
Abstract
The echocardiographic markers that occur in sequence in cardiac tamponade are inferior vena cava plethora, right atrial diastolic collapse, exaggerated inspiratory variation in mitral and tricuspid velocities and finally right ventricular diastolic collapse. Contrary to popular belief, the degree of atrial inversion does not correlate with the presence or absence of tamponade physiology, however, the right atrial inversion time (exceeding one-third of the cardiac cycle) significantly improves the sensitivity of atrial collapse in predicting tamponade. We present here an important demonstration of fundamental physiology of respirophasic variation of right atrial collapse in cardiac tamponade.
Case
A middle-aged patient with metastatic carcinoma breast presented with complaints of exertional dyspnea. On evaluation, the patient had tachycardia without any pulsus paradoxus or hypotension. The patient was mildly tachypnoeic at rest, with elevated jugular venous pressures, apparent cardiomegaly and muffled heart sounds. Respiratory system examination revealed no abnormality. An urgent trans-thoracic echocardiogram showed circumferential effusion measuring a maximum of 30 mm (Supplementary video 1). There were inferior caval vein plethora, exaggerated respiratory variations in mitral (>25%) and tricuspid (>40%) inflow velocities, right ventricular early diastolic collapse. M-mode interrogation of the right atrium in apical four-chamber view showed the diastolic collapse of the atrial free wall (Figure 1A), compared with normal: Figure 1B). The invagination of the atrial wall varied with the respiratory cycle, lasting longer during expiration. The patient was taken up for emergency pericardiocentesis, following which she improved symptomatically.
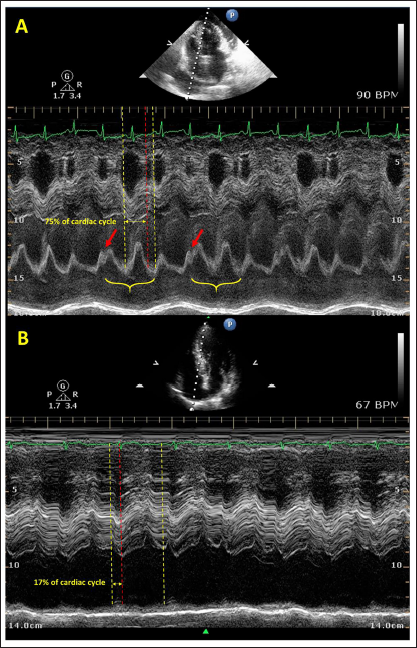
(A) M-mode 2D echocardiogram in apical 4-chamber view across a right atrial wall in a case of pericardial tamponade showing diastolic right atrial collapse (between yellow to red dotted lines) which extends up to more than one-third (75% in this case) of the cardiac cycle (between yellow dotted lines). Note that the collapse is exaggerated during expiration (brackets) when the intrathoracic pressure rises owing to the net intrathoracic volume shrinkage, causing a notch on the tracing (arrow). (B) A similar echocardiographic mode in a normal patient without pericardial tamponade showing right atrial collapse only during atrial systole, which is less than one-third (17% in this case) of the cardiac cycle which corresponds to the atrial systole duration in a normal cardiac cycle which is 0.1 second of 0.8 seconds (13%).
Discussion
The echocardiographic markers that occur in sequence in cardiac tamponade are inferior vena cava plethora, right atrial diastolic collapse, exaggerated inspiratory variation in mitral and tricuspid velocities and finally right ventricular diastolic collapse.
In the normal population, the rounded and concave configuration of the right atrial free wall is maintained during systole as well as diastole. In the presence of significant pericardial fluid, there is a diastolic buckling of the right atrial free wall. During diastole, the atrium empties into the ventricle causing a fall in pressure. The right atrial pressure and volume are lowest at end-diastole and intra-pericardial pressures are highest due to maximal ventricular distension. At this point, the intra-pericardial pressure exceeds right atrial pressures causing atrial collapse. Atrial collapse begins at end-diastole and continues into the ventricular systole for a variable period depending on intra-pericardial pressures. In contrast, ventricular collapse occurs in early diastole when the intra-ventricular pressures and volumes are lowest. Atrial collapse is more sensitive than ventricular collapse as the wall is thinner and more compliant. 1
The degree of atrial inversion does not correlate with the presence or absence of tamponade physiology, however, the right atrial inversion time (exceeding one-third of the cardiac cycle) significantly improves the sensitivity of atrial collapse in predicting tamponade. 2 The collapse duration varies with respiration, which is more prolonged during expiration. With expiration, there is a net increase in intrathoracic pressure as the thoracic cavity volume shrinks, which is transmitted to the pericardium leading to exaggerated atrial collapse. So, a transient inversion lasting less than one-third of the cardiac cycle without respirophasic variation may be non-specific. 3
Right atrial diastolic collapse is not dependent on the preservation of atrial contraction, as it was noted even in patients with atrial fibrillation or flutter. 2 The presence of atrial hypertension negatively impacts atrial collapse. The atrial collapse has also been documented in severe pectus excavatum or large pericardial effusion in the absence of tamponade due to extrinsic compression.4, 5 This case highlights the importance of atrial collapse duration and respiratory variation rather than depth of collapse in deciphering tamponade physiology in a case of large pericardial effusion.
Author Contribution
SSK (Conceptualization: Equal; Formal analysis: Lead; Writing – original draft: Lead; Writing – review & editing: Lead); SM (Conceptualization: Equal; Investigation: Equal; Supervision: Equal); SKG (Conceptualization: Equal; Formal analysis: Lead; Writing – review & editing: Lead).
Data Availability Statement
All data are incorporated into the article and its online supplementary material.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
Not applicable.
Supplemental material
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient consent for publication
Obtained.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.