
Abstract
Minimally invasive cardiac surgery is performed for cardiac procedures through a small incision similar to laparoscopy for abdominal surgeries to facilitate faster wound healing, early recovery, better cosmesis, and early resumption of work. Minimally invasive cardiac surgery needs longer instruments, training in specialized centers, a prolonged learning curve, and prolonged cardiopulmonary bypass and aortic cross-clamp time. This article is a brief review of minimally invasive cardiac surgery.
Keywords
Introduction
Minimally invasive cardiac surgery (MICS) involves performing cardiac procedures through a smaller incision in lieu of a conventional full sternotomy approach with the goal of reducing the invasiveness and morbidity of the procedure. 1
Levels of MICS
Based on the size of the skin incision used for accessing the pericardial cavity, MICS is divided into four levels. Level 1 is under direct vision with a limited 10- to 12-cm skin incision; level 2 is under direct vision or video-assisted with a miniincision of 4–6 cm; level 3 is video-directed or robotic-assisted with a microincision of 1.2–4 cm; and level 4 is telemanipulation with port access with a less than 1.2 cm incision.
Types of procedures that can be performed in MICS include surgeries for valvular heart diseases, including the Bentall procedure, atrial mass excision, coronary artery bypass surgery (CABG), and a few RACHS-1 congenital heart diseases.
Using a different set of instruments that are longer than those used in the open sternotomy approach, MICS is indicated as conventional surgery with limitations such as the need for different access (multivessel coronary artery disease), the presence of peripheral vascular disease (hindered peripheral cannulation), atherosclerosis of the abdominal or thoracic aorta (risk of atheroembolism), extreme body habitus or chest deformities, prior cardiothoracic surgeries, previous chest infection leading to pleuropericardial adhesions, and redo surgeries (Figures 1–4). 2
Cygnet Aortic Cross Clamp.

Cosgroove Aortic Cross Clamp.

MICS Needle Holder.

Knot Pusher.

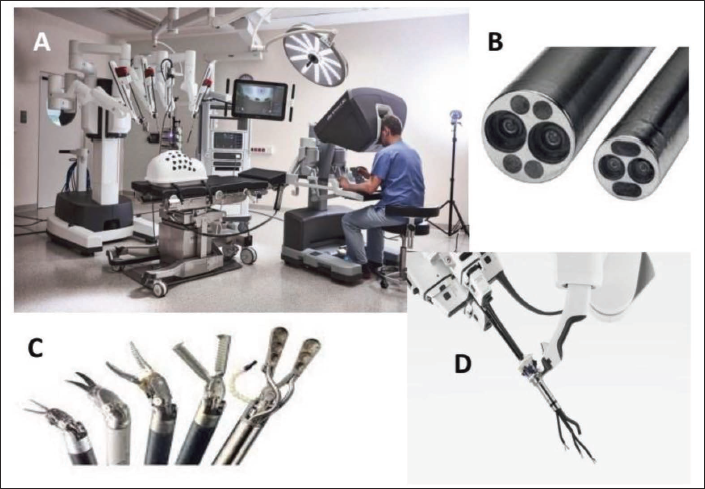
The approaches used in MICS are the upper ministernotomy for aortic valve surgery and thymectomy, the lower ministernotomy for mitral and tricuspid valve surgeries, the parasternal approach, the right minithoracotomy for mitral and tricuspid valve surgeries, atrial septal defect closure, excision of atrial mass, the left minithoracotomy for CABG, the subxiphoid approach for the pericardial window, epicardial ablation, and so on.3, 4 In addition, video assistance, 3 port access for instrumentation, and robotic telemanipulation using the Da Vinci Surgical System facilitate MICS through smaller incisions. (Figure 5).
Da Vinci Robotic Surgical System.
The complications of the parasternal approach are the chances of parasternal chest hernia, sternal instability with ministernotomy, and injury to the internal mammary artery.
Preoperation Preparation for MICS
In addition to routine preparation for cardiac surgery through open sternotomy under general intravenous anesthesia, performing MICS requires additional preparation such as Doppler or CT angiographic evaluation 5 of the femoral artery and vein along with the carotid, renal, and radial arteries for patency, size, and screening for atherosclerosis; a chest roentgenogram or computerized tomography to evaluate the relation between intercostal spaces (ICS), ribs, sternum, ascending aorta, and all valves; to rule out lung diseases, pleural adhesions, and so on, which preclude MICS. 6
Prerequisites for MICS
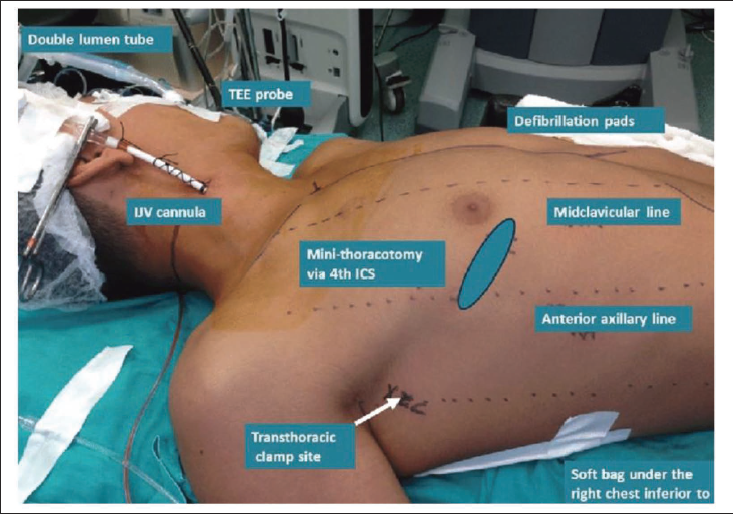
Double lumen endotracheal intubation or bronchial blocker for single lung ventilation, 3 intraoperative transesophageal echocardiography (TEE), external defibrillation paddles, groin preparation to access the femoral artery and vein, instruments, patient position, draping, prior informed consent, and instruments for conversion to an open sternotomy in case of difficulty (Figures 6 and 7). Intraoperative TEE is necessary for confirmation of catheter position (femoral vein cannula, retrograde cardioplegia cannula, etc.), looking for atherosclerosis of the thoracic and abdominal aorta, post-procedure completion of de-airing of cardiac chambers, ventricular and valvular function, residual gradients, regurgitation or paravalvular leak, and so on.
Femoral Artery Cannula.

Femoral Vein Cannula.

Short-acting anesthetics are used in MICS to facilitate early extubation.
Position of the Patient
Supine position with 30° elevation of the right side of the chest for right minithoracotomy (Figure 8).
Patient Position for MICS.
Brief Steps of the Surgical Procedure
In groin preparation for exposure of the femoral artery and vein to facilitate femor-femoral bypass, a 5–6 cm skin incision is made in the second ICS, right midclavicular line for aortic valve surgery, or in the third ICS along the anterior axillary line for mitral and tricuspid valve surgeries, and in the left fifth ICS/inframammary fold for CABG. 3 A single 1 cm incision is made in the seventh ICS, mid-axillary line, for cardiotomy vent or drain placement. 5 The pectoralis major muscle is incised or split along the superior border of the lower rib, the intercostal muscles are incised along the upper border of the rib, the internal mammary artery is secured or ligated, and the pleural space is entered. A soft tissue retractor is placed, followed by a rib retractor. The lung is deflated, and a 3–4 cm pericardiotomy is done 5 cm anterior to the phrenic nerve, and pericardial stay sutures are placed. A telescopic camera can be used to improve visualization.
Cannulation Strategies
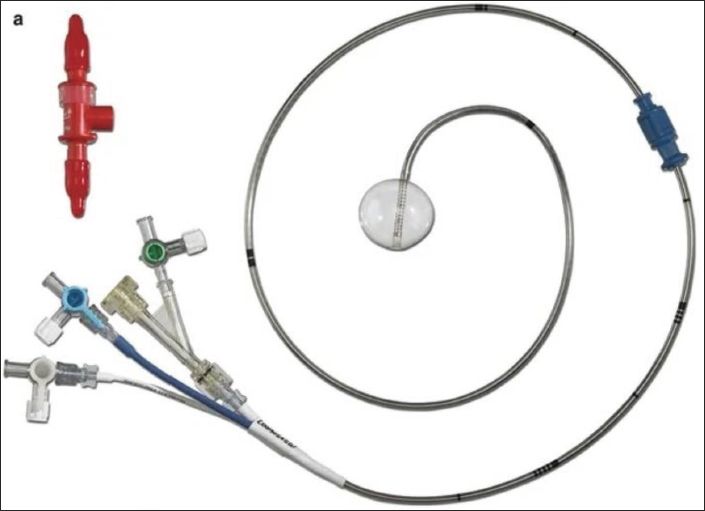
Options for arterial cannulation are direct aortic cannulation (antegrade arterial perfusion), femoral (retrograde arterial perfusion), or axillary artery cannulation and venous drainage through the femoral and/or internal jugular vein. The femoral artery is cannulated using the Seldinger technique. Venous drainage is augmented with vacuum assistance (40–60 mmHg). Cardioplegia delivery can be antegrade through the aortic root using a long cannula or retrograde through the coronary sinus. 2 An aortic cross-clamp can be an external Chitwood, flexible Cosgroove, cygnet clamp, or endoaortic balloon occlusion. 5 Rapid-fire suture ligature devices facilitate a faster procedure (Figures 9 and 10). 1
Endoballoon.
Left Atrial Retractor System.

Carbon dioxide is flooded into the pericardial cavity during the procedure to avoid an air embolism.
Intraoperative TEE is used for confirmation of the position of the femoral vein cannula and retrograde cardioplegia cannula, preoperative assessment of valvular structure and function, and postoperative assessment of complete de-airing, ventricular and valvular function.
A standard surgical procedure is performed. After completion of rewarming, cardiopulmonary bypass is gradually weaned off and decannulated. All vascular access sites are repaired, and complete hemostasis is secured. The pericardium is closed with 2–3 sutures. A chest tube is placed. 4 Intercostal nerve block for early postoperative analgesia. 1 The chest wall is closed in layers.
Postoperative management is followed as per hospital protocol. Early extubation and drain removal on the first postoperative day ease early mobilization. 5
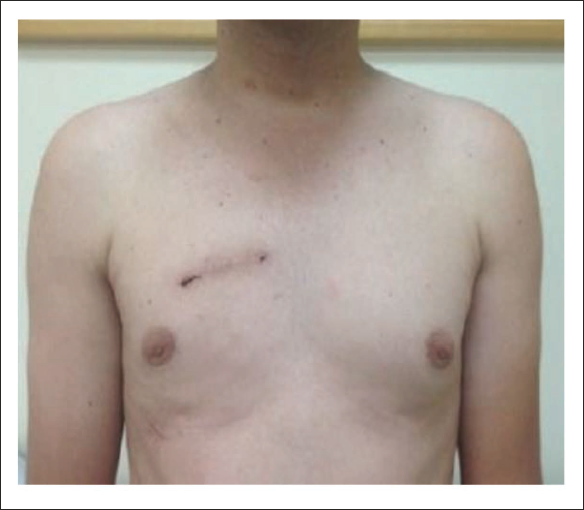
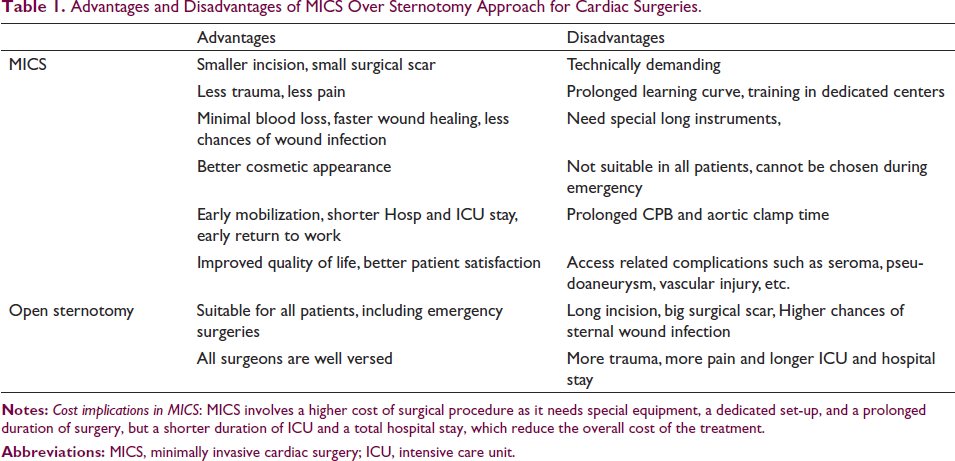
The advantages of MICS are a small incision and small scar, less trauma and pain, minimal blood loss, faster wound healing, lower chances of wound infection, few wound-related complications, better cosmetic appearance, early mobilization, shorter ICU and overall hospital stay, quick recovery, early return to work, improved quality of life, and better patient satisfaction (Figure 11). 2
Post Operative Surgical Scar in MICS AVR.
Challenges with MICS are technically demanding; procedures need to be performed using long instruments from a greater distance, leading to a steep learning curve; they need training in dedicated centers where large numbers of cases are performed; they need additional equipment that is expensive; they may need conversion to open sternotomy in cases of difficulty; and they are not suitable for all patients and situations,2, 6 whereas the open sternotomy approach has withstood the test of time, provides wide and near complete access to all cardiac structures, maximum control of circulation and breathing, and is comfortable for all cardiac surgeons.
Possible complications in MICS are longer operative time (including bypass time and aortic cross-clamp time), 7 which can be overcome with experience, and access site complications such as dissection, pseudoaneurysm, hematoma, infection, seroma/lymphocele, increased risk of stroke, and so on. Preoperative screening for atherosclerosis/peripheral vascular disease can reduce the incidence of stroke (Table 1 and Figures 12–14). 6
Advantages and Disadvantages of MICS Over Sternotomy Approach for Cardiac Surgeries.
Open Surgery Left Atrial Retractor.

Open Surgical Instruments.

Postoperative Surgical Scar in Open Sternotomy.

Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ehical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Not applicable.