05). At 30 days, the predetermined outcomes in terms of improvement in EF, cardiac output, improved eGFR and cardiac index were better in the levosimendan compared to dobutamine group significantly.
Conclusion
In ADHF patients with decreased EF and poor renal function, levosimendan improved renal and cardiac indices more than dobutamine at 30 days of follow up.
Keywords
Introduction
Although acute decompensated heart failure (ADHF) continues to be a primary reason for hospitalization worldwide, it is still not apparent how these patients should be treated. About 15% of admissions for emergency care are attributable to this condition. Cardiorenal syndrome (CRS), which complicates 20% of cases of heart failure (HF), is the condition in which renal impairment results from HF and vice versa. Diuretics and inodilator are the standard of care for these patients. 1 Dobutamine, is the age old intrope with action through beta-1 receptor of the heart thereby increasing cardiac contractility and stroke volume. However, it increases intracellular cyclic adenosine monophosphate within the failing heart and is associated with an increased risk of death and other cardiovascular events.1 The advantages of levosimendan are it is, a calcium sensitizer, an intrope that enhances renal blood flow, vasodilation and has antiinflammatory actions against tubular injury. 1 The facilitation of an adenosine triphosphate-dependent potassium channel opening is responsible for its vasodilatory action. 2 Its action is independent of interaction with adrenergic receptors, a unique action compared to other inotropes.3, 4 This study aimed to examine the renal effects of the two medications in ADHF patients, presuming that levosimendan would be well tolerated and relieve symptoms compared to dobutamine.
The Aim of the Study
To determine whether levosimendan produces superior clinical and hemodynamic results than dobutamine when used to treat individuals with ADHF who have a low ejection fraction (EF) and impaired renal function.
Methodology
The study was conducted among the patients admitted with a diagnosis of ADHF in the Department of Cardiology between January to December 2022. It is a prospective, comparative, randomized study. The Institutional Ethical Committee approved the study. Patients included in the study were with age >18 years and having EF by Simpson’s method <40% and estimated glomerular filtration rate (eGFR) by MDRD between >15 and <60 mL/min/1.73 m2. Patients with a heart rate (HR) >120 bpm on admission, serum potassium <3.5 mmol/L, pulmonary embolism, presence of clot in the left ventricle or right ventricle, hypertrophic cardiomyopathy, age >75 years, acute myocardial infarction of less than 14 days duration were excluded.
Sample size: The prevalence of ADHF is 11.6% in a study by Patricia et al. 5 Using this as the basis, the present study sample size was estimated using the formula below.
N = 1.96 × 1.96 × pq/L2 (absolute precision) [P: Prevalence, Q: 1-prevalence, L: Allowable error]
P = 11.6% = 0.116, Q = 0.884 (1 − p), L = 15% = 0.1
N = 1.96 × 1.96 × 0.116 × 0.884/0.1 × 0.1 = 0.3939/0.0225 =17.5 = 18
The minimum sample size required for the study was 18 for each group, and as the study progressed, 30 patients were enrolled in each group.
Methodology: The patients included were questioned regarding their sociodemographic details. Patients and attendees were questioned about their histories. On the day of admission, after the infusion was finished, and on days 7 and 30, all investigations were sent (complete hemogram, renal function tests, liver function tests, serum electrolytes, electrocardiograms, and an echocardiogram). The eGFR, according to the MDRD equation, EF, cardiac output (CO), and cardiac index (CI) were among the variables noted following the infusion, on the day of discharge/day 7, and at the one-month check-up. The additional factors evaluated were the change in symptoms, EF, and mortality at 30 days.
Data analysis: The gathered information was entered into a Microsoft Excel workbook and then exported to SPSS (Version 21.0 for Windows). The data has been presented in tables and diagrams with mean + SD and percentages. For the significance test, chi-square and non-parametric testing were used.
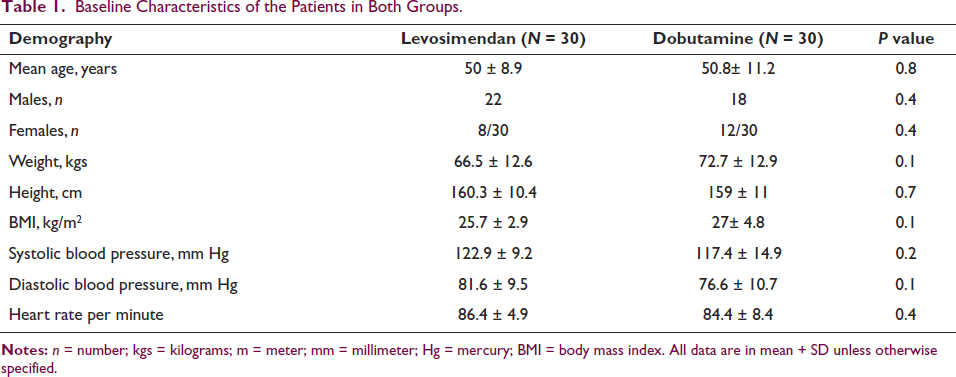
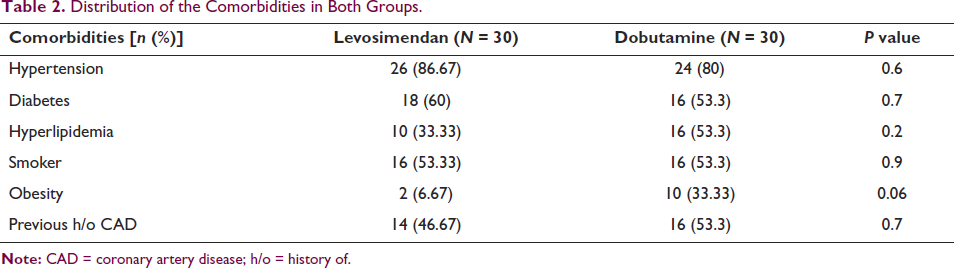
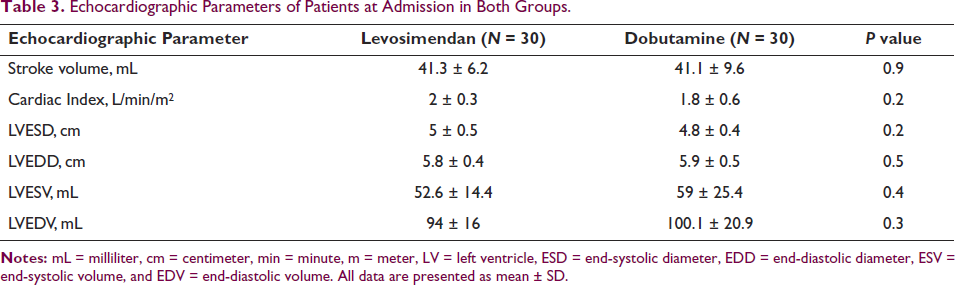
Results: Of the 60 patients, 40 were males and 20 were females (2:1 ratio). The mean age of both groups was (levosimendan, 50.8 ± 8.9 years vs. dobutamine, 50.8 ± 11.2 years, P = NS). The weight and body mass index of patients at admission were higher in the dobutamine group (66.5 ± 12.6 vs. 72.7 ± 12.9, P = 0.1) and (25.7 ±2.9 vs. 27 ± 4.8, P = 0.1), respectively. Clinically, the blood pressure and HR were higher in the levosimendan group than in the dobutamine group (Table 1). The common comorbidities were hypertension and diabetes in both groups (Table 2). The stroke volume, CI, left ventricle end-diastolic dimension, and volumes on echo at admission in both groups were (41.3 ± 6.2 mL vs. 41.1 ± 9.6 mL, P = 0.9), (2 ± 0.3 vs. 1.8 ±0.6, P = 0.2), (5.8 ± 0.4 vs. 5.9 ± 0.5, P = 0.5), (52.6 ± 14.4 vs. 59 ± 25.4, P = 0.4), and (94 ± 16 vs. 100.1 ± 20.9, P = 0.3), respectively (Table 3). At follow-up, the levosimendan group improved in serum creatinine, eGFR, CO, and CI compared to the dobutamine group (P < .05) (Table 4).
Discussion
This study in 60 patients with ADHF who had reduced EF and impaired renal function showed that levosimendan improved CO, CI, and eGFR during the hospital stay and at 30-day follow-up.
The American Heart Association and the American College of Cardiology Foundation say that people with low blood pressure and poor CO should get temporary intravenous inotropic support to keep their vital organs working, especially their kidneys (class IIb; level of evidence C). There has been a presumption that any inotropic medication that demonstrates a beneficial impact on blood circulation in the central and peripheral blood vessels will also enhance the functioning of the kidneys. This study has shown that levosimendan and dobutamine have distinct effects on the glomerular filtration rate (GFR). These findings are clinically significant and suggest that levosimendan may be the preferred inotropic drug for treating CRS.
Levosimendan acts by sensitizing calcium and opening KATP channels. It has a vasodilating, positive inotropic effect, enhancing gastrointestinal mucosal flow, creatinine clearance, and urine output while decreasing lactate. In renal failure, its effects and inotropic effects outperform dobutamine. 6
Dobutamine, conversely, appears to cause equal widening of both the arteries that carry blood to the kidneys (afferent arterioles) and the arteries that carry blood away from the kidneys (efferent arterioles). This leads to an increase in RBF while keeping the pressure for filtering blood in the kidneys (glomerular filtration pressure) unchanged. The observed pattern closely resembles the one previously reported for low-dose dopamine administration in patients who had heart surgery. In these individuals, dopamine caused a significant rise in RBF without affecting the GFR.
Experimental investigations suggest that levosimendan may positively impact the glomerular capillary ultrafiltration coefficient. Mesangial cells, which are found in the mesangium of the glomerulus and look like smooth muscle cells, control the surface area of the glomerular capillaries. They exhibit a response to vasoconstrictors, such as angiotensin II, by reducing the surface area accessible for filtration. levosimendan effectively reverses the contraction of mesangial cells induced by angiotensin. It is possible to hypothesize that the inhibition of angiotensin II-mediated contraction of mesangial cells and an increase in the surface area of glomerular capillaries are both contributing factors to the increase in GFR that levosimendan causes in HF patients, who typically have elevated levels of angiotensin II in their circulatory system.7, 8
The average age of the study population was like that of Khaled et al. (55.20 ± 8.59 years) but lower than that of John et al. (63.47 ± 12.23 years) and Lannemyr et al. (58.1 ± 11.6 years). The study found that there is a substantial proportion of patients with a history of coronary artery disease (CAD), and the average age of CAD patients in India is lower compared to other countries. This could explain why the average age in this study was lower than in most other studies.
The study comprised 20 females, 8 in one group and 12 in the other. The percentage of females in both groups is lower compared to similar studies such as the LIDO study (15 vs. 12) and the study of Yilmaz et al. (8 vs. 5), which were also fewer than 20% of the overall population. The incidence of ADHF is lower in females compared to males.
In their study, John et al. found that CAD accounted for 36.36% of cases, hypertension accounted for 36.36% of cases, and diabetes accounted for 68.18% of cases in the levosimendan group. The prevalence of diabetes in the dobutamine group was 66.67%, hypertension was 69.44%, and coronary heart disease was 25%. These features were like those in our study, except for hypertension.
Khaled et al. research showed that the levosimendan group had a much higher postoperative EF than the conventional group. Additionally, the levosimendan group had a significantly shorter hospital stay. Furthermore, the logistic EUROSCOREII exhibited a statistically significant increase in EF in the levosimendan group compared to the control group. 9
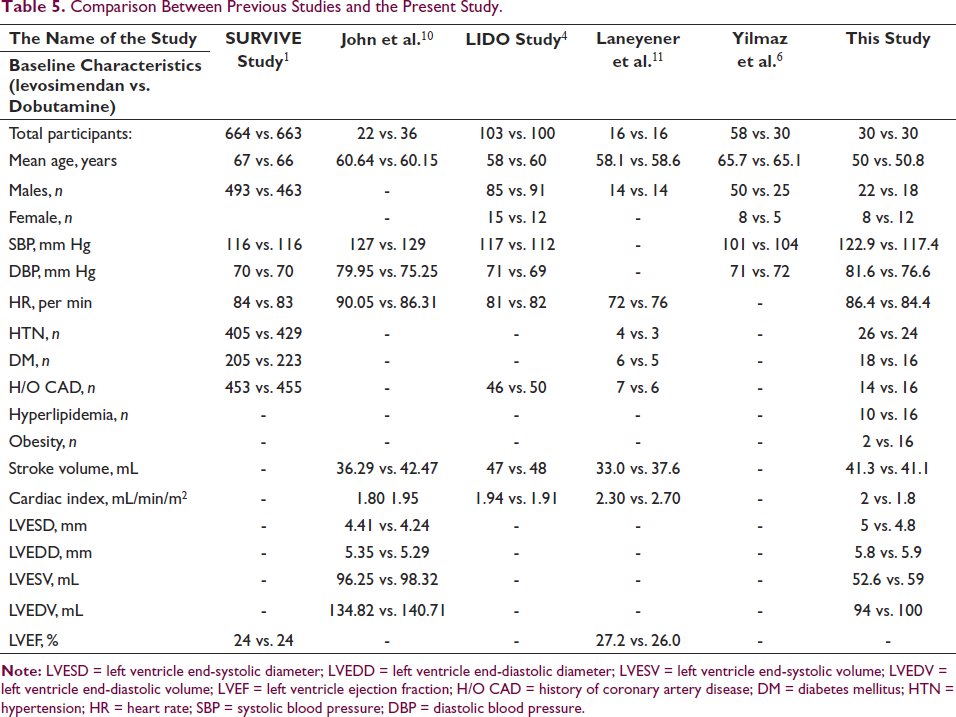
John et al. stated that levosimendan decreased HR from the initial measurement to 48 hours on the seventh day. The EF in the levosimendan group exhibited a substantial increase compared to the baseline measurements at 48 hours, 7 days, and 30 days. Although the HR dropped, the elevation in EF from the initial measurement to 48 hours in the dobutamine group was statistically significant but not in subsequent measurements. levosimendan demonstrated a substantial increase in EF at 48 hours, 7 days, and 30 days compared to dobutamine. 10 The comparison of previous studies with present study is shown in Table 5.
The levosimendan group consistently declined serum creatinine levels throughout the study period. However, a notable deviation from the initial measurement was observed only at the 30-day mark. In contrast, there was a considerable increase in eGFR from the initial measurement to 48 hours and only at 7 days. When compared to the baseline, the creatinine levels in the dobutamine group initially decreased and then increased until day 30. On the second and seventh days, there was a rise in eGFR compared to the first observations. levosimendan exhibited a significant reduction in creatinine levels at day 30, leading to an elevation in eGFR in contrast with dobutamine. On day 7, levosimendan decreased uric acid levels relative to the initial measurement, while dobutamine lowered uric acid levels on both day 7 and day 30. levosimendan was observed to reduce potassium levels at 48 hours and seven days. The injection of dobutamine resulted in a drop in potassium levels 48 hours later. levosimendan or dobutamine did not cause any significant changes in other parameters.
In animal tests, the vasodilator effects of levosimendan have been shown to keep mice from getting experimental endotoxemic acute renal failure. It has also been shown to turn on the ATP-sensitive potassium channel and nitric oxide synthase in mitochondria, which helps protect cells from damage caused by ischemia and reperfusion. 12 The pleiotropic activity of dobutamine is absent in this research, which helps to understand why uric acid and creatinine fall while eGFR increases.
The levosimendan and dobutamine groups both showed increased stroke volume index, CI, systemic oxygen delivery, and venous oxygen saturation (SvO2), according to the study by Lannemyr et al. 11 The filtrating fraction exhibited a 22% rise in the levosimendan group but remained stable in the dobutamine group. levosimendan did not have any impact on the filtering fraction. However, dobutamine resulted in a decrease of 17% in the filtering fraction. Both groups exhibited a decrease in renal oxygen extraction, with no differences.
In their study, Dharmendra Jain et al. 13 found that levosimendan (group 1) and dobutamine (group 2) substantially increased blood pressure and CI. However, patients in group 1 who received continuous administration of levosimendan saw a higher increase. In group 1, there was a significant rise in CO. However, in group 2, CO initially increased for the first 48 hours but declined on the fifth day. Stroke volume significantly increased in both groups; however, the rise was more prominent in the people treated with dobutamine in group 2.
According to Yilmaz et al.’s study, 6 it was evident that the left ventricular EF increased significantly for both groups. Following 24 hours, individuals in the levosimendan group saw a notable enhancement in their GFR. In contrast, those in the dobutamine group did not exhibit any significant changes in their GFR. Furthermore, the GFR in the levosimendan group exhibited a considerable improvement after 72 hours compared to the initial levels. However, no notable change was observed in the dobutamine group. Both medicines resulted in an enhancement of 24-hour urine production. levosimendan offers benefits over dobutamine in enhancing renal function for HF patients requiring inotropic therapy.
Baseline variables such as obesity, smoking, and hyperlipidemia were not included in significant earlier research that was conducted about HF risk factors. However, in this investigation, we have included similar characteristics. Certain studies solely examined renal indicators without assessing the hemodynamics of the heart. Both criteria have been incorporated into our investigations.
Limitations: The study’s small sample size may lead to false-positive findings or an overestimation of the strength of a relationship. Additionally, the single-center study’s small sample size and limited funding are weaknesses. A single center and a limited number of investigators will encounter challenges in recruiting and monitoring the required number of patients. Unblinding can introduce bias. An extensive follow-up period was necessary for this investigation to observe the effects on renal markers.
Conclusion
At 30 days in individuals with ADHF having reduced EF and impaired kidney function, the increase in CO caused by levosimendan not only raised RBF but also, unlike dobutamine, improved GFR, indicating a selective widening of the blood vessels supplying the kidneys. According to these data, levosimendan may be the preferred medication for treating individuals with CRS.
Baseline Characteristics of the Patients in Both Groups.
Distribution of the Comorbidities in Both Groups.
Echocardiographic Parameters of Patients at Admission in Both Groups.
Study Variables on Days 1, 7, and 30 in Both Groups.
Comparison Between Previous Studies and the Present Study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical Committee approval not needed for case reports in our institution.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Patient consent has been taken for the study.