
Abstract
“Coronary cascades” or “coronary arcades” are congenital inter-coronary communications allowing uni- or bi-directional blood flow seen in the absence of obstructive coronary lesions. Coronary cascades take up the role of collaterals if atherosclerotic lesions develop. We present the angiogram images of a coronary cascade connecting left anterior and right posterior descending arteries (LAD and RPDA) in the distal interventricular groove in a patient with spontaneous coronary artery dissection and near total occlusion of LAD who presented with inferior wall myocardial infarction secondary to acute thrombotic occlusion of the right coronary artery. The presence of the arcade prevented a massive inferior or anterior wall myocardial infarction in our patient.
Case Description
A middle-aged hypertensive gentleman presented to an outside centre with acute inferior wall myocardial infarction (IWMI) 18 months back. Coronary angiogram (CAG) showed mid-right coronary artery (RCA) thrombotic occlusion and spontaneous coronary artery dissection (SCAD) of the proximal to mid-left anterior descending (LAD) artery. Following a failed attempt of thrombus aspiration, the patient was managed medically with anticoagulation. He had developed angina on exertion since last 2 weeks and had come to our centre for further management.
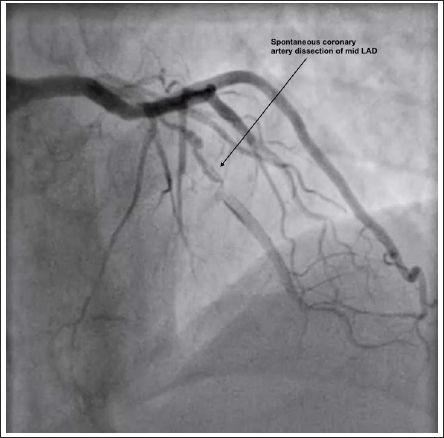
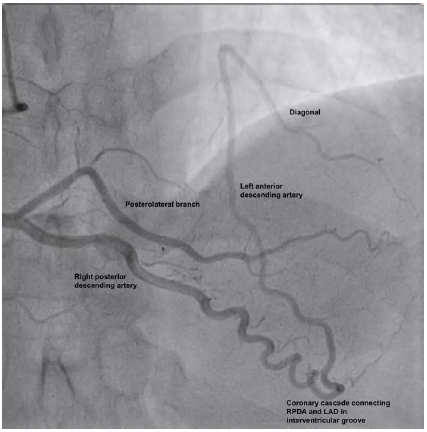
The patient was taken up for revascularization. The proximal to mid-LAD SCAD showed near total occlusion with preserved antegrade blood flow (Figure 1 and Supplementary Figure S1). Right coronary injection showed a recanalized RCA with posterior descending artery (PDA) wrapping around the apex and continuing as LAD (Figure 2). Collaterals are generally smaller in calibre compared to the donor or recipient vessel. Here, the vessel was the same size as the donor and recipient and appeared to serve as a direct continuity between the two vessels, likely indicating that it was a coronary cascade or an inter-arterial communication rather than a coronary collateral.
Left Coronary Injection Shows a Spontaneous Coronary Artery Dissection in Mid-LAD with Preserved Antegrade Blood Flow.
Right Coronary Injection Shows a Coronary Cascade Connecting the Right Posterior and Left Anterior Descending Arteries in the Interventricular Groove.
Discussion
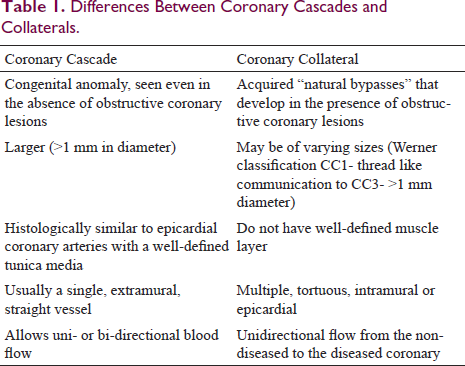
Coronary collaterals and coronary cascades are the two described forms of communication between the coronary arteries. While coronary collaterals are considered “natural bypasses” that develop in the presence of obstructive coronary lesions to provide an alternative blood supply to myocardial territories supplied by stenosed vessels, inter-coronary communications, also known as coronary cascade or coronary arcade is a congenital anomaly due to the persistence of fetal pattern of coronary circulation. It is a rare coronary anomaly with a reported incidence of 0.002%. 1 Coronary cascades are much larger (more than 1 mm), single, and have a straight extramural course compared to coronary collaterals, which are smaller and multiple, with tortuous epicardial or intramural course (Table 1). Coronary cascades have well-defined tunica media like normal epicardial coronaries and allow a bidirectional blood flow. However, unidirectional blood flow has also been documented. 2 Coronary cascades are usually described as connecting LCX and RCA in the posterior atrioventricular groove and LAD and RPDA in the distal interventricular groove, as in our patient. Other communications between the ramus and left anterior descending artery, PDA, and diagonal have also been rarely reported. 3
Differences Between Coronary Cascades and Collaterals.
Coronary cascades take up the role of collaterals if the patient develops significant atherosclerotic lesions. In our patient with near total occlusion of LAD, the coronary cascade ensured blood supply to the LAD territory from the right coronary system, thus preventing infarction. When the patient developed IWMI with thrombotic occlusion of RCA, it allowed perfusion of RCA territory from the left coronary system. In non-diseased coronaries, unidirectional blood flow via these connections might lead to coronary steal and myocardial ischemia. Most reported cases of coronary cascades showed that angina was a common complaint. It is important to recognize these anomalies during coronary angiograms as symptomatic patients with a normal coronary system, apart from these coronary connections, do not need any intervention and only reassurance. Due to their anatomic location, they may come up in the future as alternative retrograde access to stenosed vessels during difficult percutaneous coronary interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical committee approval is not required according to guidelines as this case report is anonymous.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors confirm that the consent for submission and publication of this case report has been obtained from the patient in line with the Committee on Publication Ethics Guidance.
Supplemental material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.