
Abstract
Lutembacher’s syndrome is a rare condition and is most often treated surgically. Due to the advances in percutaneous procedures, this form of management is desired which has the advantage of decreased morbidity and is aesthetically superior. In this case report of percutaneous treatment for a Lutembacher’s patient the percutaneous transvenous mitral commissurotomy and atrial septal defect device closure was done with minimal technical difficulties and with excellent post-procedure results.
Keywords
Introduction
Lutembacher’s syndrome (LS) is a very rare condition and is characterized by a congenital ostium secundum type atrial septal defect (OS-ASD) and an acquired mitral stenosis (MS) which is commonly rheumatic in origin.1, 2
Traditionally the treatment preferred for patients with LS was surgical ASD closure and open mitral commissurotomy or valve replacement.3, 4
However, percutaneous management is always desirable, especially in females in whom LS is more common.5–8
This is a case report of a 23-year-old female suffering from LS who underwent successful percutaneous treatment.
Case Report
A 23-year-old married female presented with a chief complaint of dyspnoea on exertion for the last 4 years.
On examination patient had a parasternal heave and a wide fixed split S2, with a loud P2. A low-pitch, grade 3/4, mid-diastolic murmur was heard in the mitral area. A grade 3/6 ejection systolic murmur was heard in the left second parasternal area.
The electrocardiogram showed normal sinus rhythm with a heart rate of 62 bpm and incomplete right bundle branch block with right axis deviation.
Chest X-ray showed pulmonary plethora with straightening of left heart border.
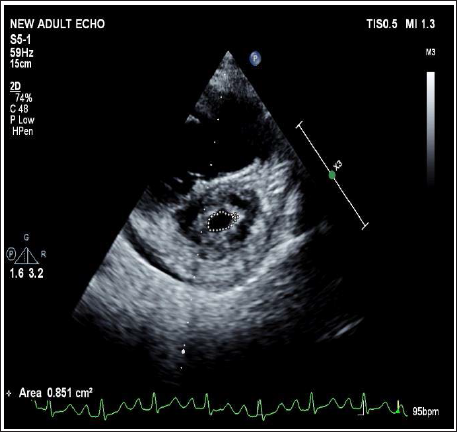
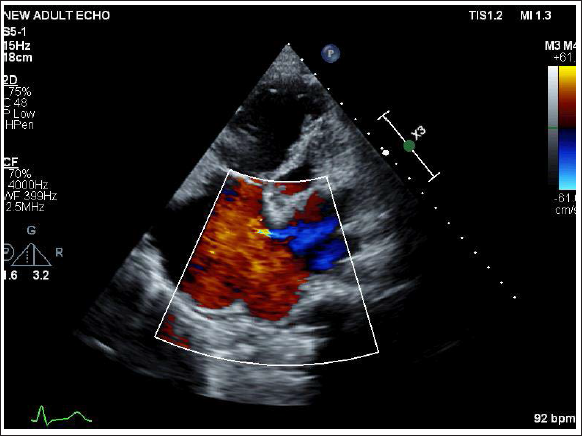
Transthoracic echocardiography was done which showed a large ostium secundum ASD and severe rheumatic MS. The mitral valve orifice area was 0.8 cm2 by planimetry with a mean mitral valve gradient of 12 mm Hg. The mitral valve leaflets were noncalcified. The Wilkins score was 6. There was no mitral regurgitation. Color flow Doppler revealed a left-to-right shunt across the ASD (Figures 1 & 2).
Pre Procedure Transthoracic Echocardiography Showing SAX View at Mitral Valve Level with Mitral Valve Area (MVA) of 0.8 cm2.
Pre Procedure Transthoracic Echocardiography Showing Large ASD with Color Flow Doppler Showing Left to Right Shunting and Grossly Dilated RA/RV.
Transesophageal echocardiography (TEE) was done which showed 19 mm OS-ASD. There was mild tricuspid regurgitation (TR) with a pulmonary artery systolic pressure (PASP) of 42 mm Hg. On cardiac catheterization, the pulmonary artery pressure was 40/23(30) mm Hg, with a mean of 30 mm Hg, and the mean left atrium (LA) pressure was 20 mm Hg.
The ASD and MS were amenable to percutaneous treatment, hence both the transcatheter therapy was performed in a single setting.
Technique
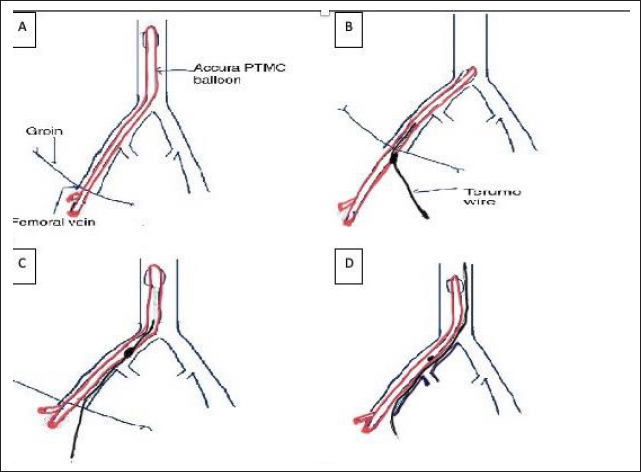
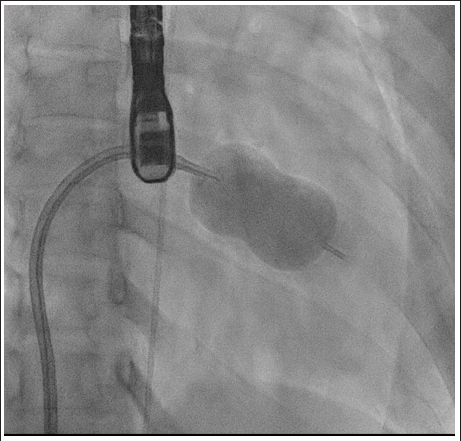
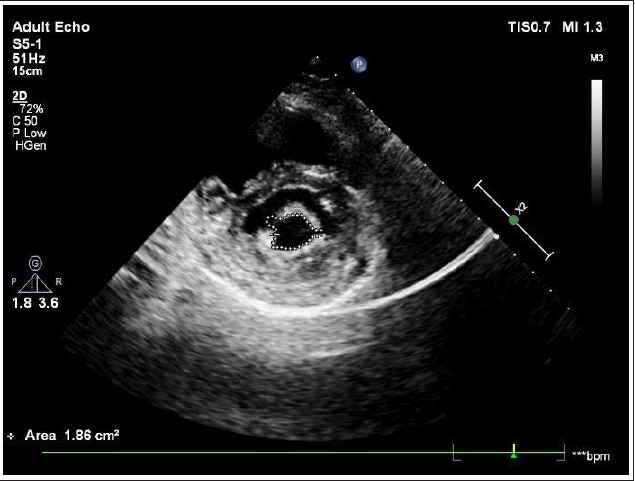
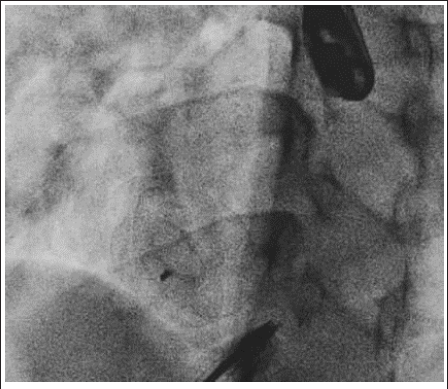
Balloon mitral valvotomy (BMV) was performed first. The atrial septum was crossed with Mullins sheath across ASD. LA wire was placed into the LA then the PTMC balloon was guided over the LA wire. LA wire was removed and an Accura 28 mm PTMC balloon was attempted to cross the mitral valve, however, the new style that came with the balloon damaged the balloon and its lumen. We were unable to get a wire across the lumen to remove the balloon. In order to maintain access we then made a small opening in the balloon shaft and inserted a Terumo wire and passed it together till the common iliac. Under fluoroscopy, the wire was then pulled slightly back and passed into the lumen of the vessel till SVC, and the balloon was taken out to maintain access (Figure 3). We then used another balloon with a different stylet and crossed across the mitral valve into the LV. The MV was dilated successfully with a 28 mm Accura balloon (Figure 4). Post BMV transmitral gradient reduced to 2 mm Hg and achieved an MVA of 1.86 cm2 with no significant MR (Figure 5).
Schematic Diagram Showing the Method Used to Maintain Venous Access After the Accura Percutaneous Transvenous Mitral Commissurotomy (PTMC) Balloon and Lumen Got Damaged. Part (A) Showing Damaged PTMC Balloon in Femoral Vein. (B) PTMC balloon was Withdrawn and a Small Opening was Made in the Balloon Shaft to Pass the Terumo Wire. (C) PTMC Balloon with the Terumo Wire was Passed Together Till the Common Iliac. (D) The Terumo Wire Under Fluoroscopy was then Pulled Slightly Back and Passed into the Lumen of the Vessel Till Superior Vena Cava (SVC) and the Balloon was Taken Out to Maintain Access.
Fluoroscopy Image Showing Well Inflated 28 mm Accura Balloon During PTMC.
After successfully performing BMV, the ASD device closure was undertaken. A 21 mm ASD device was placed across the atrial septal defect under TEE guidance (Figure 6).
Fluoroscopy Image Showing Well Deployed 21 mm Figulla Flex ASD Device (Occlutech).
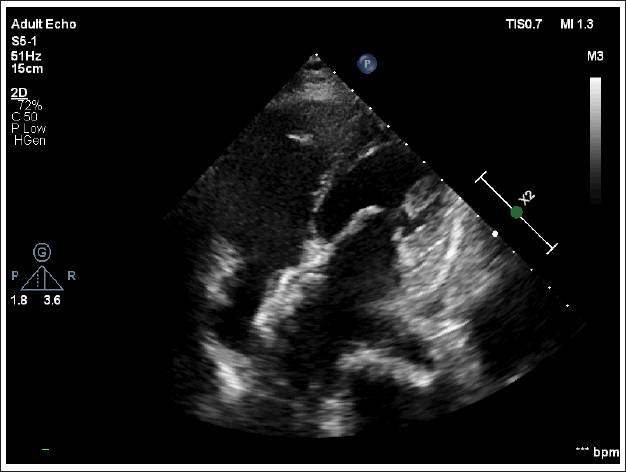
Post-procedure a transthoracic 2D echocardiography (ECHO) was performed which showed a well-deployed ASD device in situ (Figure 7).
Post-procedure Transthoracic Echocardiography A4C Showing ASD Device In Situ with Wide Open Mitral Valve.
Discussion
Since the time when LS was first described by Rene Lutembacher in 1916, there have been great advancements in understanding the pathophysiology, diagnosis, and management of LS. 1
The effect of ASD on MS causes the delayed appearance of high pulmonary venous pressure, and hence symptoms like dyspnoea, hemoptysis, and early increase of pulmonary arteriolar resistance. While the MS maintains the pressure gradients across the atria promoting left-to-right shunting till the late stages. 9
The one hemodynamic complication of MS which is aggravated by atrial septal defect is low systemic output which improves after the appearance of PAH which decreases the left to right shunting. 9
With improving and evolving percutaneous techniques the management of LS in properly selected patients can be successfully managed percutaneously rather than surgically with good results and lesser morbidity and complications. The merits of this mode of treatment are being effective and safe in selected patients and prevention of major cardiac surgery and anesthesia complications. It also prevents sternotomy with skin scars and reduces hospital stay.
The current indications for percutaneous transcatheter treatment are a large hemodynamically significant ASD with a Qp to Qs ratio of >1.5, with good rims, moderate to severe symptomatic MS with favorable valve morphology for BMV, and pulmonary hypertension of any degree.
A systematic review of the literature showed that to date 25 cases of percutaneous intervention for Lutembacher’s have been published in world literature.8, 10, 11 Due to the presence of ASD there is a lack of support for the PTMC balloon and hence crossing the mitral valve can be challenging. Various techniques are then required eg. OTW technique, balloon flotation, catheter sliding technique, etc.4, 11 In our case we did not have much difficulty in crossing the mitral valve.
In some cases, ASD device closure was done three to four days after PTMC to be sure of the result of PTMC as repeating PTMC after the device is difficult. In the present case complication of the stylet damaging the balloon was successfully managed while maintaining wire access which is an important learning point. The result of PTMC was good hence ASD closure was done in the same sitting.
Take home message: LS is a condition where with proper patient selection and planning both lesions can be treated with percutaneous therapy and in one setting.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not Applicable.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
The consent was obtained from the patient to be involved in this study.