
Abstract
Submitral left ventricular aneurysm is a rare entity. It is mostly in Africans; the most prevalent etiology is congenital. It is also seen rarely in Caucasians and Asians due to varied etiologies. The diagnosis may be achieved by transthoracic echocardiography, transesophageal echocardiography, or even left ventricular angiography. We present a case where the former was misleading and the latter could not be performed due to cardiac failure, yet diagnosis was achieved by magnetic resonance imaging.
Introduction
Submitral left ventricular aneurysm is a rare cardiac entity of unspecified etiology. This illness, which was initially discovered in Nigeria and other African countries, is more common among Black Africans. 1 Due to a deficiency in the posterior mitral annulus, it is typically thought to be congenital in origin. However, it can also be reported in other conditions including rheumatic and ischemic heart disease, infectious endocarditis, TB, and syphilis. 2 Patients may be completely asymptomatic and may exhibit ventricular wall rupture, heart failure, thromboembolism, mitral regurgitation, and/or left ventricular dysfunction, and also occasionally abrupt cardiac death. Surgery can prevent cardiac arrest if there is a strong suspicion and an early diagnosis. 3 We describe the challenges in preoperative evaluation and surgical management.
Case Report
A 65-year-old lady presented with progressive exertional dyspnea for the last 2 years and it progressed to a stage of NYHA class IV. She had pedal edema and mild dysphagia to solid foods. She had been investigated at various hospitals and the diagnosis was given as “severe mitral regurgitation with an additional septum/tumor in the left atrium leading to tethering of mitral valve and consequent reflux.”
On presentation, she had tachycardia with a blood pressure of about 100/60 mm Hg and had signs of cardiac failure evidenced by elevated jugular venous pressure, bilateral basal lung crepitations, and mild hepatomegaly. There was a pan systolic murmur in the precordium extending to the left axilla.
She was investigated extensively and the most recent transthoracic echocardiogram showed a mitral regurgitation with a septum or tumor that was tethering the valve, a trans-esophageal echocardiogram was also performed and it too showed a similar finding. A coronary angiogram was performed showing mild coronary artery disease and no distortion of the coronary vessels. Left ventricular angiogram was not done as the patient was in cardiac failure. We were not satisfied with the findings of the transthoracic echocardiogram and the rest of the investigations and hence magnetic resonance imaging was done to determine the cardiac morphology.
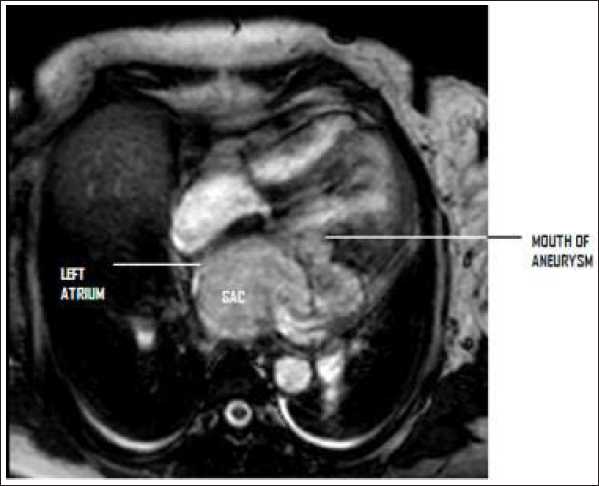
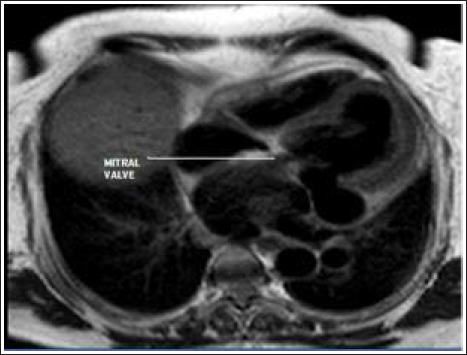
The cardiac MRI scan showed a defect in the left ventricle just below the posterior mitral leaflet (Figure 1 and 2). Although the mouth of the aneurysm was not large (i.e., less than 1 cm), huge sacs measuring 4.5 cm × 4.8 × 8.5 cm were seen behind the heart, and a large one compressing on the left atrium. The left atrium was compressed into a thin crescent-shaped cavity with diminutive volumes and the posterior wall of the left atrium was also in apposition with the posterior mitral leaflet. This may have led to the false impression of “a septum being adherent to the posterior mitral leaflet.”
The patient was first treated for cardiac failure and she also required anti-arrhythmic drugs as she occasionally had episodes of ventricular tachycardia.
Once she was stable, she was taken up for surgery. A median sternotomy was done and the patient was placed on a standard cardiopulmonary bypass. The aneurysm was initially approached through the left atrium. The mouth of the aneurysm could not be seen from there even after disconnecting the posterior mitral leaflet from the mitral annulus. Hence a left ventriculotomy was performed at the base parallel to the left anterior descending artery. This helped in revealing the mouth of the aneurysm about 6 mm × 10 mm in size. This was closed with a Gore-Tex Cardiovascular patch (W. L. Gore and Associates, Flagstaff, AZ) with interrupted pledget sutures and the aneurysm was excluded. The posterior mitral leaflet appeared thickened and tethered. Initially, repair of the Mitral valve was attempted, but, as the result was not satisfactory, the mitral valve was replaced with a mechanical prosthesis (27 mm St Jude mechanical bileaflet valve (SJM Master series, Abbott, Santa Clara, CA). The cardiotomies were repaired and the patient was weaned off the cardiopulmonary bypass. The postoperative period was uneventful. The aneurysmal sac was sent for histopathology and showed no specific etiology.
Discussion
In the black population of southern and western Africa, 4 Submitral left ventricular aneurysms are not unusual, and sporadic occurrences have also been reported in the white community. 5 Submitral aneurysms are rare and diverse disorders with an enigmatic etiology. Due to racial predisposition, genetic etiology has been proposed. 6 It is usually congenital in origin, but can also be secondary to diseases such as tuberculosis, rheumatic heart disease, and infective heart disease. 7
The basic pathology in these lesions has been described as a dysfunction between the left ventricle musculature and the left atrium-mitral valve region due to the disturbance of the complex embryogenesis that encloses the left atrium, left ventricle, and the mitral valve ensuring electrical isolation. 8
Nayak et al., 9 described submitral membranous dinas as the potential anatomical basis for this aneurysm. Beyond the Dosteromedial commissure, this membrane-which varies in length throughout the posterior annulus-forms a possible weak point. The posterior mitral annulus can have an aneurysm that affects anywhere from a tiny spot to the entire region.
Patients may present with mitral insufficiency, cardiac failure, arrhythmias, and myocardial ischemia due to compression of the coronary artery. The mitral apparatus may get distorted as the aneurysm grows in size. The surgical plan and execution will depend on the direction of the growth of the aneurysm.
Echocardiography forms the first line of investigation and is considered the gold standard. The questions that need to be answered regarding the aneurysm are exact location, spatial relationship, potential involvement of the mitral apparatus, morphological features, and assessment of mitral regurgitation. Misdiagnosis or doubt of submitral aneurysm by transthoracic echocardiogram is seen even in experienced centers. It may be subject to observer errors as shown in the above paper. Left ventricular angiography can also clinch the diagnosis, however, it is an invasive test and does give a “contrast load” to the heart and may not be safe in some patients who are in failure or who have a chance of having free clots in the aneurysm. A left ventricular angiogram may precipitate arrhythmias and already these patients are prone to ventricular arrhythmias (many of the reported mortalities are due to the onset of arrhythmias).
Magnetic resonance imagery has shown to be of great help in making the diagnosis in this case.10, 11 It has emerged as the preferred non-invasive modality for the assessment of all the anatomical and morphological features of a submitral aneurysm. 9 The clinico-imageological correlation was good as seen in the operation theatre after cardiotomy. As the investigational modality is non-invasive, it is safe and can be performed easily. The images help the surgeon in identifying the morphology correctly and also in planning the operation.10, 11 The MRI’s drawbacks include its non-portability length and unavailability. It also scans slowly.12–14
The main surgical challenge for us was the approach as atriotomy was not giving adequate visibility and access. A left ventriculotomy was necessary for a complete assessment of the Submitral aneurysm to plan the repair and subsequent mitral valve replacement.
Conclusion
In conclusion, in such rare cases, a successful outcome depends on proper diagnosis, careful handling of the heart, planning of the approach to the aneurysm, and avoiding injury to the coronary vessel.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical permission was not applicable, as this work was a case report, not a research study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Patient consent for the publication and sharing of radiologic investigation figures was obtained.