
Abstract
Cardiovocal syndrome or Ortner’s syndrome can be caused due to a myriad of etiologies in the neck or mediastinum. The syndrome can also be a consequence of many cardiac or mediastinal pathologies or even complications of surgical treatment. The objective of this research was to systematically review to provide an overview of the etiopathogenesis of Cardiovocal syndrome or Ortner’s syndrome. Cochrane Handbook for Systematic Reviews was used for the methodology of the review and the review adhered to the “Preferred Reporting Items for Systematic Review and Meta-analysis Protocols” PRISMA protocol. The database PubMed and ClinicalKey were searched using prompts “hoarseness” OR “recurrent laryngeal nerve paralysis” AND “Ortne’s syndrome” OR “Cardiovocal syndrome” OR “aneurysm” OR “thoracic aorta” OR “unilateral vocal fold paralysis.” After data extraction synthesis was done based on the 24 most relevant and recent publications reporting and outlining this condition. Newer investigative modalities like Videolaryngostroboscopy and Transcutaneous laryngeal ultrasound (TLUSG) are useful for early recognition of this condition before the development of Aortic dissection or Rupture of Aortic Aneurysm. Cardiac physicians and Otolaryngologists must remain vigilant to the sudden onset of left vocal cord palsy as it can be an early warning sign of an ominous mediastinal pathology.
Keywords
Introduction
Unilateral vocal fold paresis, also synonymous with unilateral abductor paralysis of the vocal cord, is a disorder in which the muscle that separates the vocal cord is weakened or paralyzed. The fixation brought on by muscular infiltration by tumors or ankylosis or fixity of the cricoarytenoid joint should be distinguished from this one. 1
Hoarseness, difficulty speaking, and trouble breathing are all symptoms of left vocal fold paralysis. The branch of the vagus nerve known as the recurrent laryngeal nerve provides the larynx with motor and sensory fibers (voice box). 1 This branch of the Vagus nerve loops around neck structures like the aortic arch before supplying the larynx hence it is named “recurrent.” 1
Damage to the recurrent laryngeal nerve, which is the nerve that regulates the movement of the vocal cord, is the most frequent cause of abductor paralysis. Surgery (such as thyroid surgery), radiation therapy, tumors, infections, and specific medical diseases are some of the factors that lead to recurrent laryngeal nerve injury (such as sarcoidosis). 1
Speaking difficulties and hoarseness can result from injury to the recurrent laryngeal nerve, which can also impair breathing. It is frequently harmed after thyroid surgery, which might cause paralysis of the vocal cords. The pitch may be off due to loss of tensors, and the voice may sound weak or breathy due to increased Rima glottidis. Surgery, voice therapy, and speech therapy are all possible forms of treatment for recurrent laryngeal nerve paresis. Treatment options will differ based on the underlying reason and degree of paralysis. 2
Norbert Ortner, an Austrian internist, 1897, described 3 cases of mitral stenosis leading to Left Atrial enlargement, compressing the Left Recurrent laryngeal nerve. 3 This rare condition Ortner’s syndrome, also known as laryngeal neuropathy or laryngeal dysmotility, is marked by hoarseness and difficulties swallowing because of the laryngeal muscles’ weakening or paralysis (voice box) due to causes in Thoracic aorta.
Stocker et al used the term “Cardiovocal syndrome” when they noted the manifestation of left vocal cord paresis associated with cardiovascular disease. 3 In cases where a cause of Ortner’s syndrome or Cardiovocal syndrome cannot be identified, it is left recurrent laryngeal nerve injury dysfunction due to some form of mediastinal compression is presumed to be the pathology. Hoarseness, swallowing issues, and coughing when swallowing are some signs of Ortner’s syndrome. The incidence of Ortner’s syndrome is 1% to 3% of total cases presenting with the extra-laryngeal cause of hoarseness of voice and dysphonia. The disorder is typically not life-threatening but can reduce the patient’s quality of life.1, 2
The primary artery that transports blood from the heart to the rest of the body, the aorta, develops a bulge or dilation known as an aortic aneurysm. Although aneurysms can develop anywhere along the aorta, they are most frequently found in the abdomen. An aneurysm can rupture and cause serious internal bleeding if it grows too large. Age (aortic aneurysms are more common in those over 60), smoking, high blood pressure, a family history of aneurysms, and certain medical diseases like Marfan syndrome or aortic valve disease are also risk factors for aortic aneurysms. 3
The bulging or enlargement of the thoracic aorta condition is known as a thoracic aortic aneurysm (TAA). The disorder develops when the wall of the aorta weakens and protrudes, resulting in a pouch that resembles a balloon. A TAA has the potential to rupture and produce internal bleeding that might be fatal if addressed. Chest or back pain, shortness of breath, and trouble swallowing are all signs of a TAA. 4 A TAA can be treated surgically, endovascularly, and under close observation. The aneurysm’s size, location, and growth rate, as well as the patient’s general condition, will determine the best course of action. 3
Diagnostic imaging procedures like a CT scan, MRI, or ultrasound are frequently used to identify aortic aneurysms. The size, location, and rate of aneurysm growth will all affect the available treatments. Some of the treatment options include monitoring with routine imaging, blood pressure-lowering medication, or surgical surgery.1, 3
Material and Methods
Study Design
A Systematic Review of Case reports and Review was conducted, to provide an overview of the etiopathogenesis of Cardiovocal syndrome or Ortner’s syndrome. Cochrane Collaboration methodology as set out in their handbook was followed, and we also followed the PRISMA guidelines.5, 6, 7
Materials and Methods
This study’s goal was to systematically review the existing corpus of information about the etiopathogenesis of Cardiovocal syndrome or Ortner’s syndrome. The systematic review was conducted using the PRISMA statement and guided by the Cochrane Handbook for Systematic Reviews of Interventions approach.
Prompts “hoarseness” OR “recurrent laryngeal nerve paralysis” AND “Ortner’s syndrome” OR “Cardiovocal syndrome” OR “aneurysm” OR “thoracic aorta” OR “unilateral vocal fold paralysis” were search prompts utilized as search phrases in the search strategy. 6 The “free full-text” filter was applied to searches in the PubMed, and ClinicalKey databases.
The methodological quality of case reports was assessed using the CAse REports (CARE) criteria.8 2,167 articles in all were found by our algorithm. Following an assessment of the titles and abstracts, 23 papers were determined to be pertinent to the study’s objectives, and data were extracted, and synthesis created. 6
Electronic Database Search Strategies for Finding Relevant Literature
Search strategy PubMed, and ClinicalKey, databases were searched using the keywords terms “hoarseness” OR “recurrent laryngeal nerve paralysis” AND “Ortner’s syndrome” OR “Cardiovocal syndrome” OR “aneurysm” OR “thoracic aorta” OR “unilateral vocal fold paralysis.” The thorough search plan is depicted in the PRISMA flowchart depicted. 7 No search filters limitations on dates or languages (if English translations were available) were imposed.
Search Results
Authors, year of publication, type of study, cause of Ortner’s syndrome, pathogenesis, onset of hoarseness, co-morbidities of the patients, number of cases reported, sex, age, treatment given, level of recovery and recovery time were all information that two reviewers independently gathered from the analyzed studies.
Selection of Studies
The papers were also quantitatively examined following the CAse REports (CARE) checklist (
Screening Process
Two independent reviewers conducted database searches and eliminated duplicate entries, and unavailable papers from their compilation following the PRISMA flowchart, as shown in Figure 1. Papers that were unrelated to the subject of the study were excluded. Full texts of selected papers were read to ensure that they complied with the paper inclusion criteria.
Flowchart showing the methodology of our systematic review PRISMA 2020 flow diagram for new systematic reviews which included searches of databases only. 5
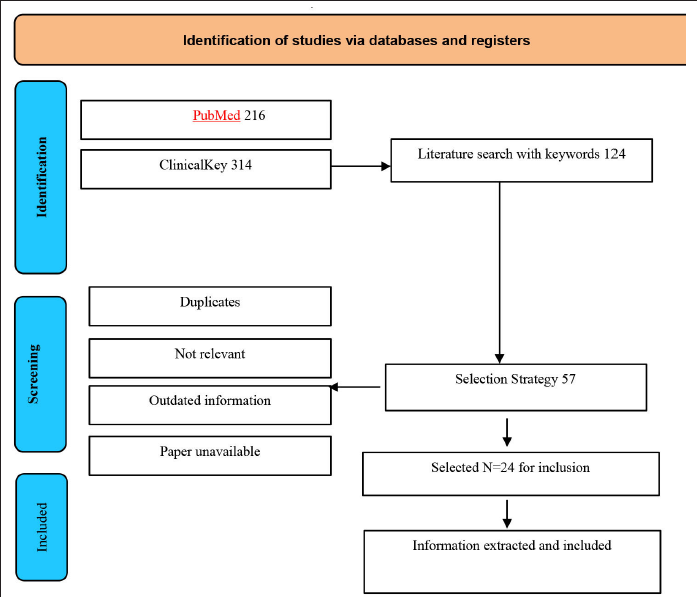
A total of 1,809 articles were accessed throughout the two databases that were methodically searched with the keywords: 216 in PubMed, and 314 in ClinicalKey. The number of identical articles was eliminated bringing the overall to 124. The implication of the publications to the topic of the study was then determined by perusing the titles and abstracts, and 57 were covered. To ensure that the articles met the inclusion requirements and CARE guidelines, 24 were chosen and read in their entirety.
Inclusion and Exclusion Criteria
The following were the inclusion requirements: (a) case report (CR) studies; (b) systematic reviews; (c) anatomical monographs; (d) book chapters (e) monographs related to Ortner’s syndrome and (f) scoping reviews.
The following causes led to the removal of items that did not match the selection criteria: (a) duplicates; (b) outdated information; (c) not relevant information; (e) vague information; (f) no novel information other than “Thoracic aneurysm led to Ortner’s syndrome” (several case reports were found to have no new information); and (g) full-text unavailable for perusal.
Quality of Case Reports
The methodological quality of the CRs included in this study satisfied the criteria outlined in the Materials and methods section and the CARE standards. 8
Choosing Studies
The abstracts and titles of the articles found through the literature search were evaluated separately by the review authors. The Zotero software was used to assess and remove duplicates. Studies that met the predetermined inclusion criteria were chosen. Record management was done using Zotero software. A PRISMA diagram was drawn to demonstrate the flowchart of the SR procedure. Mutual Consensus was used to settle any disputes.
Data Extraction
Data were independently extracted from the included papers by the review writers. Calibration was done to guarantee uniformity among reviewers.
Discussion
Cardiovocal syndrome or Ortner’s syndrome has the highest incidence in the older age group of patients, though it can occur at any age and even in newborns (Patent ductus arteriosus). 9
Symptoms of Unilateral Vocal Fold Paralysis
In adults, unilateral vocal cord paralysis maybe asymptomatic, or can present with vocal fatigue, minimal hoarseness, breathiness of voice, respiratory effort, and aspiration. In children the signs of Unilateral vocal fold paralysis can be subtle, like breathing difficulties, cyanosis, feeding difficulties with chronic aspiration. 10
Signs of Unilateral Vocal Fold Paralysis
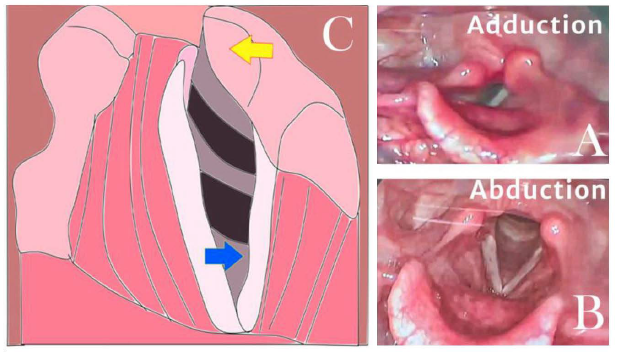
Abnormal ipsilateral pyriform sinus dilatation, a medial deviation of the aryepiglottic fold, left pyriform sinus dilatation, and ipsilateral laryngeal ventricle dilatation, also known as the “sail sign,” are the three most perceptive imaging findings that indicate the existence of Vocal fold paralysis 11 . Left-sided unilateral vocal fold paralysis (ULVFP) is characterized by glottal gaps, lowered position cord, or bowed cord due to loss of tension, and anterior-medial tilt of arytenoid cartilage during respiration. Paretic vocal cords occupy the Para-median position, in comparison to the generally inferred median position, leading to a breathy voice and aspiration of food and water. 12
The signs of Left vocal cord palsy, author’s schematic impression. The blue arrow depicts the lowered position cord or bowed cord3, and the yellow arrow points at anterior-medial tilt of the arytenoid cartilage.5, 9
Etiology and Pathogenesis of Vocal Cord Palsy in Ortner’s Syndrome
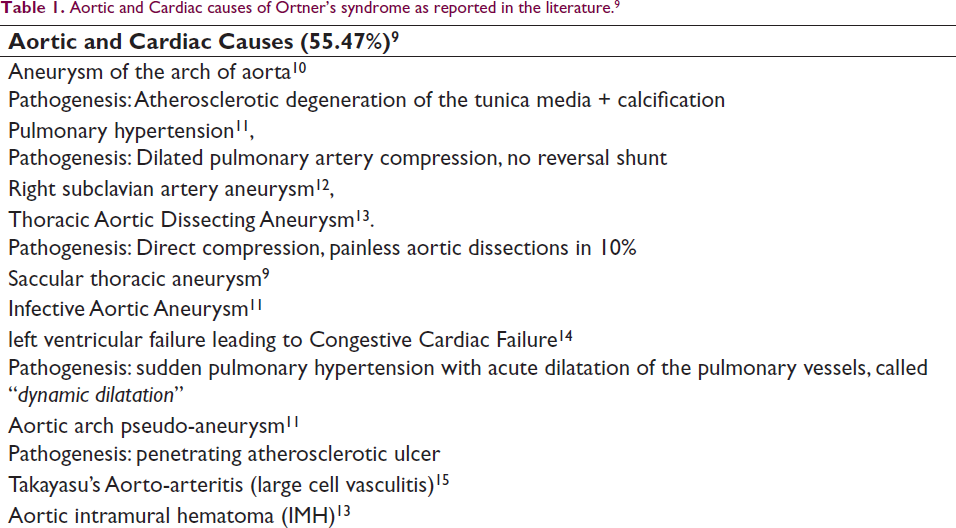
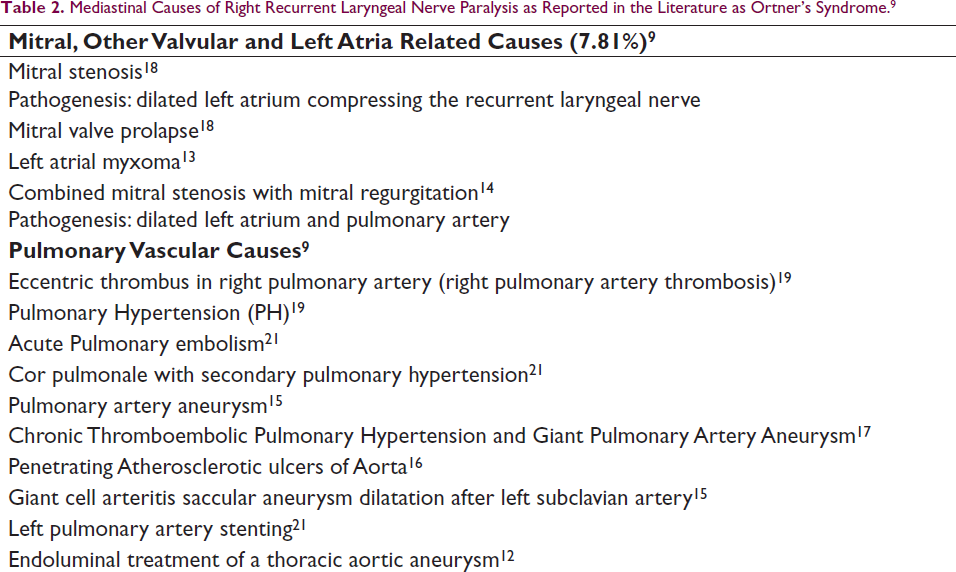
The causes of Ortner’s syndrome as reported by numerous case reports, case series, and systematic reviews, we propose to classify causes as (a) Aortic and Cardiac causes (55.47%); (b) Mitral, other valvular and Left atria related causes (7.81%); (c) Pulmonary Vascular causes (d) Congenital cardiac causes (5.47%); and (e) Extra laryngeal/Mediastinal causes. These are summarized in Table 1.
Aortic and Cardiac causes of Ortner’s syndrome as reported in the literature. 9
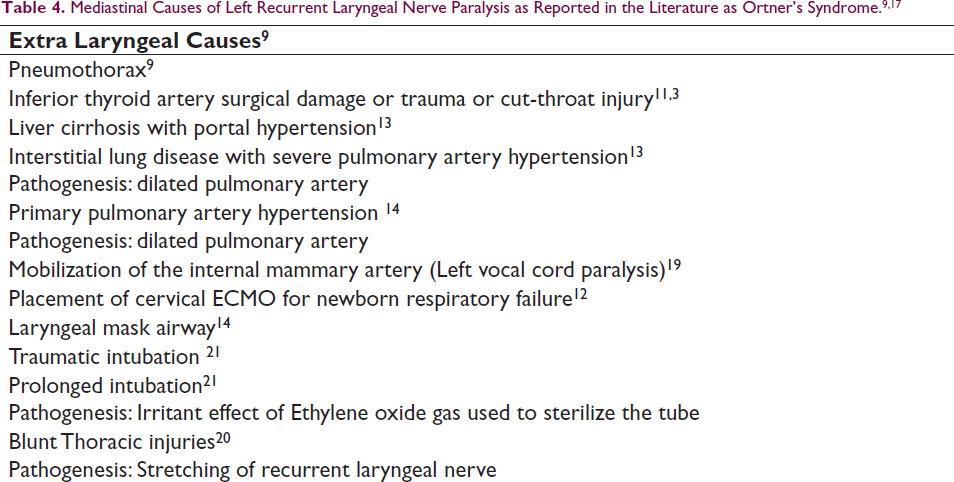
In addition to stretch and compression various mechanisms of left recurrent laryngeal nerve injury are described as follows: compression by the left main bronchus, mediastinal lymphadenitis, scar formation in the aortic window causing nerve fixity, left heart hypertrophy, atherosclerosis of pulmonary arterial system, mediastinitis, pericardial effusion, obliterative pericarditis, and pleural effusion. 16
Vocal cord paralysis as a postoperative complication of adult cardiac surgery is around 1.1%. Ortner’s syndrome may follow permanent endocardial pacemaker, trans-catheter ablation of atrial fibrillation, stenting of the left pulmonary artery, and coil closure of patent ductus arteriosus (PDA The rate of complications was around 3.5% to 5.3%, in another case series. The authors also observed that 77% of their patients showed signs of partial recovery of voice function at 4 months and full recovery was expected at 6 to 7 months. 17
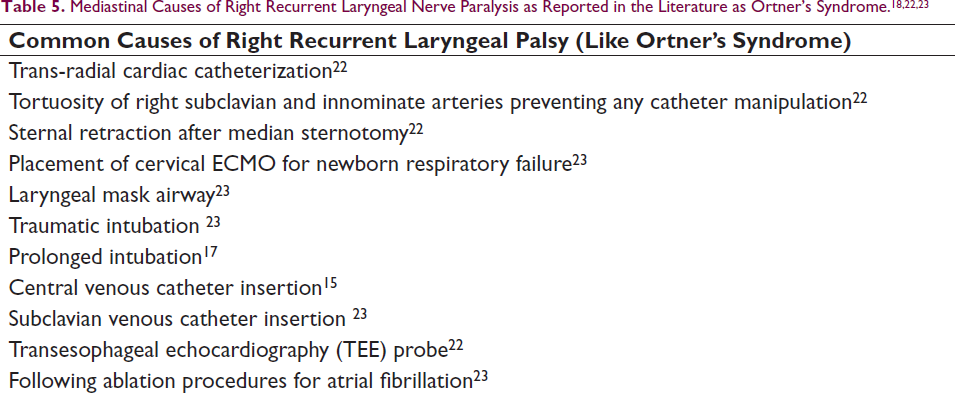
Mediastinal Causes of Right Recurrent Laryngeal Nerve Paralysis as Reported in the Literature as Ortner’s Syndrome. 9
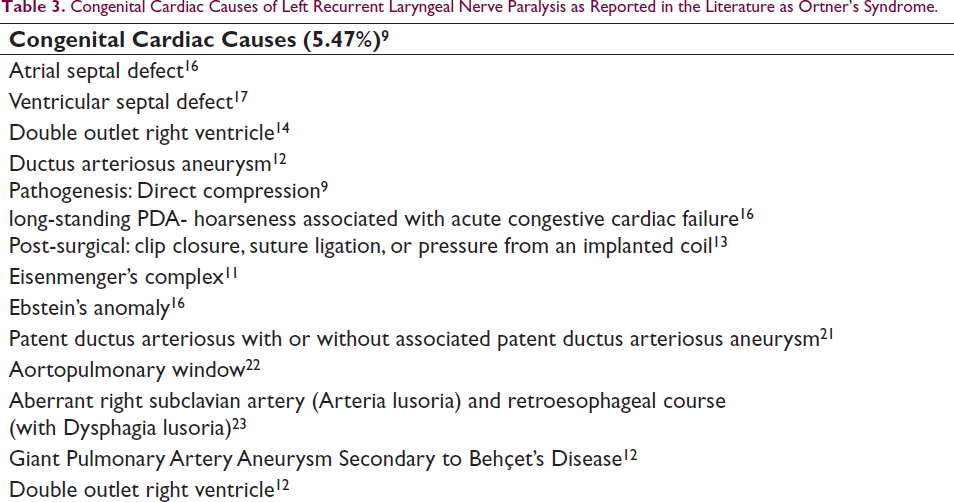
Bilateral nasogastric tube insertion has reportedly led to Cricoid-chondritis, post-cricoid ulceration, and bilateral vocal cord paralysis. Congenital cardiac causes of Left Recurrent laryngeal nerve paralysis as reported in the literature as Ortner’s syndrome listed below. 22
Congenital Cardiac Causes of Left Recurrent Laryngeal Nerve Paralysis as Reported in the Literature as Ortner’s Syndrome.
Right RLN is less common (only 30% according to some studies) and the causes of Right RLN as reported by numerous studies are as follows. 14
Course of Unilateral Vocal Fold Paralysis 23
The course of Unilateral vocal Fold Paralysis can eventually lead to 3 different outcomes2, 3:
spontaneous regaining of mobility absence of recovery but compensation by the vocal cord on the opposite side Flaccid paralysis without any evidence of recovery or compensation
24
The likelihood of recovery is highly dependent on the cause of paralysis; repeated idiopathic paralysis or surgical damage both have a favorable prognosis. Medialization laryngoplasty using silicon Implantation of the paretic vocal cord is the definitive treatment of palsy and can be undertaken if palsy shows no improvement over a considerable period. 25
Role of Laryngeal Electromyography (L-EMG)
Laryngeal electromyography (L-EMG) may be useful to evaluate the functioning of Lateral Cricoarytenoid, and Thyroarytenoid muscles, that are innervated by the recurrent laryngeal nerve. The results of L-EMG studies may provide confirmatory diagnosis and chances of spontaneous recovery. L-EMG must from performed 6 weeks to 6 months after the onset of laryngeal paresis, if any prognostic information is to be gleaned. 26
Positron Emission Tomography/Computerized Tomography Scan Findings of Left Vocal Fold Paralysis
On PET/CT scan it was noted that there was asymmetric and reduced uptake of fluorodeoxyglucose (FDG) pointing to a reduced metabolic rate of the impaired and immobile left vocal cord musculature. The left vocal cord was abducted in position and the ventricles were spacious. 27
Transcutaneous Laryngeal Ultrasonography
There are several investigations for Vocal cord paresis such as indirect laryngoscopy, direct flexible laryngoscopy (DFL), Videostrobolaryngoscopy (VL), and the novel, transcutaneous laryngeal ultrasonography (TLUSG). 28 Transcutaneous laryngeal ultrasound (TLUSG) is evolving as a non-invasive auxiliary to invasive endoscopic laryngoscopic examination for the vocal cord (VC). Male gender and older patient age are significant risk factors for non-visualization of vocal folds with TLUSG. Low-frequency probe use ensues a higher Vocal fold USG imaging rate than high-frequency probes.29, 30
Limitations
This study is a compilation of extant evidence provided by several case reports, case studies, and systematic Reviews. The condition is rare enough that a full-fledged clinical trial has not yet been reported. 31 The sample size of reported cases is less and there is considerable heterogeneity in the studies, partly due to high variability in the cause and pathogenesis of Ortner’s syndrome.
Conclusion
Cardiovocal syndrome or Ortner’s syndrome can be caused due to a myriad of etiologies in the Neck or Mediastinum. The syndrome can also be the consequence of many cardiac or mediastinal pathologies. Newer investigative modalities like Videostroboscopy and Laryngeal ultrasound are useful for early recognition of this condition which may be a harbinger of Aortic dissection or Rupture of Aneurysm leading to a fatal outcome for the patient. Cardiac physicians and Otolaryngologists must remain vigilant to the sudden onset of left vocal cord palsy as it can be an early warning sign of an ominous mediastinal pathology.
Footnotes
Data Availability Statement
The datasets generated by the current study are available under the author’s profile in the data-sharing platform online research repository Figshare.com (
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.