
Abstract
Introduction
The aortopulmonary window (APW) is a rare congenital cardiac anomaly in which there is incomplete separation of the pulmonary artery and aorta. Percutaneous transcatheter closure is possible in a specific subset of APWs only, and surgery remains the mainstay of therapy.
Clinical summary
We report a rare case of percutaneous device closure of post-device residual APW in a 32-month-old baby who had residual shunt post the device closure at two months of age.
Discussion
Transcatheter closure of an aortopulmonary window is an effective and safe procedure for specific anatomic defects.
Introduction
The aortopulmonary window (APW) is a congenital defect resulting from incomplete separation of the walls of the pulmonary artery and aorta at the conotruncal septum. It accounts for 0.2% to 0.6% of all congenital heart diseases. 1 Surgery is the first line of treatment; however, percutaneous device closure is also suitable in a specific subset of APW. Several case reports describe the transcatheter closure of APWs with different devices. 2 Residual defects are a known complication of patch closure of these defects, but rarely have residual defects been reported post the device occlusion. We report here the percutaneous transcatheter closure of a residual (post-device) APW.
Case Report
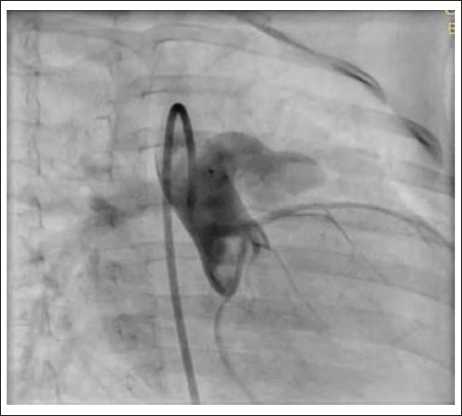
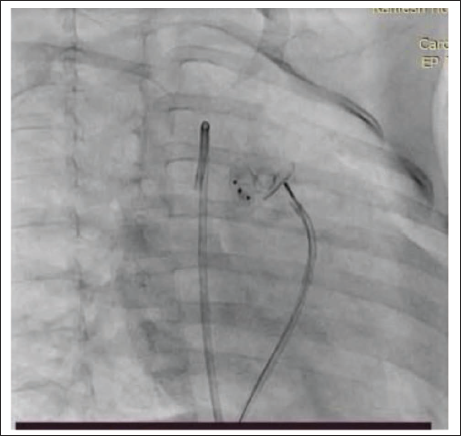
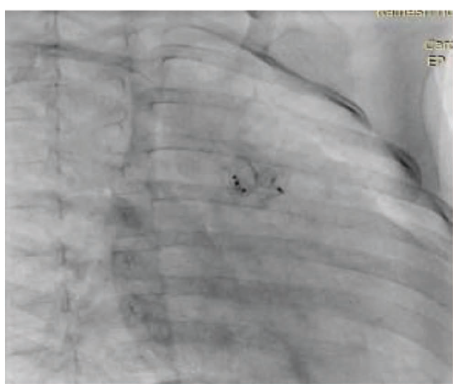
A two-month-old male baby was admitted with a history of failure to thrive and tachypnea. On evaluation, the child had features of congestive heart failure and weight of 3.5 kg. The chest X-ray showed cardiomegaly with plethoric lung fields. Echocardiography showed a 4.5 mm proximal APW with a dilated left heart and severe hyperkinetic pulmonary arterial hypertension (RVSP: 50 mm Hg). The baby was scheduled for device closure. Right femoral arterial and venous access were obtained, and an angiogram was taken to profile the APW. A 0.038 Terumo wire was passed from the retrograde route and snared through the femoral vein, making an aorta-venous loop. 6 X4 Amplatzer Duct Occluder-II (ADO-II) was deployed from the aortic side (retrograde) with a 5F JR guide (Figure 1). There was a small residual shunt with a left-to-right shunt post the device deployment. There was no supravalvular obstruction of the great arteries or coronary obstruction. The baby was started on aspirin and discharged on the third day of the procedure. On follow-up, the baby was gaining weight, and symptoms subsided. At the age of 2 years and 8 months on follow-up, the baby was found to be tachypneic with a 4 mm residual aortopulmonary window, a dilated left heart, and mild pulmonary arterial hypertension (mean PA pressure: 25 mm Hg). In view of the significant shunt, it was decided to close the residual shunt with the device. After obtaining consent, the baby was scheduled for AP window device closure. 5F right femoral arterial and venous access were obtained. The aortogram showed a 4 mm residual shunt (Figure 2), the defect was crossed from the venous side, and 6 × 6 ADO-II was deployed by 5F JR anterogradely (Figure 3). There was no residual shunt and no supravalvular great arterial obstruction, and both devices were sitting in harmony (Figure 4). The baby was discharged on antiplatelet, is gaining weight, and is asymptomatic on follow-up.
ADO-II 6 × 4 Deployed Successfully Through the Retrograde.

Angiogram Depicting a Significant Residual Shunt Above the Device.
Deployment of the Second Device ADO-II 6 × 6 through the.
Both Devices Sitting in Harmony.
Discussion
APW is classified into three types: type I (proximal defect) is midway between the semilunar valves and pulmonary bifurcation; type II (distal defect) is with the posterior border absent and the aortic origin of the right pulmonary artery; and type III (total defect) includes the defects present in both types I and II. Device closure is often possible in Type 1 APW. 3 Surgery is the mainstay of therapy, as excellent outcomes are achieved with it, and transcatheter closure is technically difficult. Despite the advances made in the development of devices for the closure of various congenital heart diseases, transcatheter APW is still in its early stages. This approach also has several advantages, such as the avoidance of extracorporeal circulation during the procedure and shorter postoperative and hospital stays. 4 The importance of appropriately characterizing the defect through several angiographic views or measurement balloons cannot be underestimated. It has been a challenge to choose the appropriate device, and in fact, there is no consensus on the choice of an optimal device for closure. Different devices, including septal occluders, muscular VSD devices, perimembranous VSD devices, duct occluders (ADO-I, ADO-II, and ADO-II AS), and vascular plugs, have been used with good results. Each has its own advantages and disadvantages. Septal occluders are bulky and carry with them the risk of injury or obstruction to semilunar valves or coronary origins. Perimembranous VSD devices have a flat profile; changes of instruction are reduced, and since these have asymmetrical disks, they can be used to close APW with a relative deficiency of one of the borders. ADO-I can protrude into MPA and cause obstruction. In our case, we have used ADO-II at both times for the occlusion of the defect owing to its low profile, the requirement of a smaller-sized delivery system (which can be deployed easily by the 4F or 5F JR guide), and lesser vascular complications. The device is made of nitinol, which is self-expanding, has greater flexibility and a low profile as it is produced by fiber-free technology, and is made in such a way that each disk assumes its own independent orientation, which significantly reduces the risk of protrusion and anatomical distortion. 5 On the other hand, its double-disk design may cause turbulence in the pulmonary artery. Our closure of residual post-device APW with a second device is the second case reported in the literature, which shows the uniqueness of the method. Only one such case has been reported by Quintero et al. from Mexico, in which they used ADO-II 6 × 4 at the first instance at one month of age to occlude the APW, and later, after one year, the residual was occluded by ADO-II 4 × 4. 4
Conclusion
APW is a rare congenital heart disease for which surgery is the mainstay of treatment. Percutaneous device closure is feasible in specific anatomical subsets. Our case adds on to the rare experience of post-device residual occlusion with the second device of APW.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.