
Abstract
Ginkgo biloba leaf extract is a common herbal supplement globally. It became popular in recent times, due to its stated benefits of improving memory. We report a case of a 66-year-old female having rhythm abnormality secondary to this supplement. She had no cardiac ailment, and the rhythm abnormality resolved on the withdrawal. Every arrhythmia evaluation checklist should include the use of Ginkgo biloba and other supplements.
Keywords
Introduction
Cardiac arrhythmias are disorders of the heart rhythm―which can be at a low rate (heart rate <50 beats per min (bpm), bradyarrhythmia) or a high rate (>100 bpm, tachyarrhythmia). They can be asymptomatic, being detected incidentally on examination. When symptomatic―they can cause widely varied symptoms―palpitations, dyspnea, fatigue, dizziness, and syncope. Severely symptomatic arrhythmias, when not intervened, can lead to cardiac arrest or sudden death. The etiology of the arrhythmias comprises mainly, structural abnormality in the heart (myocardial infarction), abnormal conduction (accessory pathways), or abnormality of the ion channels. Some complementary herbal medicines or over-the-counter drugs can have cardiac arrhythmic side effects.
Ginkgo biloba is used as a dietary supplement (mainly leaf extract), despite no scientific evidence that it has a beneficial effect on improving health, cognition impairment, intermittent claudication, and vertigo.1, 2 We present a case of a 66-year-old female presented with palpitations secondary to the use of Ginkgo biloba. The bradyarrhythmia improved after discontinuation of the drug. The pharmacokinetics, its effect on the heart, and a literature review are presented.
Case
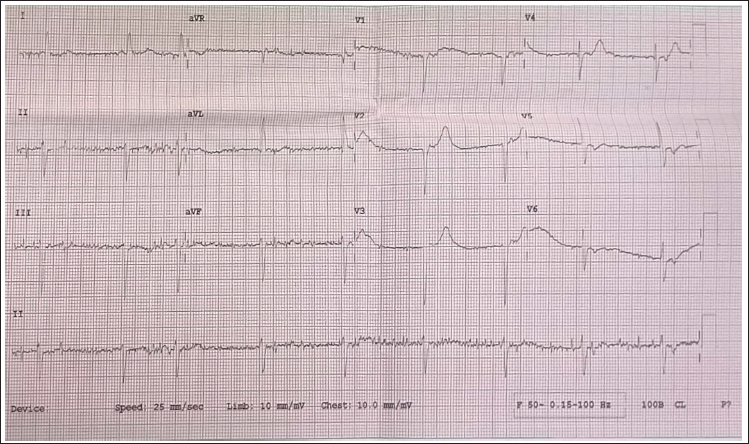
A 66-year-old female presented to the cardiology department with dizziness and palpitations. On examination, her heart rate was 52 bpm; and her blood pressure was 130/80 mm Hg. Heart and lungs were normal on auscultation. An electrocardiography was taken which showed junctional rhythm with a rate of 52 bpm. There were P waves after every QRS complex (? retrograde) (Figure 1). The Chest X-ray and 2D echocardiography were normal. The thyroid profile was normal. Routine blood investigations, and serum electrolytes, including serum calcium and magnesium were within normal limits. On further evaluation of the past history, it was revealed that she had been diagnosed with frontotemporal dementia a few months prior to the presentation. She did not have any signs of autonomic dysfunction.
Electrocardiogram at Admission Showing a Heart Rate of 52 bpm, No P Waves Seen Before Each QRS Complex, Junctional Rhythm. Baseline Artifacts Are Seen in the Limb Leads.
The consulting neurologist prescribed Tab. Rivastigmine, Tab. Memantine, Tab. Citalopram, and Tab. Ginkgo 60 mg twice daily and she has been using them since then. Holter monitoring for 48 h was done subsequently. The average heart rate was 65 bpm (minimum 37 bpm and maximum 94 bpm).
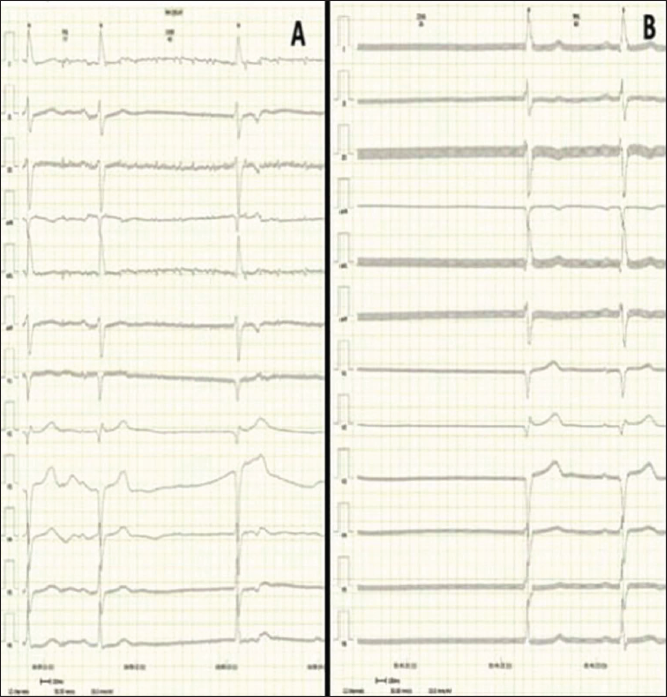
There were no supraventricular beats. Ventricular beats were 686. Of the 1052 delays, the longest was 1.98 sec. A total of 512 pauses (>2.0 sec) were recorded (Figure 2).
Holter Electrocardiography Showing (A) N-N Delay of 3 sec; (B) Pauses of 3.6 sec Duration.
With suspicion of the arrhythmic potential of the Gingko biloba, and no other factors responsible for the bradyarrhythmia, we stopped the medication for 48 h. During her hospital stay, medications to increase the conduction through the atrioventricular node were given when required. (Inj. Atropine 1 cc (0.6 mg). Orally Tab. Etofylline and Theophylline combination along with Orciprenaline was initiated. To facilitate the washout of the drug, intravenous frusemide was used.
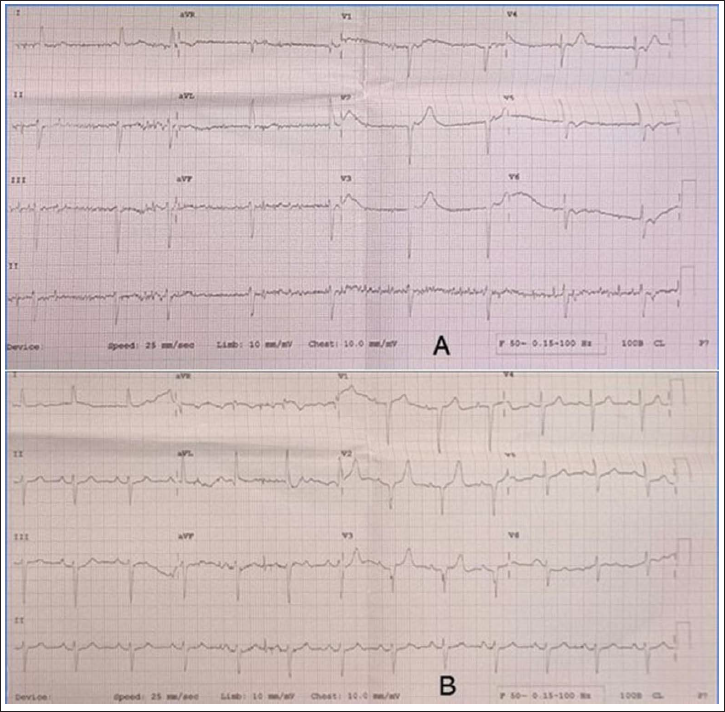
After 48 h off Ginkgo biloba, repeat electrocardiography (Figure 3) showed normal sinus rhythm, rate of 77 bpm. Each P wave was followed by the QRS complex. The corrected QT interval was normal.
Electrocardiogram (A) at Admission Showing Bradycardia with a Heart Rate of 52 bpm, Junctional Rhythm (B). After 48 h of Stopping the Gingko biloba showed Normal Sinus Rhythm with a Rate of 75 bpm.
Discussion
Dietary supplements are a worldwide business worth over 100 US$ billion annually. Up to 50% of adults and one-third of youngsters take these supplements in economically sophisticated countries. Ginkgo biloba is the most used herbal supplement worldwide. 3 During the COVID-19 pandemic, its use has increased due to its effect on improving immunity. 4
Ginkgo biloba, or the maidenhair tree, is a traditionally used herbal medicine in China. Besides reports of improving immunity, and memory, it is easily available online.
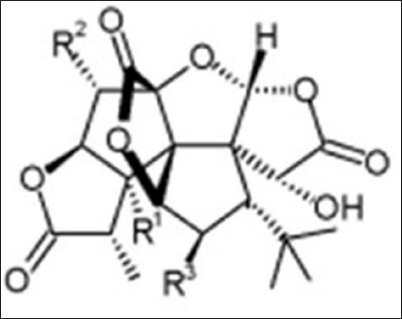
The primary elements responsible for the pharmacological activity linked to Ginkgo biloba include flavanol glycosides (kaempferol, quercetin, and isorhamnetin), diterpenes, and sesquiterpenes. They are abundant in the plant leaves, the extract of which is used as a supplement. Ginkgolides are diterpenes comprising 6 five-membered rings containing a spiro nonane system, three lactones, and a tetrahydrofuran, incorporating a tert-butyl group5–8 (Figure 4).
Chemical Structure of Ginkgolides. Based on the R1, R2, and R3―Being Either H, OH, or Both They Are Categorized as A, B, C, J, and M.
It has varied mechanisms of action 1, As an antioxidant regulating the oxidative stress by activation of the Akt/Nrf2 pathway 2, free radical scavenger 3, antiplatelet effect 4, modulating the activity of various ion channels. Inhibition of the calcium channels, delayed rectifier potassium channels, and inward rectifier potassium channels leads to shortened ventricular action potential. It inhibits hyperpolarization-activated cyclic nucleotide-gated channels 2 and 4, present in the sinoatrial node and the ventricles affecting the heart rate.9, 10
The above mechanisms imply that Ginkgo biloba compounds can modify the cardiomyocyte ion channels resulting in various impacts on the electrophysiological characteristics of the heart.
Common side effects of Ginkgo are nonspecific and include headache, nausea, diarrhea, and rash. The most severe is an increased bleeding risk because of the antiplatelet effect. The literature on the proarrhythmic effects of Gingko biloba is sparse.
Umegaki et al. (2000) and Moulton et al. (2001) demonstrated a significant decrease in blood pressure and heart rate in patients using Ginkgo biloba.11, 12 Cianfrocca et al. (2002) described palpitations on the use of Ginkgo biloba. 13 The described case had a left bundle branch pattern that resolved when the drug was discontinued. According to research by Kubota et al. (2002), Ginkgo biloba may provoke atrial arrhythmias more likely. 14 Pfister et al. (2008) described an electrical storm in a patient with ischemic cardiomyopathy using Ginkgo biloba. 15 Satoh (2004) demonstrated the unique effects of Ginkgo biloba and its effect on action potential duration and cationic currents in mouse ventricular myocytes. 16 Russo et al. (2011) in his study described the association between Ginkgo biloba and Atrial fibrillation, which was improved after discontinuation of the drug. 17 Natour et al. (2020) demonstrated the effect of Ginkgo biloba and its association with ventricular arrhythmias. 18 These studies provide evidence supporting our case report.
Conclusion
Ginkgo biloba leaf extract is among the most commonly used herbal supplements worldwide. Consideration regarding Ginkgo and other herbal medicines should be a part of every arrhythmia evaluation. This case demonstrates the potential arrhythmic side effects of Ginkgo biloba.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.