
Abstract
We present a case of bigeminal rhythm where a critical evaluation of underlying rhythm abnormality is important to differentiate escape-capture bigeminy from escape-echo bigeminy, and to decide further management plans.
Case
An octogenarian patient presented with one presyncope episode and was diagnosed with symptomatic sick sinus syndrome and referred for permanent pacemaker implantation. Clinical examination, routine blood investigations including electrolytes, and echocardiographic evaluation were within normal limits. A 12-lead electrocardiogram has been shown in Figure 1A. What is the likely mechanism?
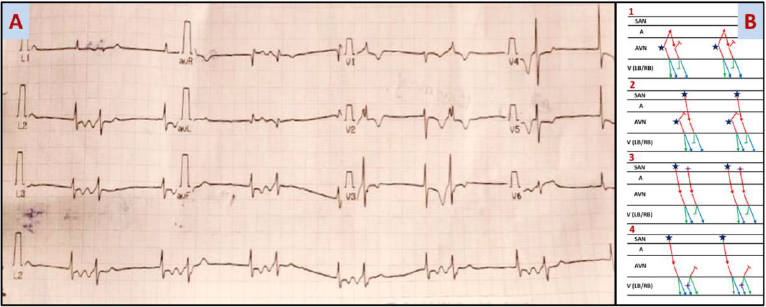
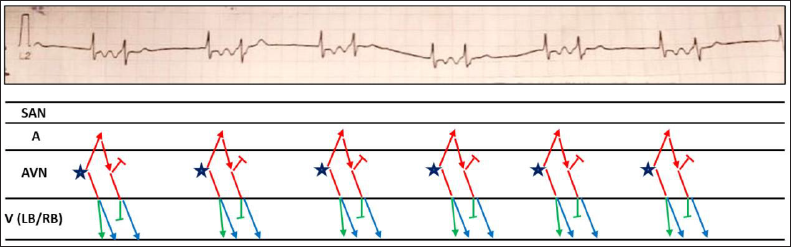
The 12-lead electrocardiogram shows a junctional escape-echo bigeminy with the Ashman phenomenon (Figure 1A and 1B1). 1 The first beat is not preceded by any P wave suggesting a sinus node dysfunction with a narrow escape rhythm (likely junctional ectopic having forward activation of ventricles via left and right bundle branches, and retrograde activation of the atria). Following the junctional ectopic, retrograde P waves are best seen in the inferior leads as a negative deflection on T waves. This P wave is conducted aberrantly with a right bundle branch block pattern (Figure 1B1, 2). The right bundle has a property of faster conduction velocity with a longer refractory period causing it to be prone to conduction block in the presence of a preceding shorter cycle length. It is documented in atrial fibrillation patients that a conducted QRS has a right bundle branch block immediately after a shorter cycle length and it recovers after a longer cycle. This is known as the Ashman phenomenon. 2 The term junctional escape capture bigeminy means a bigeminal rhythm where a nodal junctional escape beat is followed by a sinus beat conducted to the ventricle either with or without aberrancy (Figure 1B2). 1 Hence, a sinus P wave resides in between two QRS complexes (a retrograde P wave instead of sinus P in case of escape-echo bigeminy).
Figures 1B3 and 1B4 represent atrial and ventricular bigeminy, respectively. The patient underwent an AAI permanent pacemaker and is asymptomatic at present.
Author Contribution
SM: Conceptualization - Equal; Formal analysis - Lead; Writing—original draft - Lead; Writing—review & editing - Lead.
DB: Conceptualization - Equal; Investigation - Equal; Supervision - Equal.
Data Availability Statement
The data underlying this article are available in the article and in its online supplementary material.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Obtained.