
Abstract
Pacemaker bigeminy is not an uncommon electrocardiographic finding in device clinics. However, such a pattern mandates the differentiation of important possible diagnostic considerations such as premature atrial contractions, oversensing the T wave or the QRS complex, dual AV nodal physiology, and retrograde atrial depolarization. We present a case of pacemaker bigeminy where ventricular pacing was used to exclude the truncated form of pacemaker-mediated tachycardia and reach a diagnosis of atrial bigeminy, which was crucial from the management’s perspective.
Case
A sexagenarian man with a complete heart block had undergone implantation of a dual-chamber DDD pacemaker (Biotronik, Berlin, Germany) in the past. He presented with the electrocardiogram on follow-up, with the rhythm shown in Figure 1. Ventricular and atrial lead parameters (threshold and impedance) were within normal limits. Sensed AV delay, paced AV delay, and post-ventricular atrial refractory periods were 135, 180, and 225 ms, respectively. Ventricular threshold testing showed no retrograde conduction during pacing at 70/min.
What is the likely mechanism for the bigeminy?
T wave oversensing Truncated pacemaker-mediated tachycardia (PMT) R wave oversensing Atrial bigeminy
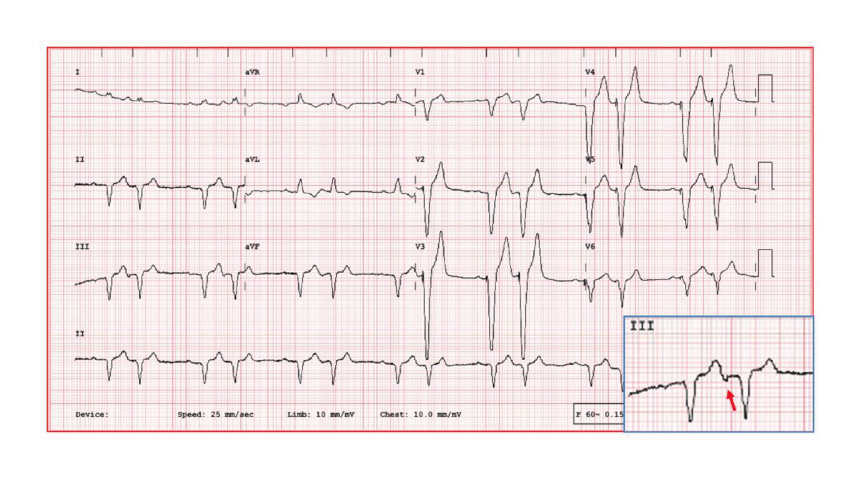
12-lead Electrocardiogram Showing Ventricular Depolarizations in a Bigeminal Pattern, All of Which Are Preceded by a Pacing Stimulus. In Addition, the First Beat in Each Pair Is Followed by an Atrial Depolarization (Arrow in Inset: Lead III), Which Appears to Be Retrograde Atrial Activation from the Ventricular-paced Beat.
Discussion
The electrocardiogram revealed pacemaker bigeminy (Figure 1). A search for the preceding atrial event for the second complex in the bigeminy revealed a negative deflection after the T wave in lead III. This negative wave was possibly a retrograde P wave following ventricular activation or an intrinsic atrial ectopic (Figure 2(a)). Differential diagnoses of such bigeminy have been attributed to various causes such as premature atrial contractions, oversensing the T wave or the QRS complex, dual AV nodal physiology, and retrograde atrial depolarization.1, 2 T wave oversensing was ruled out as there was no continuation of further ventricular events following the second T wave in the bigeminy complex. R wave oversensing was also not possible because the R wave to the next R was 400 ms, which was far more than the set sensed AV delay of 135 ms (Figure 2(b)). Usually, a long AV delay permits the AV node to recover and promote retrograde conduction, a recognized etiology for PMT. However, our patient had a shorter AV delay. The absence of a P wave was noted following the second complex, suggesting either a second-degree 2:1 VA block leading to a truncated form of PMT or atrial bigeminy (Figure 1). Previous studies have shown that up to one-third of CHB patients might have intact VA conduction. 3 However, ventricular pacing during threshold testing revealed no retrograde conduction via the AV node, ruling out the possibility of truncated PMT. A subtle change in the QRS morphology of the two complexes in bigeminy had been attributed to rate-related depolarization abnormality. In summary, although short AV delay and the absence of second retrograde P indicate atrial bigeminy, truncated PMT with retrograde 2:1 VA block cannot be ruled out with certainty, often requiring baseline VA conduction evaluation by ventricular pacing.
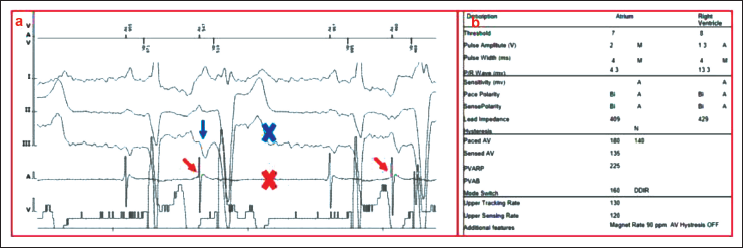
(a) Intracardiac Electrocardiogram. (Note That the First Beat in Each Pair Is Followed by an Atrial Depolarization [Negative P in Lead III: Blue Arrow, Spike on Atrial EGM: Red Arrow] and the Second Beat Is Not Followed by Any Atrial Depolarization [Cross Mark on ECG and EGM]). (b) Lead Parameters.ECG, electrocardiogram; EGM, intracardiac electrocardiogram.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Obtained from the patient in line with COPE guidance.
Authors’ Contribution
SM (Conceptualization: Lead; Formal analysis: Lead; Writing—original draft: Lead; Writing—review & editing: Lead); DPR (Writing—review & editing: Equal); JV (Writing—review & editing: Equal)