
Abstract
Background
Prosthetic valve thrombosis bears significant risks of morbidity and mortality. In our study, we explore the risk factors associated with thrombolysis for thrombosis of prosthetic valves of the heart.
Materials and Methods
This is a hospital-based cross-sectional study with 60 patients with valve replacement between 25 and 60 years. Using an organized questionnaire we have obtained data on sociodemographic, behavioral risk factors, and previous history of other medical conditions.
Results and Discussion
The incidence of prosthetic valve thrombosis was 4% (n = 60). The prevalence of aortic valve thrombosis was found to be 3.4% and mitral valve thrombosis was 5.2%. The mean age group of the study population was 30 ± 10 years. The incidence was highest (31%) in the 30–40 years age group. Aortic valve thrombosis was the most common (n = 48, 80%). The overall mortality was 38% (n = 23). The mortality rate due to Aortic valve and Mitral valvar thrombosis was 41.06% (n = 20) and 20% (n = 3), respectively. Sub-therapeutic international normalized ratio (INR) was noted in 86% (n = 52) patients and drug non-compliance was 70% (n = 42). All patients underwent thrombolysis, considering the higher severity of functional class. The risk factors significant for mortality were previous history of valve thrombosis, subtherapeutic INR and aortic valve.
Conclusions
Aoretic valve prosthetic valve thrombosis was the most common and the overall mortality was higher in women. High mortality was observed in the cohort. Previous history of thrombosis and subtherapeutic INR is an important risk factor for mortality.
Introduction
Rheumatic heart disease accounts for the majority of valve pathology in developing countries like India.1–4 Surgical valve replacement is presently the cornerstone of therapy for individuals having valvular heart disease. 5 There are several varieties of prosthetic surgical heart valves in mechanical and biological types. 6 The mechanical heart valves are more prone to have a thrombogenic nature, but also are more durable. The incidence of post-valvular valvular thrombosis may reach 13% in the first year. Prosthetic valve thrombosis with mechanical heart valves occurs at a rate ranging between 0.1% and 5.7% per year. Higher rates are observed with mechanical heart valves implanted in the mitral and tricuspid positions. Experience regarding the same is limited in India. In our study, from a tertiary care center, we studied the incidence of prosthetic valve thrombosis in patients with rheumatic heart diseases, and risk factors for mortality.
Materials and Methods
Study Design and Population
This cross-sectional study was conducted at Department of Cardiology at Stanley Medical College, Chennai, India (January 2005 to January 2016).
Sample Size and Sampling Methodologies
Inclusion criteria were as follows: patients who had undergone valve replacement at the tertiary hospital due to rheumatic heart valve disease and who were on regular follow-up; patients who were in the 25–60 age group; NYHA Class III–IV. The exclusion criteria were: patients more than 60 years; pregnancy; the ejection fraction of the left ventricle <40%; pannus in echocardiography as the cause of obstruction; congenital heart diseases; patients with bio-prosthetic valves, and patients with NYHA Class I–II.
Data Collection
We used a standardized proforma to obtain data on socio-demographic information, behavioral risk points and history of previous other diseases. We also analyzed the clinical data and prescription for medication and clinical laboratory reports. After receiving proper consent, the transthoracic echocardiography examination was done.
Methodology
The study included 60 patients who had been admitted to a critical care center between the month of January in 2005 and month of January in 2016 and who satisfied the clinical & echocardiographic criteria for prosthetic valvular malfunction due to thrombosis. Significant dyspnea, orthopnea, and/or paroxysmal nocturnal dyspnea, along with signs of pulmonary venous congestion, were considered to be clinical indicators of prosthetic valve obstruction. These symptoms were linked to absent prosthetic valve clicks with or without audible stenotic or regurgitant murmurs across the prosthetic valve. Calculated valve areas of less than 1.5 cm2 in the mitral and tricuspid locations, along with end-diastolic gradients of more than 10 mmHg, were echocardiographic indicators of prosthetic valve occlusion. Peak systolic gradients greater than 50 mmHg were considered abnormal in the aortic position. Studies of leaflet movement were evaluated by using transthoracic echocardiography. Thrombolysis was performed with streptokinase over 24 hours as intravenous infusion to attain a complete response. The results of Chest X-ray and Doppler transthoracic echocardiogram from baseline were compared to other reports from complications. At the time of admission, mean international normalized ratio (INR) less than 2.0 for aortic valve replacements and less than 2.5 for double valve or mitral valve replacements was considered to be in the sub-therapeutic range.
Statistical Analysis
The patient data was recorded classified and analyzed using SPSS Version 27.0 statistical analysis software. Medical and clinical laboratory tests, as well as sociodemographic data, were taken into account as additional explanatory variables. Using mean and standard deviation for quantitative variables, frequency, and percentages for categorical variables and descriptive analysis of the explanatory and outcome variables were carried out. Non-parametric and unpaired student t-tests and the Wilcoxon-Mann-Whitney test were employed to evaluate quantitative data for low-grade and high-grade subjects, as well as cardiovascular information, between two groups of patients. For predictors of mortality, binomial logistic regression analysis was used. For qualitative data, the p value was calculated using the Chi-square test and the Fisher exact test. A difference of p value of <.05 was considered statistically significant.
Protection of Human Subjects
This study was approved by Stanley Medical College Chennai, Tamil Nadu under the Institutional Human Ethical Committee. Informed written consent was obtained from the patient for the study. Informed consent was obtained from the participants about the study’s purpose, complications, and advantages. Throughout the course of the study, participants’ private information and statistical data were kept private.
Results
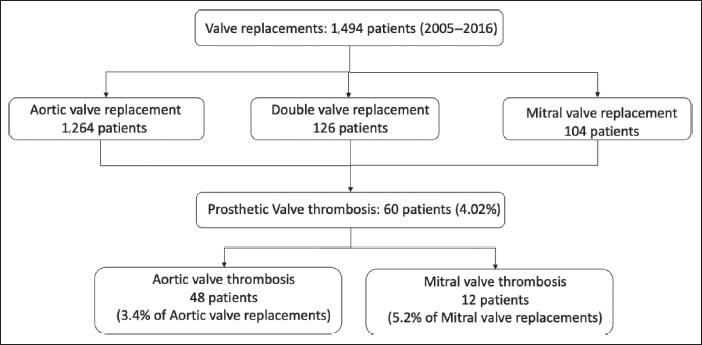
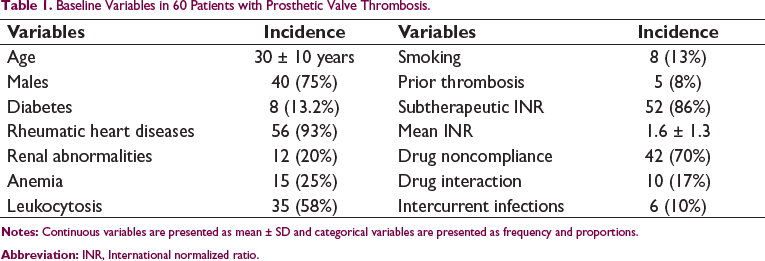
In the period between January 2005 to January 2016, 1,494 valve replacement surgeries were performed at our center (Figure 1). The mean follow-up period of the patients was 5 ± 1 years. The incidence of prosthetic valve thrombosis was 4% (n = 60). The incidence of aortic valve and mitral valve thrombosis was 3.4% (n = 48) and 5.2% (n = 12), respectively. The mean age group of this study was 30 ± 10 years (Table 1). The mean time interval to onset of prosthetic valve thrombosis from the time of surgery was 9 ± 4 months. The mean time interval was 11 ± 3 months for post-aortic valve replacement and 6 ± 5 months for post-mitral valve replacement. The mean interval time between onset of symptoms and diagnosis was 56 ± 30 days. Diabetes (n = 8, 13.2%), renal abnormalities (n = 12, 20%), anemia (n = 15, 25%), leukocytosis (n = 35, 58%), smoking (n = 8, 13%), and prior thrombosis of prosthetic valve (n = 5, 8%) were the co-morbidities in the study population (Table 1). Higher prevalence of thrombosis was noted in the age group of 30–40 years (31%). The NYHA class of symptoms at presentation were NYHA Class III (n = 46, 76%) and NYHA Class IV (n = 14, 24%).
Flow-chart of Patients Presenting with Prosthetic Valve Thrombosis.
Baseline Variables in 60 Patients with Prosthetic Valve Thrombosis.
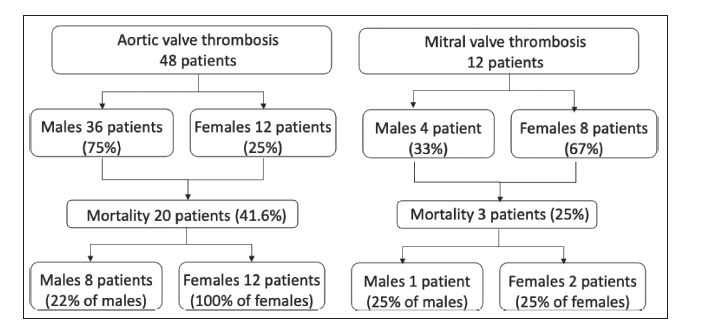
The number of patients with prosthetic valve thrombosis was 60 (Figure 2). The aortic valve was the most involved valve (80%). Females had greater incidence of mitral valve thrombosis. Females had an 18% greater prevalence of valve thrombosis. The incidence of mortality due to aortic valve thrombosis was 41.6%. Women died from aortic valve thrombosis at a rate that was greater (100%) than men (30%). The risk of death from a mitral valve thrombosis was comparable between males and females (25% each) (Figure 2).
Flow-chart of Mortality Outcomes in Patients with Prosthetic Valve Thrombosis According to Gender.
Overall, the subtherapeutic INR was 86.6%. (n = 58, mean 1.6 ± 1.3) (Table 1). The sub-therapeutic INR was higher in women (94%) than in men (76%). In the study population, drug noncompliance was 70% (n = 42). Women (80%) were less likely to comply than men (56%). Inadequate hospital visits for titration of INR (73%), medication interactions (17%), illnesses (10%), and nutrients interactions (5%), as well as food interactions (5%), were the causes of drug non-compliance. Thrombolysis resulted in reduction of symptoms and prosthetic valve gradients. Systemic embolization after thrombolysis was noticed in 10% of the study population. Systemic embolization was reported in women at a rate of 11%, slightly higher than men at 8%. Patients were not taken for surgery.
Predictors of Mortality in Patients with Prosthetic Valve Thrombosis.
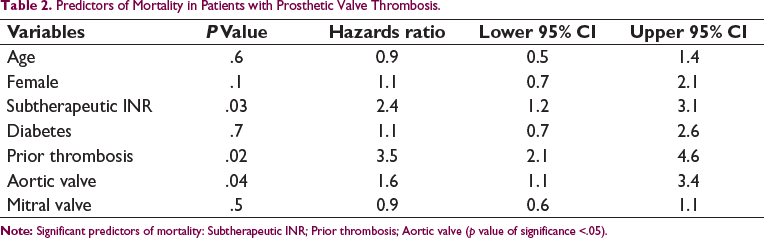
The incidence of mortality in patients with prosthetic valve thrombosis is 38% (n = 23) in the follow-up period of 4 ± 3 months. Significant predictors of mortality by binomial logistic regression analysis are presented in Table 2. Prior thrombosis, subtherapeutic INR and aortic valve had the highest hazards of mortality- 3.5 (2.1–4.6), 2.4 (1.2–3.1) and 1.6 (1.1–3.4), respectively. Among patients with prior history of prosthetic valve thrombosis, only one person survived the second episode. Female gender and coexistent diabetes were not significant predictors when adjusted for other confounders as suggested by the logistic regression model (Hosmer & Lemeshow test of model p = .7 suggested good fit).
Discussion
Our study has highlighted a few important findings: high incidence of aortic valve thrombosis in the cohort; high incidence of mortality due to prosthetic valve thrombosis in patients managed with thrombolysis only; prior prosthetic valve thrombosis and subtherapeutic INR at presentation are significant predictors of mortality.
Prosthetic valve thrombosis is a pathological condition defined by the development of thrombus on prosthetic structures and followed by prosthetic valve dysfunction with or without thromboembolism. 7 It is worth noting that decreased leaflet motion occurs more frequently in individuals with sub-therapeutic INR. 8 The same finding is reiterated in our study cohort also, as sub-therapeutic INR was an important predictor of both prosthetic valve thrombosis and mortality. A detailed review of over 200 published data on left-sided prosthetic valve thrombolysis represented that 82% of patients experienced initial stage success, 12% patients had thromboembolism, 5% to 10% of patients experienced stroke, 6% of patients died, 5% major bleeding episodes, and 11% of patients experienced recurrent thrombosis. 5 The higher incidence of aortic prosthetic valve thrombosis in our cohort and distribution of comorbidities in this cohort is similar to the prior studies in literature. However, our study has also highlighted the higher incidence of prosthetic valve thrombosis in women, primarily due to drug non-compliance and sub-therapeutic INR. A substantial incidence of thromboembolism can be brought on by individuals with artificial heart valves that are receiving insufficient anticoagulation.
Surgical mortality is minimal without thrombolysis in functional Classes I or II, compared to the 12%–17% embolic risk brought on by thrombolysis. However, if the surgical risk is significant as in patients with functional Class III or IV symptoms, fibrinolysis therapy may be a bail-out strategy due to high surgical risks. 9 The other indications for surgery include blockage brought on by endocarditis, abscess formation and typically very big thrombi with obstruction. To choose between thrombolysis and surgery, the benefits and risks of the numerous circumstances affecting each patient must be weighed against the knowledge and experience at each facility. In our study, though reduction in trans-valvular gradients could be achieved with thrombolysis, significant mortality of 38% was noted in this cohort. High mortality could be directly related to the higher functional class of presentation in this cohort.
The study has important limitations. This is a retrospective analysis of patients admitted with prosthetic valve thrombosis. There are inherent limitations of an observational study with no case-control design. The interpretation of the results might not be generalized as the outcomes were specific to the cohort.
Conclusion
In our study, aortic valve prosthetic valve thrombosis was the most common location of prosthetic valve thrombosis. The overall mortality was higher in women. Drug noncompliance was the most common reason for prosthetic valve thrombosis. Subtherapeutic INR and prior history of prosthetic valve thrombosis are significant predictors of mortality. Though thrombolytic therapy is an important bail-out strategy, systemic embolization post-thrombolysis was an important risk factor for mortality.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.