
Abstract
The association of total anomalous pulmonary venous connection (TAPVC) with transposition of great arteries (TGA) is a very rare combination of 2 congenital cyanotic heart diseases. TAPVC, in the case of TGA with the intact interventricular septum (IVS), is a cause of early regression of the left ventricle (LV). Very few cases of this rare combination (TAPVC and TGA with or without VSD) have been reported in the world of literature. We found 10 case reports in the literature. The minimum age was 6 days and the maximum age of 16 years. 5 of them, which were operated before 1990, underwent atrial switch with TAPVC repair. Other 4 of them, operated after 1995, underwent arterial switch with TAPVC repair. In this case report we are reporting 2 such rare cases. In both cases, large VSD prevented LV regression.
Introduction
Transposition of great arteries (TGA) and total anomalous pulmonary venous connection (TAPVC) are cyanotic congenital heart diseases with an incidence of 20 to 33 per 100,000 live births and 6 per 100,000 live births 1 respectively. The association of TAPVC with TGA is a very rare combination of 2 congenital cyanotic heart diseases. One pathology alters the hemodynamics of the other. A combination of TAPVC and TGA with intact interventricular septum (IVS) results in early regression of LV. Very few cases of this rare combination have been reported in the world of literature.2–10 Here, we report 2 infants, 1 with d-TGA, ventricular septal defect (VSD) with obstructed supracardiac TAPVC and the other with d-TGA, VSD with infra-diaphragmatic TAPVC, who underwent successful repair. Fortunately, because of VSD, LV is preserved in both cases.
Case 1
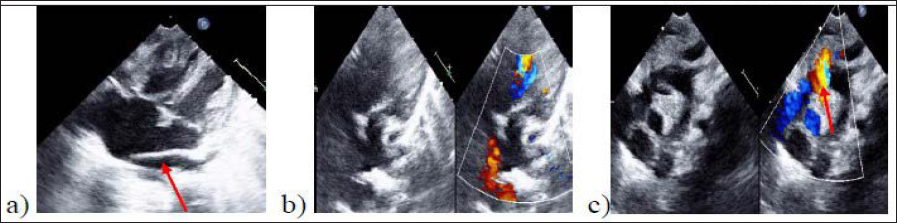
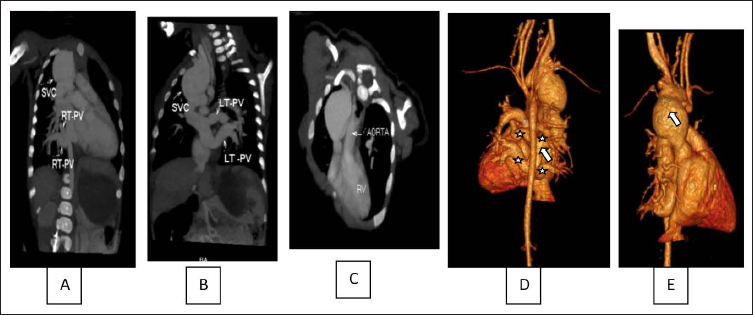
A 2-month-old, 3.8 kg female infant presented with complaints of nonacceptance of feeds and respiratory distress. On examination, the baby was dull with respiratory distress and chest retractions, oxygen saturation of 83% on room air. On auscultation, S1 was normal with single loud S2, ejection systolic murmur in the right second intercostal space with bilateral crepts in lung fields. The baby’s x-ray showed mild cardiomegaly and an increased pulmonary venous pattern. ECG showed sinus rhythm, tall P waves, right axis deviation with QRS axis 120 to 150 degrees and right ventricular hypertrophy. A 2d echocardiogram revealed situs solitus, d-looping, d-TGA, large membranous VSD, and all 4 pulmonary veins draining via a right vertical vein into SVC with obstruction at the opening into the SVC (Figure 1). CT angiogram was also done to delineate the anatomy before proceeding to surgery which confirmed our diagnosis (Figure 2).
(A) Apical 4C View Showing Common Chamber (Arrow), Dilated RA and RV (B) Pulmonary Artery Arising from LV (C) Right Vertical Vein Obstructed at the Opening in to SVC (Arrow).
(A) CT Angiogram Showing the Right Pulmonary Veins Draining into SVC (B) Left Pulmonary Veins Draining into the SVC (C) Aorta Arising from the RV (D) 4 Pulmonary Veins (Star) Forming Common Chamber (Arrow) (E) Dilated SVC (Arrow).
The baby underwent arterial switch surgery, TAPVC repair and VSD closure. Cardiopulmonary bypass time was 287 minutes with an aortic clamp time of 153 minutes. The chest was closed on the second day of surgery because of the high risk of bleeding due to prolonged cardiopulmonary bypass time. The baby was extubated on the third postoperative day. The baby was shifted to wards on the fourth postoperative period with minimal oxygen support. Oxygen support was gradually weaned off and the baby was discharged on the eighth post-op day. Follow-up after 1½ years of surgery showed normal hemodynamics and normal growth and development.
Case 2
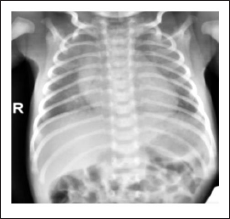
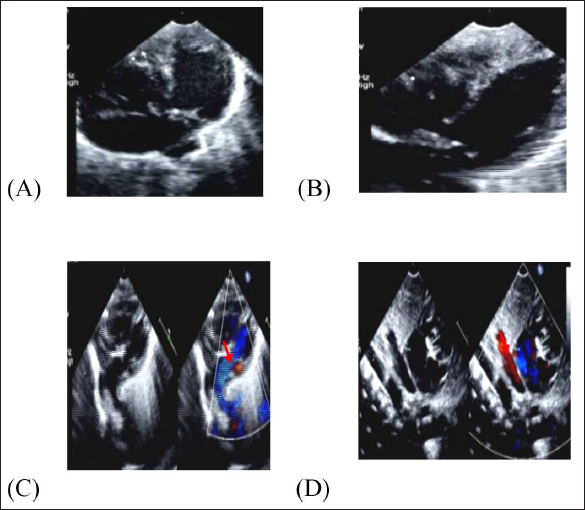
5 days old, 2.6 kg male neonate presented with respiratory distress and oxygen saturation—88% on room air. On examination, the baby had respiratory distress, no clinical cyanosis, single S2, and ejection systolic murmur in the right parasternal area, and bilateral crepitations in lung fields. Chest X-ray showed a cardiothoracic ratio of 0.55 with congested lungs (Figure 3). ECG showed sinus rhythm, normal P waves, right axis deviation with QRS axis 120 degrees, and right ventricular hypertrophy. 2d echocardiography showed situs solitus, d-looping, d-TGA, all 4 pulmonary veins draining into a single common chamber and draining into the portal vein via a vertical vein, a large inlet VSD and an additional small apical muscular VSD (Figure 4).
CXR Showing Bilateral Congested Lungs With Cardiomegaly.
(A) Apical 4C View Showing AV Concordance with Dilated RA and RV (B) 2d Echo Showing Moderate Size VSD (C) Image Showing the Pulmonary Artery (Arrow) Arising from LV (D) Image Showing the Vertical Vein (Arrow) Draining in to the Portal Vein.
The baby underwent ASO, TAPVC repair and VSD surgical closure. Cardiopulmonary bypass time was 236 minutes with an aortic clamp time of 147 minutes. Chest closure was done on first postoperative day. The baby was extubated on third postoperative day. Immediate postoperative period baby revealed culture positive sepsis. The hospital stay was 10 days.
At a follow-up after 9 months, the baby had normal growth and development with normal echo parameters.
Discussion
Hemodynamics in TAPVC associated with TGA is different from that of isolated TGA and TAPVC. One defect partly corrects the negative hemodynamic consequences of the other. There will be relatively high saturations when compared to isolated TGA. TAPVC delivers all pulmonary venous return to the systemic side of the heart and avoids overloading of the pulmonary circulation. TAPVC with TGA-IVS is a cause of early regression of the LV.
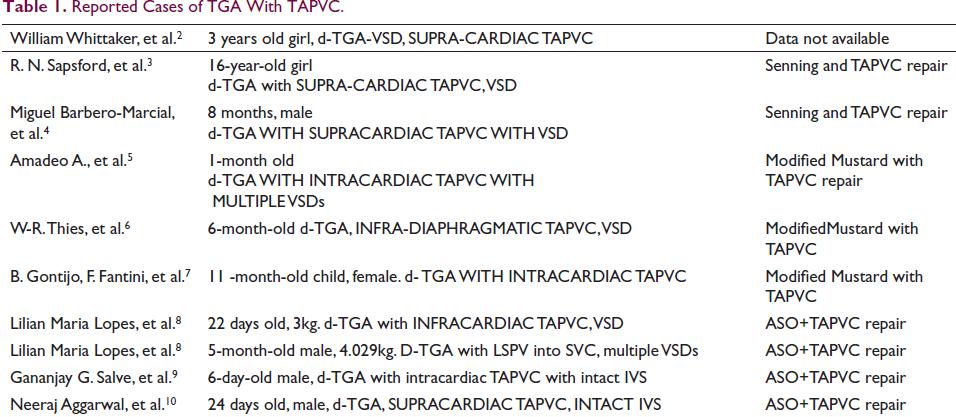
We found 10 case reports in the literature (Table 1). The age ranged from 6 days to 16 years. 2 of them underwent a Senning operation along with TAPVC repair, 3 underwent the Mustard operation and TAPVC repair and the other 4 of them underwent arterial switch with TAPVC repair. Until early 1990s many centers preferred atrial switch irrespective of LV size. The 2 cases reported here underwent complete anatomical repair that is arterial switch operation and TAPVC repair.
Reported Cases of TGA With TAPVC.
Conclusion
The clinical picture of TGA with intact IVS changes when associated with TAPVC. Because of relatively high saturations, the patient may present late and by that time LV might have regressed. The presence of VSD or large PDA or VSD with pulmonary stenosis may help in preserving the LV. Therefore TAPVC should be suspected in the case of TGA with intact IVS and early LV regression, and in infants presenting with high saturations with inadequate mixing communication. Arterial switch operation can be performed successfully along with TAPVC repair after assessing the LV mass and its capability to receive aorta.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
This article is a letter to the editor. No patient is subjected to any newer and unapproved pharmacological or interventional. so ethical committee approval is not required.