
Abstract
We report a case of deceleration-induced cardiac injury in a truck driver following traffic accident.Sonography revealed large pericardial effusion with tamponade. Surgical exploration showed large tear at SVC-RA junction which was repaired.Mechanism of such tear at that site is discussed.
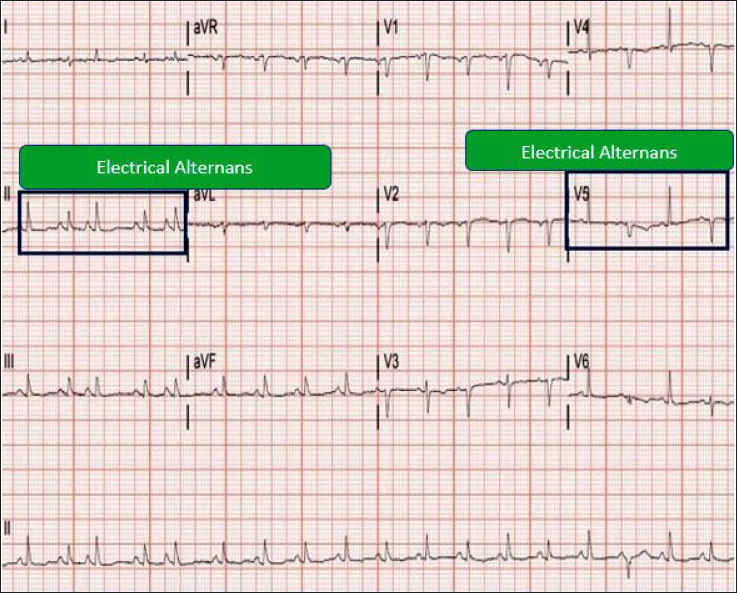
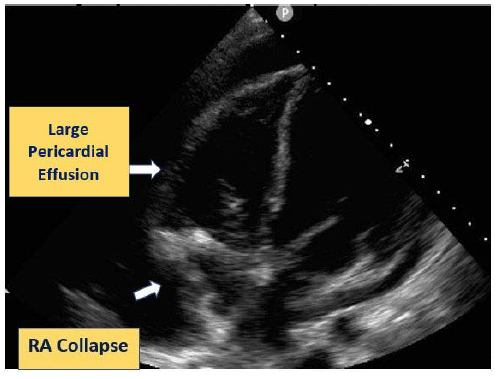
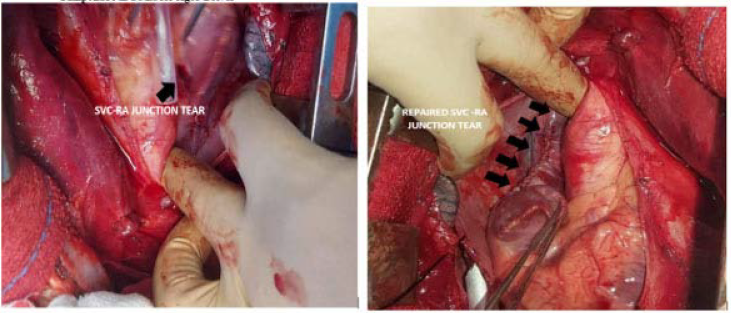
We report a rare case of deceleration-induced cardiac injury to the superior vena cavae–right atrial (SVC-RA) junction in a truck driver, following a road traffic accident. A 30-year-old male, cannabis addict, alcoholic, and obese presented to the emergency department with cardiac tamponade. He stopped the vehicle immediately while driving at 60 to 70 km per hour on the national highway to save himself from an impending head-to-head collision and sustained a blunt trauma to the chest wall from the steering wheel. At presentation, he was hypotensive with a heart rate of 130 beats per minute and blood pressure of 80/40 mmHg in the right arm supine position with SpO2 of 88%. Chest X-ray PA view revealed sternal fracture with fracture of right 3rd to 5th rib and ECG revealed electrical alternans (Figure 1). CT scan thorax revealed bilateral lung contusion with right-sided hemothorax. The Focused Assessment with Sonography in Trauma (FAST) revealed large pericardial effusion and bedside echocardiography revealed the presence of cardiac tamponade with right atrial collapse (Figure 2). He was put on oxygen therapy, aggressive fluid, and inotrope support. Intercostal chest tube drainage was inserted and he was rushed to the cardiac surgery operation theatre (OT) with suspicion of aortic isthmus injury which is the commonest form of deceleration-induced cardiac injury. 1 After midline sternotomy, a purse-string suture was put on the pericardium over the aortic root and the exposed pericardial sac revealed a large organized blood clot inside. The aortic root, ascending aorta, and isthmus were intact. Interestingly, there was a large organized clot over the SVC-RA junction and active bleeding was found underneath. This large organized clot over the SVC-RA junction tear might have prevented the patient from rapidly developing cardiac tamponade for which he was able to be shifted to the cardiac surgery OT. After exposing the pericardial sac, a longitudinal tear in the SVC-RA junction about 5 cm long extending from distal SVC to the right atrial appendage was seen. After placing a side biting hemostatic clamp, it was repaired with a double layer 5-0 prolene suture with a 17 mm needle (Figure 3). As the tear was across the sinoatrial node, a pledgeted suture was not used during the repair of this longitudinal tear. A single-layer closure of the pericardium was done. As SVC -RA junction longitudinal tear was across the area of the sinoatrial node, the patient was in Type II sinoatrial block for which a temporary epicardial pacing wire was kept in situ besides the pericardial drain. Fractures of the 3rd to 5th ribs were conservatively managed and the fractured manubrium sterni was repaired with the modified Robicsek method, ie reinforcing the sternum by 4 interlocking parasternal steel wires followed by conventional transverse sternal steel wire rib binding. The procedure was performed without cardiopulmonary bypass. Post-procedure patient was extubated after 2 hours, was without hemodynamic support and his oxygen saturation was normal. The injury in SVC-RA junction is attributed to abrupt deceleration injury as there were undisplaced fractures at the right costochondral junction corresponding to the SVC-RA junction. If those fractures would have been displaced fractures, the tip of the fractured ribs would have caused penetrating injury to the SVC-RA junction. Additionally, intraoperatively there was no pericardial injury to support penetrating injury to SVC-RA junction by the fractured ribs. Our case is the first case report of a deceleration-induced SVC-RA junction longitudinal tear presenting as cardiac tamponade. Deceleration thoracic aortic injuries commonly occur with high- speed motor vehicles with speed more than 100 km/hr. Blunt aortic injury occurs after sudden deceleration and tearing of the aorta most commonly occurs at the transition from the mobile segment to the fixed segment, ie aortic isthmus distal to the origin of the left subclavian artery. SVC is fixed to the mediastinum and right atrium is highly mobile. Hence, SVC- RA junction behaves as a hinge point like aortic isthmus during deceleration cardiac injury. Abrupt deceleration induced shear traction at the SVC-RA junction hinge point may have resulted in tear. A landmark study by Parmley et al 2 described 45% of those blunt thoracic aortic injuries occurring at this location. Shear forces and stretching of the aorta are the most likely mechanisms of deceleration-induced vascular injury. “Pinch injury” in which the aorta is violently compressed by the first rib also occurs. 3 Deceleration injury involves rupture of the inner intimal and medial layers followed by delayed adventitial rupture. Similar mechanism along with hyperextension and traction on blood vessels 4 operates in the injury of nonaortic great vessels as demonstrated in our case in which SVC-RA junction hinge point may have sustained significant shear stress and might have been ruptured. Thoracic blunt trauma may lead to vessel avulsion in which the patient may die before reaching the hospital 5 or the patient may not survive the operation.6,7 In less severe cases, blunt thoracic trauma results in arterial wall disruption and pseudo aneurysm formation which may remain asymptomatic for a long period. 8 Innominate and left carotid artery injuries most commonly occur proximally,9,10 whereas most of the subclavian artery injuries are distal.11,12 Nwaejike et al 13 described deceleration induced right inferior pulmonary vein injury extending up to the right superior pulmonary vein which was successfully repaired under cardiopulmonary bypass. The paradoxical aspect of deceleration induced pulmonary vein injury is that patient remains deceptively stable after pulmonary vein injury as low pressure left atrium and pulmonary vein contribute towards development of a low pressure hemothorax which effectively functions as a giant left atrium allowing maintenance of hemodynamics. 14 Walsh et al 15 described an azygous vein laceration following a vertical deceleration injury. Although the aortic isthmus is the commonest site among deceleration-induced cardiac injuries, it can happen anywhere. Even the SVC-RA junction can have a large tear, which if managed in time can save the patient from an impending doom. Early suspicion of vascular injuries with aggressive fluid resuscitation and immediate surgical intervention remains the only clue for survival from such lethal injuries.
ECG Showing Electrical Alternans.
Echocardiography Showing Features of Cardiac Tamponade.
Superior Vena Cavae–Right Atrium Junction Tear.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.