
Abstract
Congenital anomalies involving coronary artery origin are rare, with an incidence of 0.24%–1.3%. We present a case of inferior wall ST-elevation myocardial infarction in which an emergency coronary angiogram showed occlusion of the right coronary artery. However, we were unable to cannulate the left main coronary artery during the event. Interpretation of the infarct-related artery was complicated by the right arm-left arm lead reversal in electrocardiogram, adding to the dilemma in localizing the culprit vessel, namely right versus left circumflex coronary artery-related myocardial infarction. A computed tomography coronary angiogram subsequently showed the left main coronary artery having abnormal origin from the right sinus of Valsalva with inter-arterial course and no lesions in the left circumflex.
Introduction
Congenital anomalies involving coronary artery origin are rare, with an incidence of 0.24%–1.3%.1, 2 One of the most dangerous anomalies is the left main coronary artery (LMCA) originating from the right sinus of Valsalva as it predisposes to sudden cardiac death. 3 However, encountering an ST-elevation myocardial infarction (STEMI) with thrombotic occlusion of the right coronary artery (RCA) and LMCA having abnormal origin from the right sinus with inter-arterial course is challenging in many aspects, especially with the lead reversal in the presenting electrocardiogram. We report a similar case where failure to localize the LMCA origin forced us to order a computed tomography (CT) coronary angiography (CTCA).
Case Report
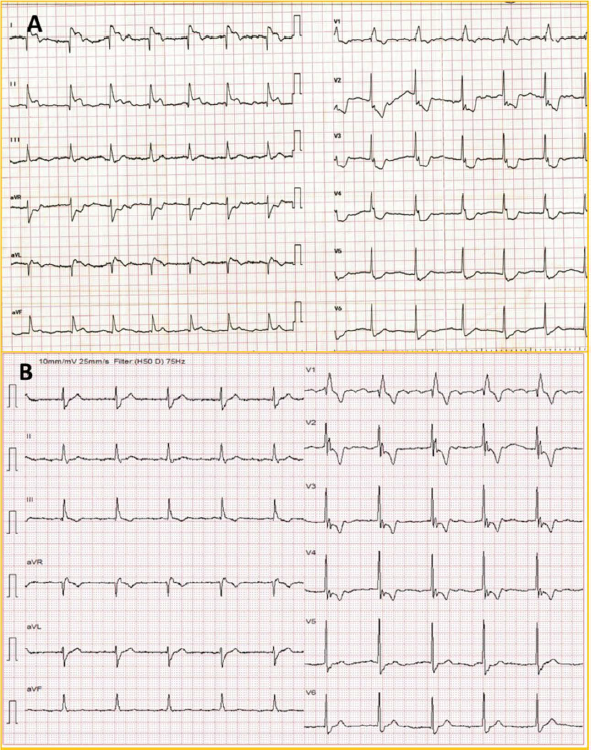
A 76-year-old gentleman with sick sinus syndrome, atrial standstill, junctional rhythm, right bundle branch block (RBBB) with left posterior hemi-block, who had undergone single chamber VVI pacemaker implantation in 2017, presented with acute onset retro-sternal chest pain. On examination, vitals were stable with ongoing angina. Presenting troponin T was normal. ECG (electrocardiogram) (Figure 1A) showed atrial fibrillation with junctional rhythm and RBBB with concordant ST elevation in leads II, III, and aVF, and discordant ST elevation in I and aVL along with precordial V2-V6 ST segment depression. In view of ST elevation in inferolateral leads (II > III), the left circumflex coronary (LCX) artery was suspected as the culprit artery. An alpha loop in the proximal right radial artery precluded the procedure via the radial route (Figure 2A). Right femoral access was taken, and the right coronary angiogram showed proximal RCA total occlusion (Figure 2C). After the failure of initial attempts to cannulate LMCA (Figure 2B), ECG was reviewed. ECG was noted to have the lead reversal of the right arm (RA) and the left arm (LA), which was overlooked in the emergency room (Figure 1B). ECG review suggested that the occlusive MI was due to RCA rather than LCX, and RCA angioplasty was performed. The final angiogram showed TIMI III flow and no complications (Figure 2D; Supplementary Video 1). However, the LMCA origin could not be identified despite multiple attempts and aortic root angiogram, and the procedure was stopped considering ST resolution and pain relief. Subsequently, a CTCA was done to delineate coronary anatomy.
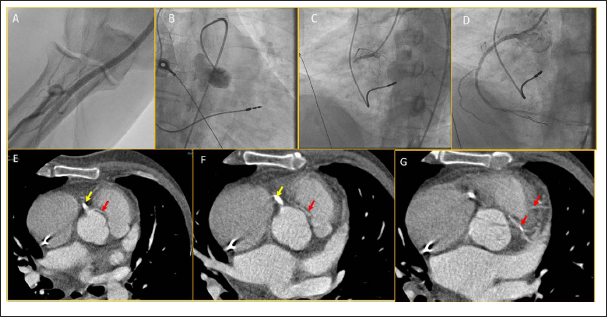
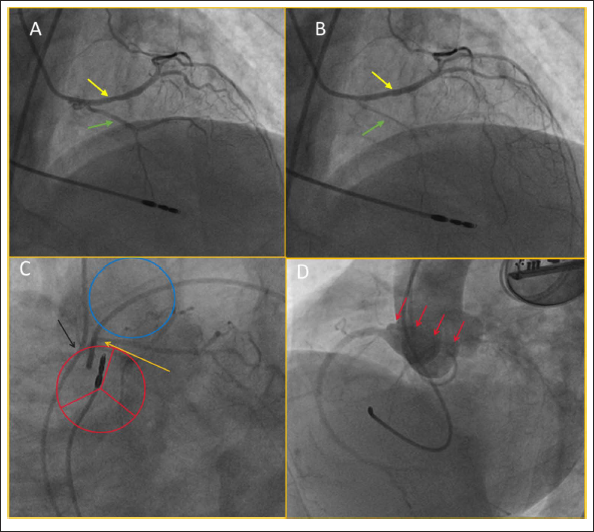
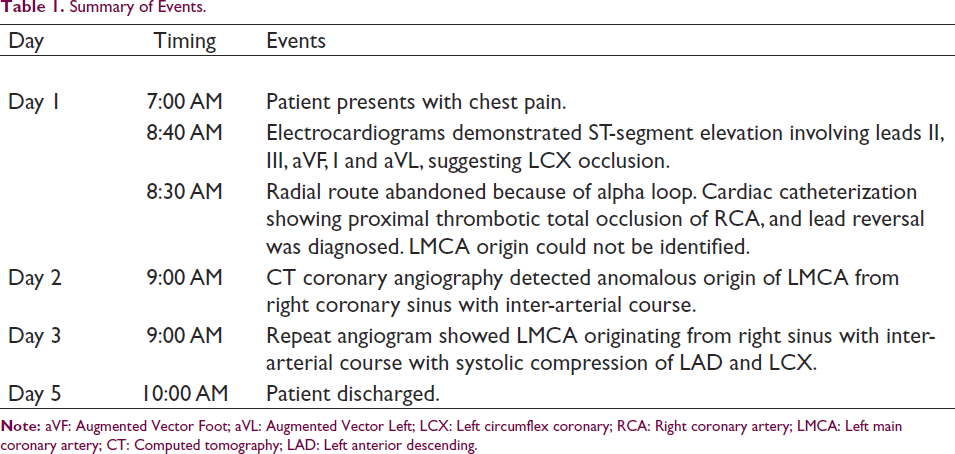
CTCA showed the abnormal origin of LMCA from right sinus immediately anterior to the RCA origin, with inter-arterial course divided into the left anterior descending (LAD) artery and LCX (Figure 2E-2G; Supplementary Video 2). The radiologist could not ascertain disease-free status because of inter-arterial compression during systole. Hence, next day the patient was planned for CAG for understanding the status of the left coronary. CAG showed an abnormal LMCA origin, a short LMCA, type I LAD and systolic compression of LAD and LCX (Figure 3A-3D; Supplementary Videos 3-8). No flow-limiting lesions were seen. Thereafter, his hospital stay was uneventful, and considering type-I LAD and old age, he was planned for medical follow-up. A summary of events is provided in Table 1.
A. AP cranial view showing short LMCA, type-I small LAD (green arrow). LAD and LCX (yellow arrow) are normal in diastole. B. Systole showing compression of LAD due to inter-arterial course (green arrow), minimal compression of LCX at a basal state (yellow arrow). C. LAO caudal view showing inter-arterial course (arrows) black: RCA origin from right sinus, orange: LMCA originating from the same sinus nearby and dividing after short distance. Red circle: possible depiction of aortic sinuses; blue circle: pulmonary root. D. Aortic root angiogram showing abnormal LMCA origin from right sinus (first red arrow of the panel) and course is inter-arterial. AP, anterior-posterior; LMCA, left main coronary artery; LAD, left anterior descending; LCX, left circumflex coronary; LAO, left anterior oblique; RCA, right coronary artery.
Summary of Events.
Discussion
Lead reversal in acute MI is not uncommon causing significant diagnostic dilemma, especially creating confusion between RCA and LCX as the culprit artery in inferior wall STEMI. 4 ST elevation in the high lateral leads (I and aVL) with ST vector toward the left and ST elevation more in lead II than lead III suggested LCX as the culprit in our case (Figure 1A). However, noting RCA proximal occlusion in the coronary angiogram, a review of presenting ECG showed the LA-RA lead reversal (Figure 2B). We did not repeat the ECG with correct lead placement because the patient was already undergoing angiography at that time. In the LA-RA lead reversal, lead aVF remains unchanged, leads aVL and aVR switch places, leads II and III switch places, and lead I becomes inverted. In our case, lead reversal could not be appropriately identified because of the absence of P wave and baseline RBBB. Post-procedure ECG showing initial R in lead I and sharp upward deflection compared to the first ECG suggests that it had shown lead reversal. Our patient also had right ventricular (RV) paced beats, baseline RBBB beats, and fusion beats occasionally with accelerated idioventricular rhythm (AIVR) intermittently (Supplementary Figure 1). After confirming CTCA findings, the coronary angiogram showed the abnormal LMCA origin from right coronary sinus, and LAD could be seen compressed during systole (Figure 3). Classically, 4 possible courses with “eye” and “dot” sign of LMCA have been described from the right sinus (Supplementary Figure 2).5, 6 These are: the septal course, likely benign; the anterior course, anterior to RV outflow tract, likely benign; inter-arterial, most often associated with sudden cardiac arrest; and retro-aortic, usually benign. We feel that the left anterior oblique (LAO) caudal view is much easier to identify the abnormal course than the previously published eye and dot signs in the right anterior oblique (RAO) view.
The clinical presentation of these patients varies from asymptomatic detection to angina, dyspnea, syncope, and in a vast number of cases, sudden cardiac death.7, 8 CTCA is the investigation of choice. 9 Surgical intervention is a class I recommendation in patients with known diagnosis irrespective of symptomatic status. 10 Surgical un-roofing is the procedure of choice for coronaries having intramural course, whereas re-implantation, ostial reconstruction, or pulmonary artery translocation is done if there is no intramural course.11–13
Conclusion
This case reemphasizes the fact that all patients with acute coronary syndrome need a critical evaluation of ECG before they are taken to the cath lab. Absent P wave, paced rhythm, and baseline bundle branch block make it challenging to identify lead reversal in ECG. Anomalous LMCA with an inter-arterial course can have a malignant presentation, although it can be a benign bystander of the primary event, as in this case.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for A Case Report of Primary Angioplasty: The Triple Whammy! by Sudipta Mondal, Bhagwati Prasad Pant and Sreevilasam P Abhilash, in Indian Journal of Clinical Cardiology
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for A Case Report of Primary Angioplasty: The Triple Whammy! by Sudipta Mondal, Bhagwati Prasad Pant and Sreevilasam P Abhilash, in Indian Journal of Clinical Cardiology
Footnotes
Learning Points
Declaration of Conflicting of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
The authors confirm that the consent for submission and publication of this case report has been obtained from the patient in line with the Committee on Publication Ethics guidance.
Ethical Approval
Not required according to guidelines as it is an anonymous case report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.