
Abstract
Coronary artery disease (CAD) represents the leading cause of death in adults and Myocardial infarction (MI) is the lethal manifestation of that. Although males and females beyond certain age are prone to CAD, young men and/or women also suffer from MI. Apart from the rare case reports of non-athermatous coronary artery disease including hyper-coagulable states, spontaneous dissections and/or substance abuse in young MI, the prevalence of conventional risk factors are on rise in young adults and children. The protection offered by young age has been overshadowed by the increased prevalence of these risk factors. To evaluate the prevalence of such conventional risk factors and angiographic pattern in young MI, we did an observational, retrospective study at our tertiary care center. It was observed that one-fourth of young MI had no conventional risk factors and among the rest, obesity (48%) was most common, followed by diabetes mellitus (DM) (32%), Hypertension (29.5%), smoking (15.5%), alcoholism (11%), and a family history of premature CAD (3%). Among the participants, 35.5%, 22.5%, 12%, 4%, and 1% of patients had one, two, three, four, and five risk factors, respectively. On angiography, Left Anterior Descending (LAD) was the most commonly diseased coronary artery (77%) followed by Right Coronary Artery (RCA) (30.5%) and Left Circumflex (LCx) (29.5%). Single-vessel disease (SVD) (69.5%) was the most frequent observation on CAG, whereas 24% and 6.5% of patients had double-vessel and triple-vessel disease (DVD, TVD), respectively.
Keywords
Introduction
Coronary artery disease (CAD) has a substantial impact on patient morbidity and mortality. 1 South Asian populations have demonstrated a concerning increase in the incidence of CAD in younger age groups. The risk of premature CAD in Indians is higher (5–10%) than other ethnicities (~1–2%). 2 Over the past two decades, there has been a significant rise in the prevalence of conventional risk factors such as obesity, physical inactivity, hypertension, etc. in younger adults. 3 History of prior myocardial infarction (MI), heart failure (HF), tobacco use, and diabetes strongly predict the long-term outcome in young CAD patients. 4 The occurrence of CAD in the absence of conventional CV risk factors is not uncommon. Novel risk factors such as increased levels of homocysteine and lipoprotein (a) also contribute to CAD in younger populations. 5 The coronary artery risk development in young adults (CARDIA) study has shown that increased hostility such as anger and psychological stress predispose young adults to coronary artery calcification (CAC) thereby documenting the fact that stress may be an another presently unrecognized risk factor for CAD. 6
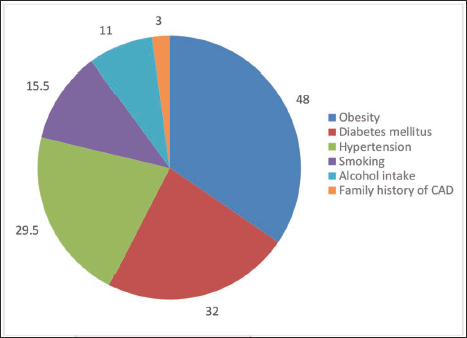
Any young CAD patient should be offered angiographic evaluation to improve the outcomes with early revascularization. 7 Angiographically, a greater prevalence of single vessel disease (SVD) with involvement of left anterior descending artery (LAD) is observed in young CAD.7, 8 Furthermore, normal coronaries may be encountered in nearly 8–22% of patients. 2 Studies in Indian populations reflect similar patterns with smoking, obesity, and hypertension being common risk factors for CAD.9, 10 Despite advances in medical education and informatics, in addition to an increased awareness within the general population, the incidence of young CAD has not declined. 11 As an increase in the prevalence of CAD in young people is expected, it is especially necessary to look at risk factor profiles in young adults, especially those of Indian descent (Figure 1).
Distribution of CV Risk Factors.
Materials and Methods
Design and Population
This was a single-center, cross-sectional observational study conducted at a tertiary care hospital in North India. Participants presenting with Acute MI (aged 18–45 years of age) who underwent coronary angioplasty for CAD were included in the study. Informed consent was obtained from all the participants before enrollment. Any participant with acute MI, within window period, who did not give consent for angiography were thrombolysed and excluded from the study. The study was approved by the institutional ethical committee and was conducted with applicable principles of good clinical practice and local regulatory principles.
Methods
Participants who fulfilled the recruitment criteria were eligible for enrollment into the study. Participants presenting with signs and symptoms of ischemic heart disease (IHD) underwent an initial electrocardiographic (ECG) assessment. Presenting features such as chest pain, dyspnea on exertion, epigastric pain, etc. were recorded in structure case record form (CRF). Acute MI was defined by rise in cardiac biomarkers (troponins) along with the presence of ischemic symptoms, ST elevation or depression on ECG, development of pathological Q-waves, or echocardiographic evidence of new regional wall motion abnormality. All the features observed on ECG were recorded in the CRF. Patientsʼ demographic details such as age and gender were captured. After confirming the initial diagnosis of participants, patients were subjected to clinical assessments and a catheterization lab.
Risk Factors Assessment
Blood pressure (BP) was measured with an electronic apparatus. Hypertension (HT) was considered if the average BP of a participant was more than 130/80 mmHg and/or the the participant was taking medications for control of HT irrespective of BP levels.
Diabetes mellitus (DM) was considered if a random test of the patient’s blood sugar was ≥ 200 mg/dL, if the glycosylated hemoglobin (HbA1c) was ≥ 6.5%, or if the participant was taking medications for control of hyperglycemia irrespective of blood sugar levels.12, 13
A current smoker was defined as a person who is either smoking any form of tobacco at least once a day or having any level of tobacco smoking within one month of the index event. 14
Obesity was defined using the body mass index (BMI) criteria for South Asians. 15 Accordingly, participants with BMI of <18.5 kg/m2, 18.5–22.9 kg/m2, 23.0–24.9 kg/m2, and 25.0 kg/m2 or higher were categorized as underweight, normal, overweight, and obese, respectively.
A positive family history of premature CAD was considered if a primary male or female relative was diagnosed with CAD before the age of 55 years or 65 years, respectively. 16
Coronary Angiography Procedure
Using the radial approach,17 a 2 mm catheter was inserted and a soft J-shaped guidewire was progressed through the catheter retrogradely under the fluoroscopy guidance. With proper manipulations of the catheter, the guidewire was advanced to the base of the aorta immediately above the aortic valve to engage the tip of the catheter in the coronary ostium. A radiocontrast dye (5–15 mL) was passed through the catheter to visualize the coronaries using fluoroscopy. Cine images of both the right and left coronary arteries with their branches were obtained. The lesions were assessed for significant or non-significant stenosis, in addition to other characteristics such as length, position of side branches, etc.
Statistical Analysis
Compiled data were analyzed using the statistical program SPSS 22 (SPSS IBM, Chicago, Illinois). Continuous data were presented as mean and standard deviation (SD) and analyzed using an independent student t-test or one-way analysis of variance (ANOVA). For categorical data, percentages were compared using the Chi-square test. P value < .5 was considered significant for all comparisons.
Results
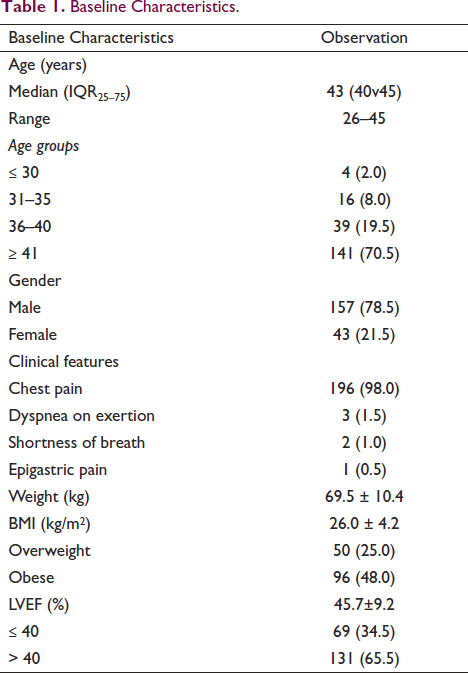
Among the 200 participants, patient’s age ranged from 26 to 45 years with the median age being 43 years. 70.5% of patients were in the age group of 41–45 years. The proportion of males (78.5%) in the participant population was higher than females (21.5%). Chest pain was the major symptom. The mean BMI was 26.0 ± 4.2 kg/m2. The proportion of overweight and obese participants was 25% and 48%, respectively. The mean left ventricular ejection fraction (LVEF) was 45.7±9. 2%, and 34.5% of patients had an LVEF 40% or lower.
Table 1 depicts the baseline characteristics of study participants.
Baseline Characteristics.
Among CV risk factors (Table 2), obesity (48%) was most common, followed by DM (32%), HT (29.5%), smoking (15.5%), alcoholism (11%), and family history of premature CAD (3%). There was no known CV risk factor identified in 25% of patients. Among the participants, 35.5%, 22.5%, 12%, 4%, and 1% of patients had one, two, three, four, and five risk factors, respectively.
Distribution of Cardiovascular Risk Factors.
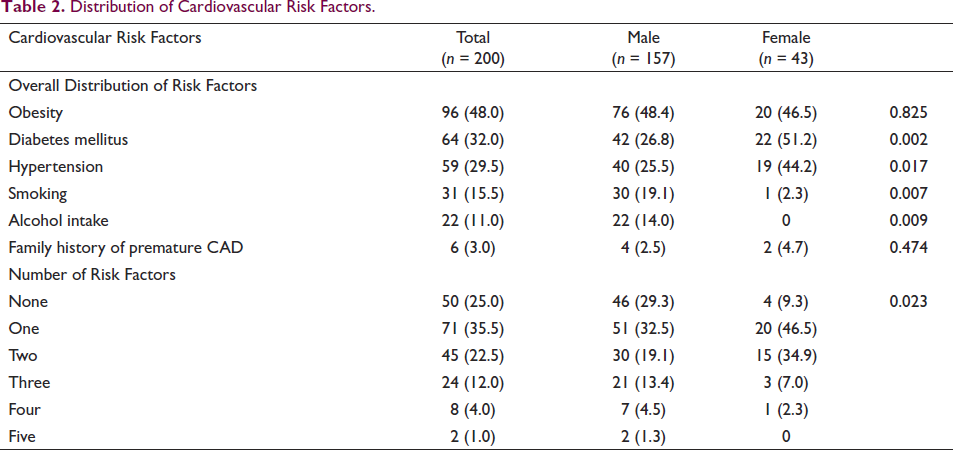
Table 3 presents the coronary angiography profiles of the patients. LAD was the most commonly diseased coronary artery, that is, in 77% of patients, followed by Right Coronary Artery (RCA) (30.5%) and Left Circumflex (LCx) (29.5%). Single-vessel disease (SVD) (69.5%) was the most frequent observation on CAG, whereas 24% and 6.5% of patients had double-vessel and triple-vessel disease (DVD, TVD), respectively. In SVD, LAD, RCA, and LCx involvement was evident in 50%, 12.5%, and 7% of patients, respectively. LAD and LCx involvement (12.5%) was the most common DVD, followed by LAD and RCA (8%) and RCA and LCx (3.5%).
Coronary Angiography Profile of Study Participants.
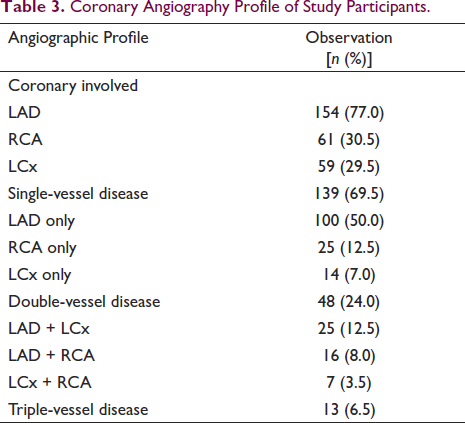
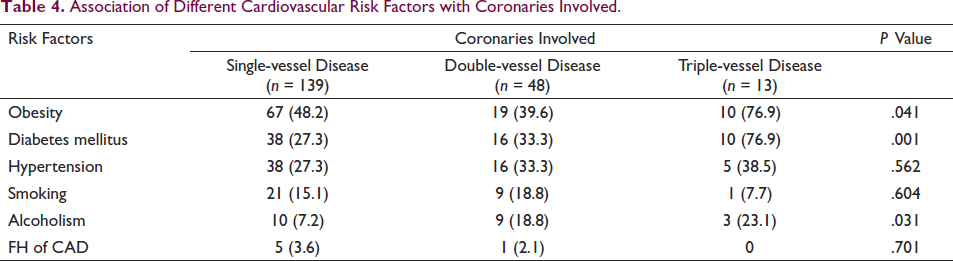
Table 4 describes the association of various CV risk factors with coronary involvement. A significantly higher proportion of patients with TVD had obesity (76.9%, p = .041) and DM (76.9%, p = .001) compared to those with SVD (48. 2% obese and 27. 3% diabetic) or DVD (39.6% obese and 33. 3% diabetic). Though the proportion of patients with TVD who had HT (38.5%) was higher, the distribution was non-significant (p = .562) compared to SVD (27. 3%) and DVD (33. 3%) patients. Alcoholism was observed with significantly greater frequency in TVD patients than SVD and DVD (23.1% vs. 7. 2% and 18.8%; p = .031). Distributions of patients who were smokers (p = .604) or who had a family history of premature CAD (p = .701) were non-significant.
Association of Different Cardiovascular Risk Factors with Coronaries Involved.
The association of participant characteristics with coronary artery is shown in Table 5. There was no significant difference in mean age and mean BMI among the three groups
Association of Participant Characteristics with Coronaries Involved.
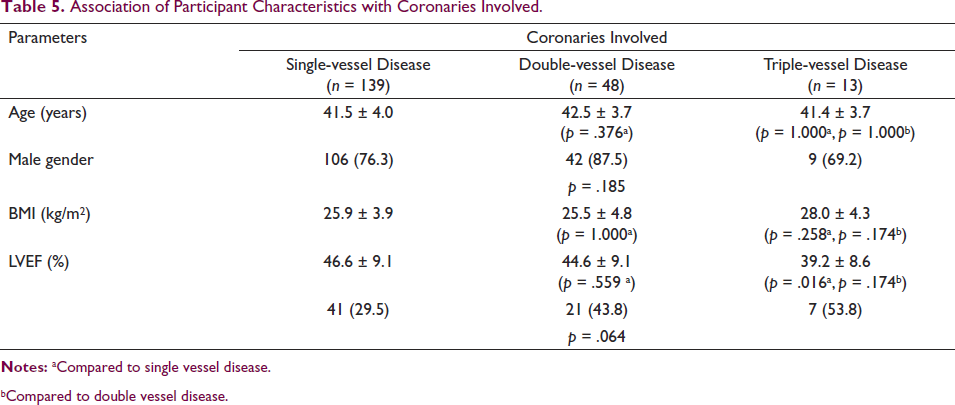
bCompared to double vessel disease.
Discussion
In this study, obesity, DM, and HT were observed as the common risk factors for CAD in young adults. The number of risk factors, 35.5% of patients had one, 22.5% had two, and 12% had three risk factors. Interestingly, one-fourth of patients had no identifiable risk factor for CAD. LAD was the most common coronary involved, while single-vessel disease (69.5%) was the most common angiographic observation.
CAD in younger individuals is common in the Indian population. The INTERHEART study proved that the mean age of CAD onset was a decade earlier in South Asians compared to Western populations. 18 In our study, the median age of the young CAD patients was 43 years of age with the majority being above the age of 41, the incidence was higher in males than females.
Bhardwaj et al. 9 reported similar observations: the mean age was 35.94 ± years and the incidence of CAD in young was almost exclusively reported in males (99. 2%). 9 Young CAD presents with classic symptoms such as chest pain, which was the one that was most frequently presented in this study. Thus, every case of chest pain should be thoroughly investigated, even in younger individuals. Among the other classic CV risk factors, obesity, diabetes, hypertension, smoking, alcoholism, and family history of premature CAD were observed in decreasing frequency. Multiple studies from India reported similar observations. In a study from North India, Sinha et al. reported smoking, FH of premature CAD, obesity, physical inactivity, and stressful life events as risk factors in 78.5%, 46.8%, 39.1%, 38.7%, and 29.6% of young CAD individuals, respectively. 10 Another study from North India by Aggarwal et al. reported dyslipidemia, smoking, low high-density lipoprotein cholesterol (HDL-C), and central obesity in 91%, 74. 3%, 68.9%, and 47.7% of young CAD individuals, respectively. 19 Women had a greater prevalence of DM and HT, whereas smoking and alcoholism were exclusively observed in males. Cole et al. also observed a significantly higher prevalence of HT and DM in women than in men, whereas no differences were reported in family history, smoking, and prior MI. 4 This indicates that risk factors may significantly vary between the two genders. Furthermore, one or more risk factors act in synergism to lead to CAD. We found that 35.5% of participants had a single risk factor, 22.5% had two risk factors and 12% had three risk factors. Compared to females, males had a greater number of risk factors in combination. A study from Sekhri et al. reported two or more risk factors in 78.6% of subjects. 20 The study also found that this was more common in males than females (86.9% vs. 33.46%, respectively). 20 Another interesting observation was that one-fourth of the participants had no identifiable CV risk factor. This could be because not every CV risk factor was evaluated. Dyslipidemia, dietary factors, psychological stress, lipoprotein (a), homocysteine levels, drug abuse (e.g., cocaine), and other disorders such as hypothyroidism and autoimmune disorders also affect the risk of CAD.2, 4, 6, 21
In our study, LAD (77%) involvement was most common with near equal involvements of RCA and LCx. SVD (69.5%) was the most common angiographic finding, followed by double-vessel and TVD. Kumbhalkar et al. had similar findings with LAD involvement in 82.5% of subjects, followed by RCA (12.5%) and LCx (5%). Single-, double-, and triple-vessel disease was reported in 57.1%, 11.5%, and 7.1% of subjects, respectively. 22 Participants with obesity, DM and alcoholism had significantly higher proportions of TVD. Compared to non-diabetics, Cole et al. observed higher rates of double-vessel and triple-vessel disease in subjects with DM. 4 Age and gender did not differ according to the coronaries involved. Mean ejection fraction (EF) was significantly lower with triple-vessel involvement, indicating declining cardiac function. This was supported by observing a proportionately higher number of individuals with LVEF <40% in TVD. Our findings agree with the observation from Machal et al. The study reported factors such as age, increased BMI, DM, low EF, left main stenosis, and genetic variation in the IL-6 promoter as independent predictors of mortality in TVD. 23
Our study, however, had certain limitations. Dyslipidemia, an important risk factor was not evaluated in the study patients. Additional genetic factor (such as polymorphism) which may play a role in modulating the CAD risk was also not assessed. Association of risk factors with mortality and outcome could have helped design strategies to target those risk factors. Furthermore, comparing CV risk factors to older age groups also could have provided further insights on differences in CV risk factor profiles in multiple age groups which could have helped us in delineating the disease process at an early stage, giving better management opportunities.
Conclusion
Young MI in India is on a rise and apart from affecting the health status, it also hampers the economic growth of the country. Many risk factors contribute to the early onset of CAD and more the number of risk factors, higher the incidence of CAD and earlier an onset. This study highlighted the association of conventional risk factors with CAD in young adults and also specified the quarter of young adults who suffered MI in absence of conventional risk factors signifying the fact that there can be various unknown and unconventional risk factors in later subgroups of patients as well. In addition, this study highlighted the risk stratification in young MI patients as those with triple-vessel disease were more common in the presence of multiple risk factors and were more prone to develop HF. Thus, evaluation of risk factors and identifying the angiographic profile of young MI patients can help strategize the management strategies to improve the long-term outcomes in young individuals with CAD.
Footnotes
Acknowledegment
These statements are on behalf of the authors of this manuscript. We certify that the above information is correct, and we would like to submit case report towards the journal for publication.
Ethical Approval
The original research has received Ethical Committee approval.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.